Article Text

Statistics from Altmetric.com
A 69-year-old man was admitted to our hospital with progressive dyspnoea accompanied by inspiratory stridor. He presented a history of surgical aortic valve replacement 3 years previously, complicated by prolonged postoperative mechanical ventilation requiring percutaneous tracheostomy. Presently, bronchoscopy evidenced tracheomalacia (TM) with subtotal tracheal stenosis. CT scan confirmed long segment narrowing >20 mm of the upper trachea (figure 1). Operative retracheostomy resulted in repeated tube dislocation incl. necessity for cardiopulmonary resuscitation. As cardiac comordities additionally impeded extensive surgical repair, insertion of an uncovered, self-expanding nitinol stent (stent diameter: 18 mm, stent length: 40 mm, individually manufactured by Leufen Medical GmbH, Berlin, Germany) was performed (figure 2, left). No intraprocedural complications occurred post stent deployment. For 2 years by now, clinical and bronchoscopic patient follow-up revealed durable adequate stent expansion and stenting of the upper trachea (figure 2, right).

CT scan images in coronal (A) and axial (B) projection showing 20 mm subtotal stenosis of the upper trachea.
{kind=link}
{kind=link}
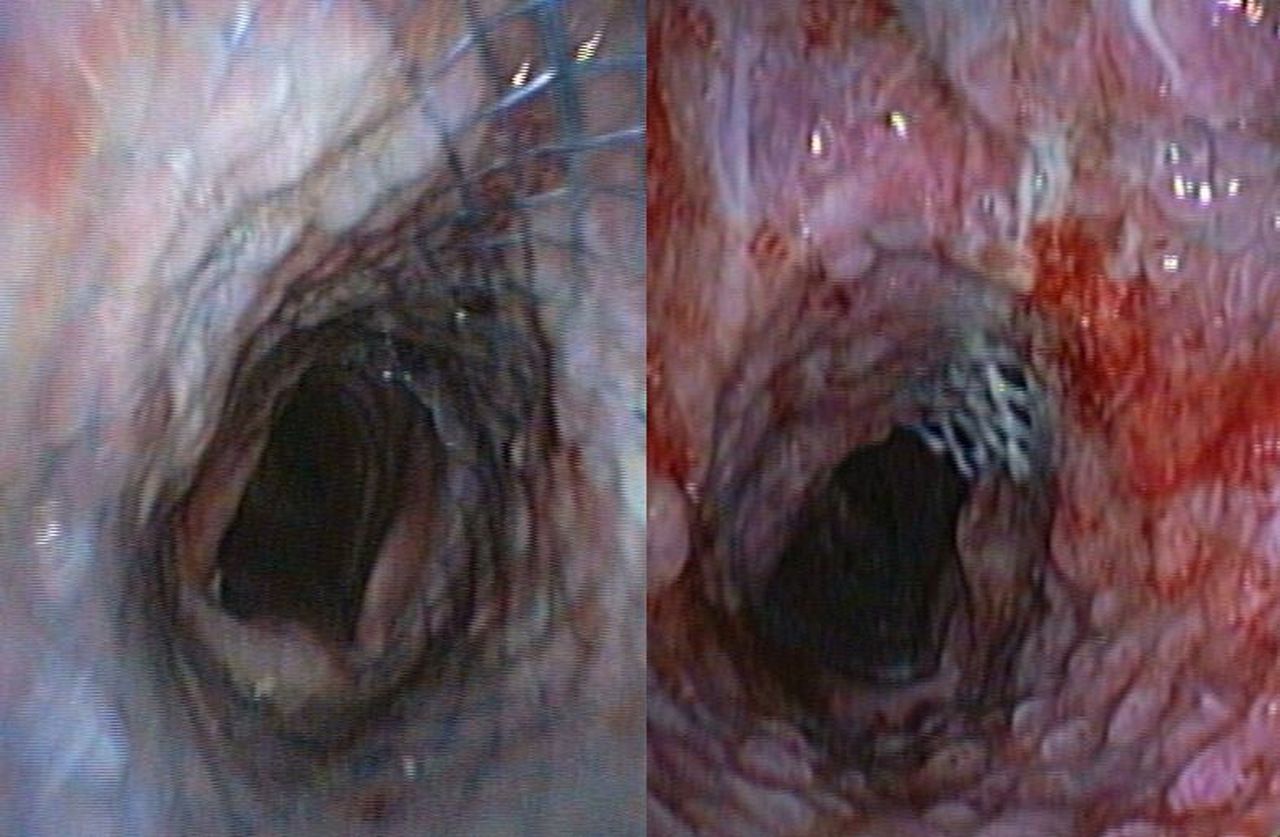
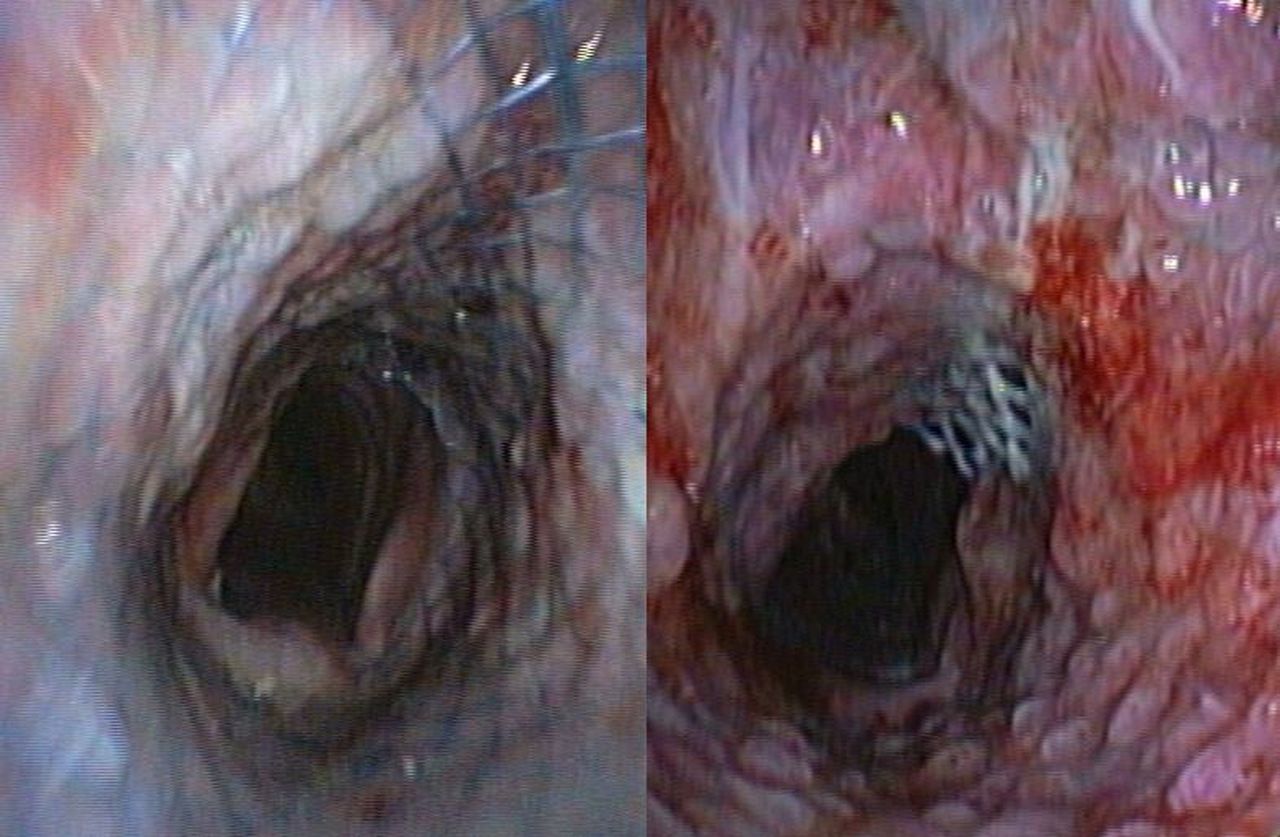
Endotracheal imaging during bronchoscopy on the day following nitinol stent implantation (left) and 25 months thereafter (right). Though formation of granulation tissue has meanwhile occurred, tracheomalacia-driven tracheal renarrowing is persistently prevented.
TM is a condition characterised by excessive diffuse or segmental tracheal collapsibility that can be classified as congenital or acquired. Among the latter, tracheostomy may provoke tracheal cartilage injury and thereby induce TM. As to the scarce therapeutic approaches in symptomatic TM, insertion of silicone stents is preferentially employed, though stent-related complications like migration, plugging or formation of granulation tissue are frequent.1 In contrast, metal stents are currently not recommended for alleviation of benign tracheal narrowing due to their potential risk of breakage. However, we presently report sustained efficiency of airway stabilisation by long-term nitinol stenting that might evolve into an equivalent treatment option in TM.
Reference
Footnotes
Contributors CP, DD, GN and DS drafted, conducted and coreported this article.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.