Article Text

Abstract
Introduction Endobronchial lung volume reduction with one-way valves (ELVR), in combination with staged unilateral VATS lung volume reduction surgery (LVRS), multiplicates the options of treatment for emphysema. No experience has yet been reported in literature of the use of LVRS after failure of ELVR. We aimed therefore to review our current series.
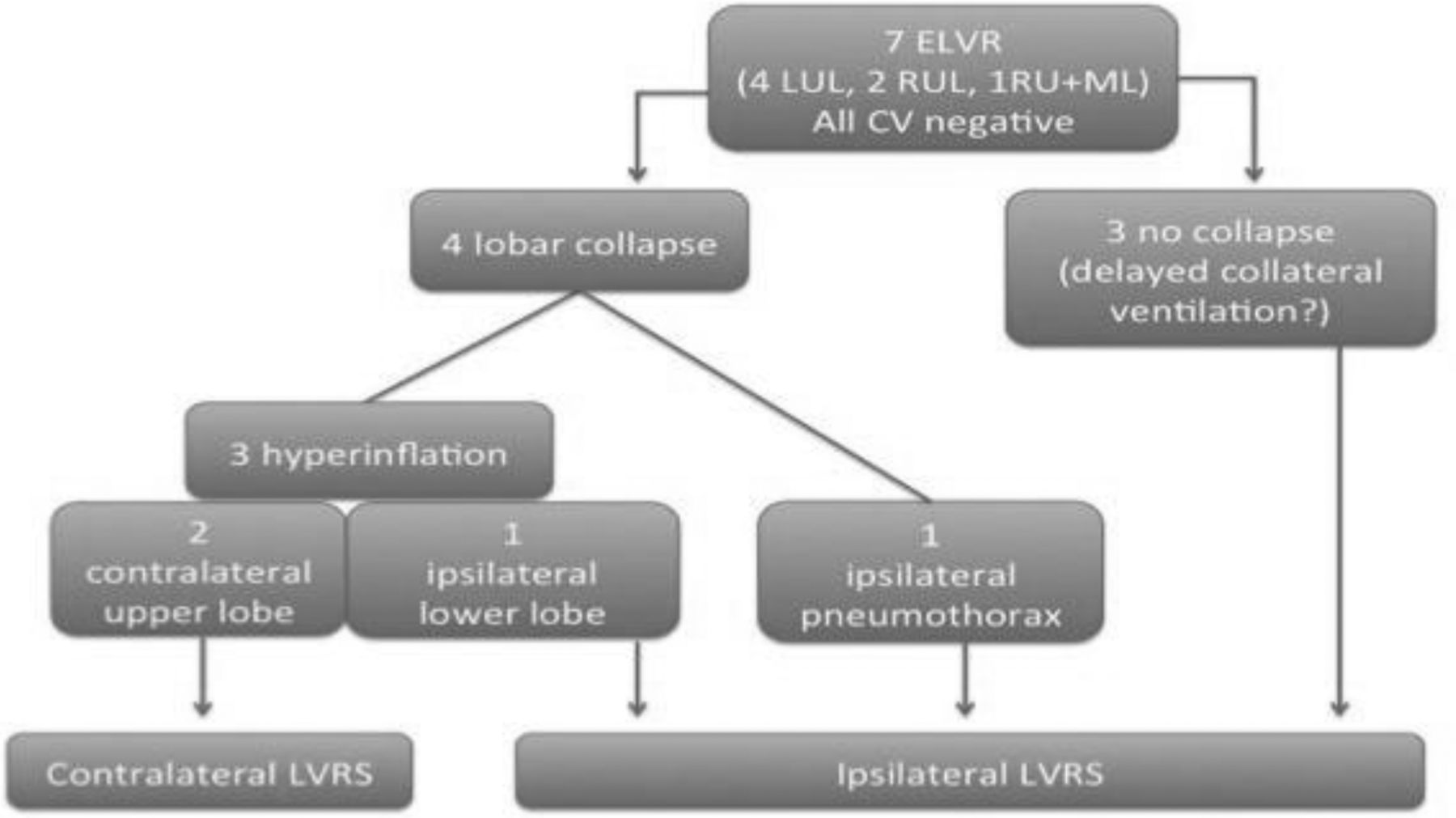
Methods 7 consecutive patients (3 male, age 68, 59–76) had successfull Chartis assessment and ELVR, and subsequently underwent salvage LVRS following failure or complications of primary procedure. All patients were suitable candidates for either approach according to our criteria (average RV/TLC 67 range 56–77, FEV1 32% range 25–38, DLCO 32%, range 24–55), with 4 patients classifying as moderate to high risk for LVRS and the rest as moderate or low. They were offered both options and opted for ELVR on the assumption of reduced risks and shorter hospitalisation. Valves were not removed prior to LVRS, except in one case who was also the first chronological patient in our series.
Results Delayed collateral ventilation with no lobar collapse and no functional improvement at any time was observed in 3 patients. The remainder had lobar collapse with initial improvement: of these, 1 developed ipsilateral pneumothorax with persisting air leak leading to LVRS, 2 developed contralateral upper lobe compensatory hyperinflation (1R, 1L) and 1 ipsilateral lower lobe compensatory hyperinflation.
No significant morbidity or 30-day/in-hospital mortality. Median lenght of stay after LVRS was 11 days (4–34), slightly longer (19 days, 4–34) for patients who were operated for contralateral hyperinflation or whose EBV was removed prior to VATS (no valve in situ on the operated side). Duration of drainage was also longer in these patients compared to the whole group, 18 (6–30) vs. 8 (5–30) days. Average EQ-5D score was 49.7 (18.9–71) six months after LVRS, vs. 42 (18.9–81.4) preoperatively, with only one patient reporting further deterioration.
Conclusion ELVR can be considered as a trial of LVR not precluding salvage LVRS. Removal of endobronchial valves prior to surgery seems unnecessary and may actually be protective against excessive postoperative air leak. Occurrence of compensatory hyperinflation may suggest that single-stage bilateral ELVR could also be considered.
{kind=link}