Article Text

Statistics from Altmetric.com
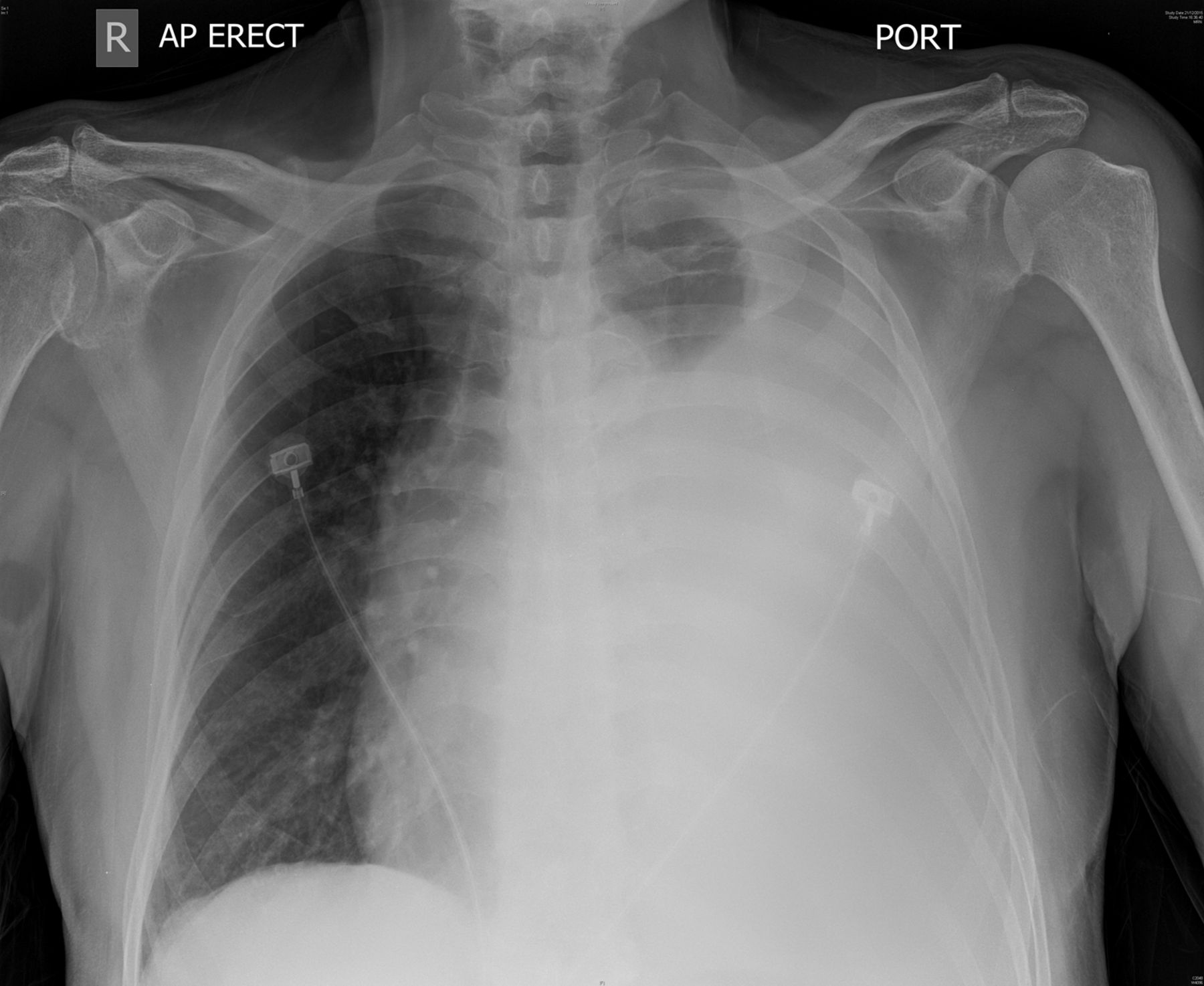
A 74-year-old man presented with cough of 3 weeks' duration. Chest X-ray showed a large left-sided pleural effusion (figure 1) that was a lymphocytic exudate with normal adenosine deaminase level, and negative bacterial and mycobacterial cultures. Flexi-rigid pleuroscopy (LTF 160, Olympus, Japan) revealed candle-wax fibrotic parietal pleura (figure 2), which was sampled using the flexible forceps (FB-55CD-1, Olympus, Japan) with cusps measuring 2.4 mm when fully open, and a cryoprobe of 2.4 mm in diameter (20416-032, Erbokryo CA, Erbe, Germany). The cryoprobe was directed to the target area and 4-second freeze time was applied. The pleuroscope and cryoprobe with the pleural specimen attached to the frozen tip were removed en bloc through the trocar. The tissue was retrieved by thawing in normal saline. Cryobiopsies revealed sarcomatoid malignant mesothelioma while those obtained with forceps were non-diagnostic (figure 3).

Left large effusion with normal mediastinum.
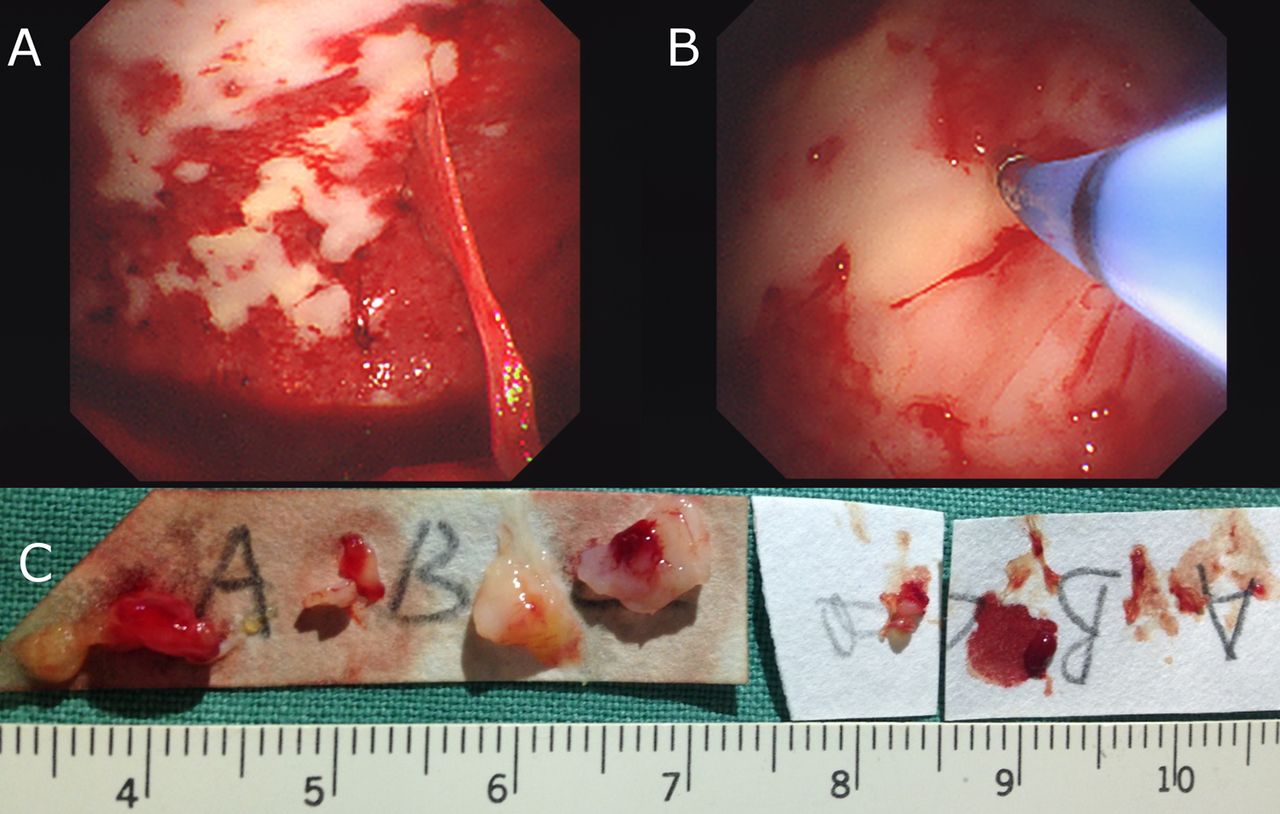
(A) Candle wax parietal pleural abnormalities; (B) cryoprobe biopsy of target area; (C) size of pleural biopsies (left: cryoprobe; right: forceps).

{kind=link}
{kind=link}
{kind=link}
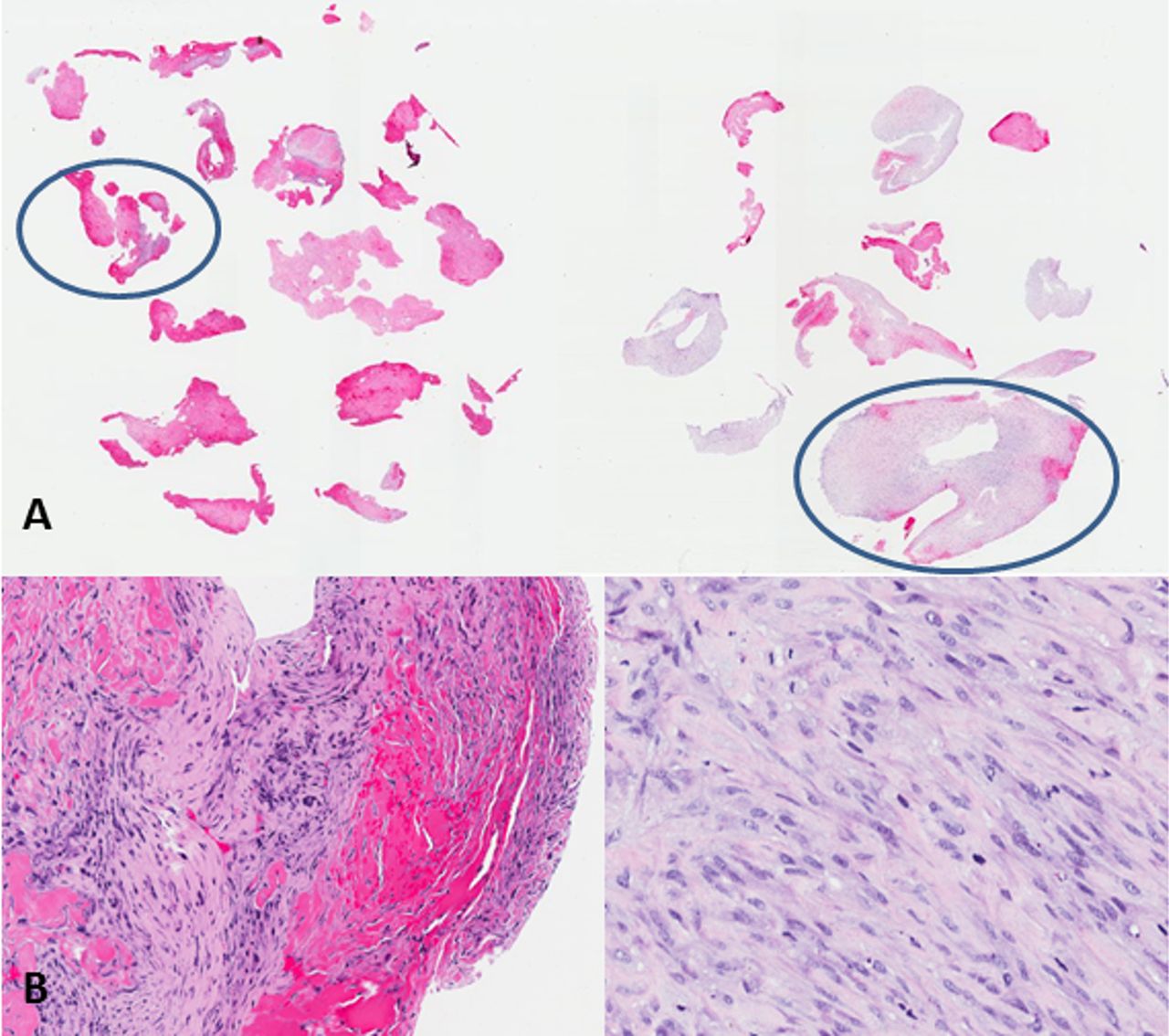
(A) Pleuroscopic forceps biopsies (left) and cryobiopsies (right). Forceps specimens demonstrated predominantly pink-staining surface exudate while thickened pleura was more clearly appreciated in cryobiopsies. (B) Pink-staining fibrin and layered reactive fibroblasts were observed in forceps specimen while cryobiopsy harboured malignant spindle cell tumour (×20 original magnification of specimens circled in A).
Diagnosis of mesothelioma can be challenging for early or sarcomatoid subtype as sampling site, technique and instrument can lead to false-negative histology, especially if biopsy samples are of inadequate depth. This arises from the need to fit the forceps through a small working channel of the pleuroscope, thereby limiting the size of the forceps and its mechanical strength in obtaining deep biopsies. Physicians advocate minithoracotomy, video-assisted thoracoscopic surgery (VATS) or insulated-tip knife to procure pleural specimens, which confer diagnostic accuracy ranging from 74–100%.1–3 Grossebner et al1 demonstrated that VATS biopsy achieved 100% histology diagnosis but led to increased hospitalisation stay due to prolonged air leak. Kao et al2 reported that thoracotomy was superior over VATS in achieving accurate subtype classification (83% vs 74%). Nonetheless, flex-rigid pleuroscopy performed under local anaesthesia remains an attractive diagnostic modality and two small studies have demonstrated excellent safety in obtaining pleural specimens using the flexible cryoprobe (table 1).4 ,5
Comparison of studies looking at the use of thoracoscopic cryobiopsy of the pleura
Our report describes sarcomatoid malignant mesothelioma diagnosed by pleuroscopic cryobiopsy where corresponding specimens with standard forceps were negative. The cryobiopsies were larger and of sufficient depth with better-preserved architecture compared with those obtained by the flexible forceps. While cryobiopsy is not routinely performed during pleuroscopy, this case highlights its potential role when smooth, fibrotic pleura is encountered.
Footnotes
Contributors H-PC and PL were involved in the pleuroscopic biopsy and writing up of the manuscript. M-FL was involved with the radiology and the writing up of the manuscript. J-ES was involved in analysis of the histology and writing up of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.