Article Text

Abstract
The assumed minimum walking speed at pedestrian crossings is 1.2 m/s. In this prospective cohort study, usual walking speed was measured over a 4 m course in 926 community-dwelling, ambulatory patients with stable COPD. Mean (SD) walking speed was 0.91 (0.24) m/s with only 10.7% walking at a speed equal or greater than 1.2 m/s. In order for 95% of this cohort to safely negotiate a pedestrian cross, traffic lights would have to assume a minimum walking speed of 0.50 m/s (2.4 times longer than current times). The current assumed normal walking speed for pedestrian crossings is inappropriate for patients with COPD.
The studies were registered on clinicaltrials.gov and these data relate to the pre-results stage: NCT01649193, NCT01515709 and NCT01507415.
- COPD ÀÜ Mechanisms
Statistics from Altmetric.com
Introduction
In many countries, including the USA,1 Canada,2 Ireland,3 South Africa4 and the UK,5 pedestrian crossings assume a minimum walking speed of 1.2 m/s—equivalent to 4 ft/s.5 Recent epidemiological studies have shown a significant proportion of older adults in the UK and Ireland walk slower than 1.2 m/s, while more than half of all pedestrians killed on the road are over 65 years of age despite this age group representing <20% of the population.6 With an ageing population, there are concerns that insufficient time to negotiate pedestrian crossings safely will become an increasing public health problem.6
Patients with COPD, in whom exertion-related breathlessness and exercise intolerance are common, may be particularly vulnerable. The aim of our study was to assess normal walking speed in a cohort of community-dwelling, ambulatory patients with stable COPD. We hypothesised that only a small minority of patients with stable COPD would have walking speeds greater than 1.2 m/s.
Methods
This was a prospective cohort study and data were collected between November 2009 and October 2013 in patients recruited from community-based and hospital-based respiratory and pulmonary rehabilitation clinics at Harefield Hospital, UK. Inclusion criteria included a diagnosis of COPD according to Global Initiative for Chronic Obstructive Lung Disease guidelines, ambulatory (defined as leaving the house at least once a week and able to walk 10 m independently) and stable disease (no change in medications in previous 6 weeks). All participants provided informed consent and the London Camberwell-St. Giles (11/LO/1780) and West London (11/H0707/2) Research Ethics Committees approved the study. Usual walking speed was measured as the 4 m gait speed (4MGS) with a standing start as previously described.7–10 Other measurements recorded included FEV1, the Medical Research Council dyspnoea scale (MRC) and the incremental shuttle walk test (ISW).
Results
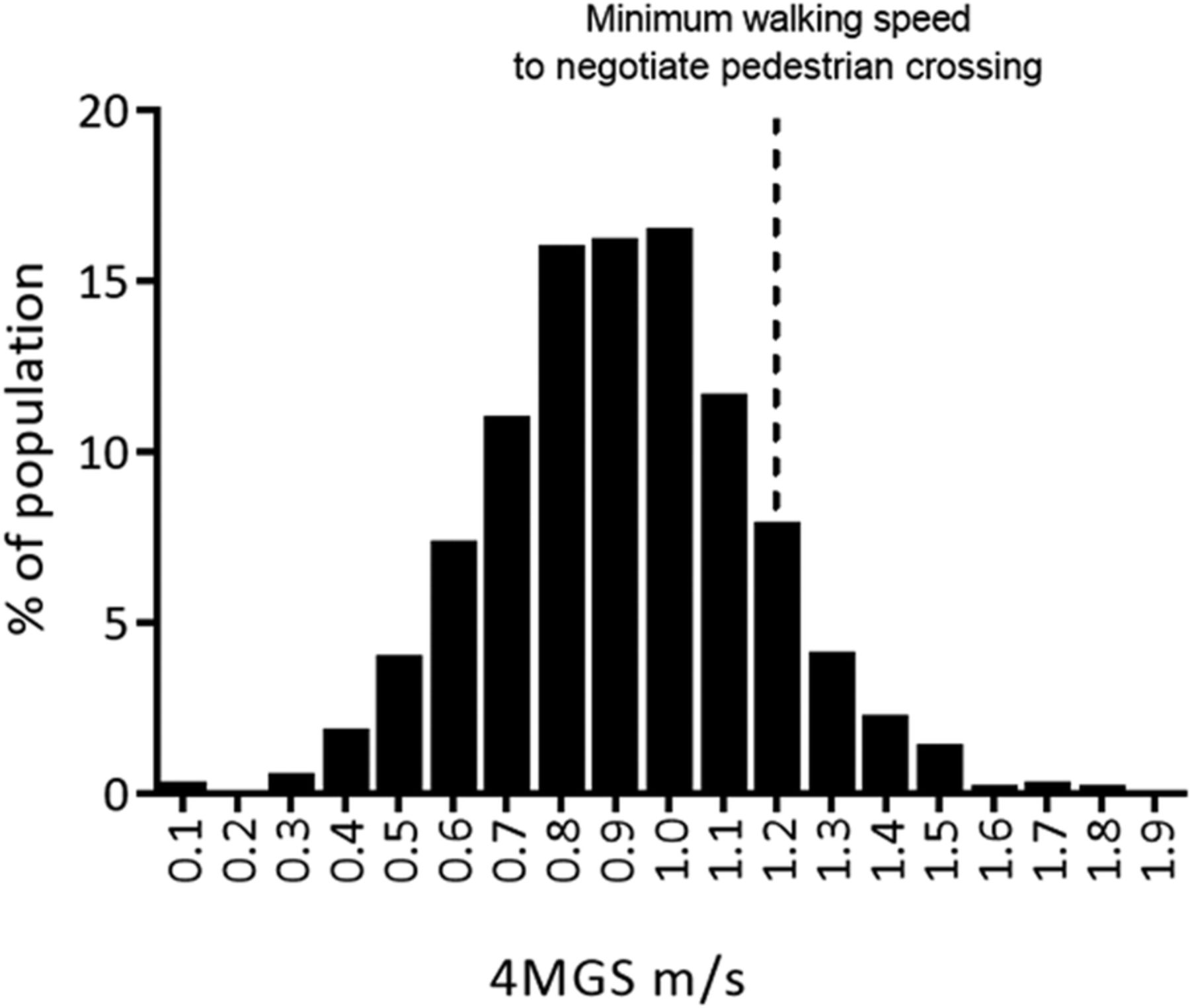
We asked 973 patients to consider participating in the study: 38 declined to participate (n=15: family commitments, n=10: not interested in research, n=9: no reason provided, n=4: miscellaneous reasons) and 9 did not meet the study inclusion criteria (n=6: recent change in medication, n=3: unable to walk 10 m). Data were available in 926 patients (548 men; 378 women). Baseline characteristics were expressed as mean (SD): age 69 (10) years, FEV1 49.8 (20.9) %, MRC 3.3 (1.1), ISW 223 (150) m and 4MGS 0.91 (0.24) m/s. Fifty-five per cent, 32% and 14% had concomitant hypertension /cardiovascular disease, obesity and osteoarthritis, respectively, while 5% used ambulatory oxygen. 4MGS was weakly associated with age (r=−0.21), FEV1%predicted (r=0.11), moderately with respiratory disability (MRC: r=−0.51) and strongly with exercise capacity (ISW: r=0.78); all p<0.001. Frequency distribution of 4MGS for the cohort is shown in figure 1, demonstrating that only 10.7% had a walking speed equal to or greater than 1.2 m/s.

{kind=link}
Frequency histogram of 4 m gait speed (4MGS) in a cohort of 926 ambulatory patients with stable COPD. Dotted line indicates the minimum walking speed assumed by pedestrian crossings (1.2 m/s).
Discussion
Our cohort of ambulatory patients with stable COPD had significantly slower walking speeds than previously reported in age-matched healthy people (mean (95% CI)), males: 1.4 (1.27 to 1.41) m/s; females: 1.24 (1.18 to 1.30) m/s),11 but were faster than those at discharge following a hospitalised acute exacerbation of COPD (mean (SD) 0.61 (0.26) m/s).9 Slow walking speed was associated with increasing respiratory disability (MRC) and decreased exercise tolerance (ISW).8
UK pedestrian crossing timings assume a minimum walking speed of 1.2 m/s, yet only 10.7% of our cohort with stable COPD would have sufficient time to walk across a pedestrian crossing safely. In order to accommodate at least 95% of our cohort, pedestrian crossings would have to assume a minimum walking speed of 0.50 m/s, resulting in traffic lights having to stay red 2.4 times longer than current times.
A limitation of the study is that gait speed measurements were carried out indoors, on a flat undisturbed 4 m walking course in a controlled outpatient setting. This may not reflect real-life conditions at pedestrian crossings such as the weather, road and pavement surface quality, varying walk distances, interactions with other pedestrians and driver behaviour. Therefore, it is possible that our gait-speed measurement actually overestimates real-life walking speed at a pedestrian crossing. In contrast, it could also be argued that with the visual or auditory feedback at a pedestrian crossing, patients with COPD and a degree of functional reserve may adopt a walking speed closer to maximum, rather than usual, gait speed.
Further work is required to assess whether the discrepancy between pedestrian crossing times and patients' walking speed may influence engagement in physical activity, a significant modifiable prognostic risk factor.12 Patients with COPD have limitations in every aspect of daily life and inability to negotiate the local environment may deter patients from engaging in physical or social activities outside their home. Indirect evidence to support this includes the previously described association between slow gait speed and reduced objectively measured physical activity levels in outpatients with COPD.13 Our data would support an evaluation of solutions to improve pedestrian safety particularly in people with COPD, including extended pushbuttons, countdown timers and pedestrian infrared detectors as well as the use of technology to allow variable pedestrian crossing times based on local factors such as weather and traffic.
In summary, approximately 90% of stable outpatients with COPD have a usual walking speed below the minimum walking speed assumed by pedestrian crossings. Currently, assumed normal walking speed for pedestrian crossings is inappropriate for patients with COPD.
Acknowledgments
The authors thank the patients for their participation in this study.
Footnotes
Contributors CNM and SSCK contributed equally to this study. WD-CM, SSCK, MM: substantial contributions to the conception and design of the study; CMN, SSCK, SP, SEJ, REB: substantial contribution to the acquisition of data; CMN, SSCK, MIP, MM, WM: analysis and interpretation of the data; CMN, SSCK, MIP, MM, WD-CM: first draft of the manuscript; All authors: revision of the manuscript critically for important intellectual content, approval of the final manuscript; CMN, SSCK, WD-CM: accountability for all aspects of the work.
Funding This work was supported by a Medical Research Council (UK) New Investigator Research Grant (G1002113/98576) awarded to WD-CM.
Competing interests This work was supported by a Medical Research Council (UK) New Investigator Research Grant (G1002113/98576) awarded to WD-CM, who was also supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Northwest London. CMN and SEJ are supported by NIHR Doctoral Research Fellowships. MM is supported by NIHR CLAHRC for South London. The views expressed in this publication are those of the authors and not necessarily those of the Medical Research Council, the NHS, the National Institute for Health Research or the Department of Health.
Ethics approval West London and London Dulwich Research Ethics Committees.
Provenance and peer review Not commissioned; externally peer reviewed.