Article Text

Abstract
Objective Postural stability depends on the coordination of the central nervous system with visual sense, proprioceptive and vestibular information. Sleep deprivation has been shown to affect this function. The objective of our study was to assess the effects of sleep-disordered breathing (SDB) on postural stability.
Methods 158 subjects referred for suspected SDB had an overnight sleep study and were placed on a posturographic platform in late afternoon. This platform allows measuring the centre of pressure (CoP) oscillations and to calculate: total displacement of CoP in X and Y axes, mean speed of CoP displacement and the length as function of surface (LFS) ratio (length of CoP displacement/surface of CoP trajectory).
Results 98 men and 60 women were included. Mean age±SD was 45.4±5.5 years old, body mass index (BMI) 27.5±5.6 kg/m2 and apnoea–hypopnoea index (AHI) 13.6±16.1/h. AHI was <5/h in 64 (41%) subjects, 5–15/h in 43 (27%), 15–30/h in 30 (19%) and >30/h in 21 (13%). In patients with an AHI >5/h versus AHI <5/h, we observed an important increase in LFS (+21%, p<0.001), in XY length (+23%, p<0.001) and in mean speed (+23%, p<0.001). After controlling for age, BMI and sleepiness (Epworth) in multivariate regression models, there was a positive association between all nocturnal breathing parameters (specifically: mean SpO2, AHI, oxygen desaturation index 3% and % time with SpO2 <90%) and the main stability outcomes (all p<0.05).
Conclusions SDB severity, especially the mean nocturnal SpO2 level, is associated with impaired daytime postural stability.
- Sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
Is sleep-disordered breathing associated with impaired postural stability?
What is the bottom line?
There is an independent association between nocturnal breathing disorders parameters, especially the apnoea–hypopnoea index and nocturnal oxygen level and impaired postural stability.
Why read on?
This study analyses the determinants of postural instability in patients with sleep-disordered breathing and the possible pathophysiological mechanisms, which may be responsible for this association.
Introduction
Sleep-disordered breathing (SDB) is a disabling condition caused by repeated episodes of upper airway obstruction during sleep, resulting in nocturnal hypoxaemia and fragmented sleep.1 Moreover, this condition is associated with an increased risk of hypertension, stroke, heart failure, diabetes, car accidents and depression.2–10 SDB has also been shown to alter reaction time and reflexes while driving with an improvement after SDB treatment.11
Postural stability is an important function of the human body.12 The body postural control depends on the coordination of the central nervous system with visual sense, proprioceptive and vestibular information to control the effector organs (skeletal muscles of the legs, gait and trunk). Any alteration in these integrative processes will negatively influence postural control.13 In a healthy individual, central nervous system uses small-amplitude postural oscillations to keep the body close to vertical alignment.14 The bipedal control of posture has primarily been studied by analysing the trajectory of the centre of pressure (CoP), which can be easily recorded using posturographic platforms.15
It has been shown that balance and gait impairments in older people increase the risk of falls, which is the leading cause of accidental death and injury-related visits to emergency departments.16 Postural control is the foundation of our ability to stand and to walk independently. Deterioration of postural stability in patients with SDB may contribute to falls occurring during activities of daily life, in particular among older patients.
It has also been shown that postural stability is affected by >19, 24 or 48 h sleep deprivation.17–20 The negative effects of sleep deprivation on postural sway seem to be due to the reduced levels of alertness19 and peaks when the body temperature reaches its minimum.20 After a night of sleep deprivation, the bilateral posterior-parietal and prefrontal areas are less activated,21 ,22 thereby prompting an alteration in sensorimotor integration.
Another factor that can affect postural stability is hypoxia. Recently, Degache et al23 showed that short exposure to hypobaric hypoxia at an altitude of 1700 and 3000 m could deteriorate the postural control. Moreover, in normobaric hypoxia condition, significant disturbances of postural stability were observed when blood oxygen saturation level (SpO2) decreased to 70% during 10 min by breathing hypoxic gas (FIO2: 6%–10%).24
Considering the decreased sleep quality and repeated oxygen saturation drops observed in SDB, we sought to test the hypothesis that daytime postural control could be impaired in patients with SDB compared with control subjects.
Material and method
Population
Subjects were recruited among consecutive patients referred to the Lausanne University Sleep Centre for suspected SDB and were informed about the protocol by post mail prior to the sleep study. Inclusion criteria were age ≥18 years and ability to give an informed consent. Exclusion criteria were the presence of a neurodegenerative disease, peripheral neuropathy, pregnancy (shift of the gravity centre), spinal or lower limb disease, inner ear disease affecting stability, any medication affecting the central nervous system and chronic alcohol consumption. Those who fulfilled these criteria were included in the study and had a stabilometry testing in the late afternoon before the sleep study.
This study was approved by the Cantonal Ethics Committee of Lausanne, Switzerland (# 474/12). All subjects provided written, voluntary, informed consent prior to participation. The experiment was conducted according to the Declaration of Helsinki.
Postural stability protocol
A posturographic platform (Fusyo-Medicapteur, Toulouse, France; Dekra certification) with a sampling rate of 40 Hz was used for postural stability assessment (figure 1). CoP excursion data were recorded using a PC computer with Fusyo software V.1.2.1. The posturographic platform measured 530 mm×460 mm×35 mm and was equipped with three pressure gauges (hysteresis <0.2%). Signal processing was accomplished using a 16-bit A/D converter at 40 Hz.25 The duration of each test was 51.2 s, resulting in a 2048-point time series.

Posturographic platform (Fusyo-Medicapteur, Toulouse, France; Dekra certification).
The subjects were placed on the posturographic platform (figure 1) using precise markers (figure 2). Their legs were extended, and their feet formed a 30° angle relative to each other with an intermalleolar distance of 5 cm. The subjects were instructed to maintain their balance, while looking at a fixed target at a distance of 90 cm with their arms at their sides and to look straight ahead. The height of the visual target was adjusted for each subject. The verbal instructions were as follows: ‘Stand with your arms at your sides and look straight ahead while trying to maintain your postural stability to your best ability’. The aim of these instructions was to limit their sway as much as possible.

Positioning of feet on posturographic platform during postural control analysis in (A) a subject with no sleep-disordered breathing (SDB) (apnoea–hypopnoea index (AHI)=3/h) and in (B) a patient with SDB (AHI=20/h). CoP, centre of pressure.
Data acquisition and analyses
CoP oscillations were collected and allowed calculating the standard postural sway parameters: (1) total displacement of CoP in anteroposterior (Y axis) and mediolateral (X axis) plan (length in mm); (2) mean speed of CoP displacement (mm/s) and (3) LFS ratio corresponding to the length of the CoP displacement as a function of the surface of CoP trajectory (index of energy expenditure).26
Sleep recordings
Subjects were equipped with a type 3 ambulatory limited channel recorder Embletta system (Embla Systems, Broomfield, Colorado, USA) at the sleep lab in the afternoon by a trained sleep technician. This device records nasal air pressure, thoracic and abdominal movements, oxygen saturation (SpO2) level, heart rate and body position. The subjects slept at home and brought the recorder back to our sleep lab the next morning.
All sleep recordings were manually scored by a trained physician (SV) using Somnologica software V.5.1.1 (Embla Flaga, Reykjavik, Iceland) and reviewed by a second physician (RH or JHR). Apnoea was defined as a 90% of airflow drop from baseline lasting 10 s or longer. Hypopnoea was defined as a ≥30% drop of airflow signal lasting at least 10 s or longer with a ≥3% oxygen desaturation. The average number of apnoea and hypopnoea per hour (apnoea–hypopnoea index (AHI)) was calculated. AHI was divided into the standard categories (normal <5/h, mild SDB 5–15/h, moderate SDB 15.1–30/h and severe SDB >30/h). The oxygen desaturation index (ODI) corresponding to the number of 3% oxygen drops per hour as well as the mean oxygen saturation level and % of the night with an oxygen saturation below 90% were also calculated. Daytime sleepiness was assessed using the Epworth Sleepiness Scale (ESS).27 A score >10/24 was considered abnormal.
Statistical analyses
All data presented in the text, tables and figures are the mean value±SD unless otherwise specified. Comparisons between subjects with and without SDB were performed with Student's t tests or Mann–Whitney tests when the data were not normally distributed. Correlations were performed using Spearman tests. Linear regression models were used to estimate the association between SDB parameters and postural stability with sleep variables used as independent variables and postural variables as dependent variables. The N for this analysis was 138 due to missing Epworth scores. A Fisher's exact test was used to compare proportional data between groups. The significance level was set at p<0.05. Statistical analysis was performed using biomedical software MedCalc for Windows V.11.4.2.0.
Results
A total of 158 patients (98 men and 60 women) fulfilled the inclusion criteria and agreed to participate (figure 3). Characteristics of these patients are described in table 1.
Anthropometric and sleep characteristics of the total population (n=158) and in no-SDB group (n=94) and SDB group (n=64)

Patients flow chart. SDB, sleep-disordered breathing.
Mean AHI was 13.6±16.1/h. AHI was <5/h (no SDB) in 65 (41%) of the patients (controls), 43 (27%) had mild (AHI 5–15/h), 30 (19%) had moderate (AHI 15–30) and 21 (13%) had severe SDB (AHI >30/h). Overall, subjects with an AHI ≥5/h were older (Δ 11.3 years), and had a higher body mass index (BMI, Δ+ 2.3 kg/m2).
Main postural parameters are described in table 2. In patients with SDB (AHI ≥5/h) compared with non-SDB patients (AHI <5/h), we observed higher LFS (+21%, p<0.001), greater XY length (+23%, p<0.001) and a higher mean speed (+23%, p<0.001). The same was found for X length alone (259 vs 301 mm, p<0.05) and for Y length alone (357 vs 459 mm, p<0.001). There was no significant difference in the stability parameters between men and women in our study (results not shown).
Postural stability characteristics of the total population (n=158) and in no-SDB group (n=94) and SDB group (n=64)
LFS, XY length and mean speed were all significantly correlated with SDB parameters such as the AHI, the ODI, the mean nocturnal SpO2 and the % of the night spent with and SpO2 <90%. When the main confounding factors (age, sleepiness and BMI) (table 3) were included in a linear regression model there was still an independent association between AHI, ODI, mean nocturnal SpO2, time with SpO2 <90 and LFS, XY length and mean speed. There was also a negative independent association between mean nocturnal SpO2 and the postural stability parameters (figure 4). However, no significant association was found between subjective daytime sleepiness measured by the ESS and postural stability parameters.
Association between SDB parameters and postural stability outcomes
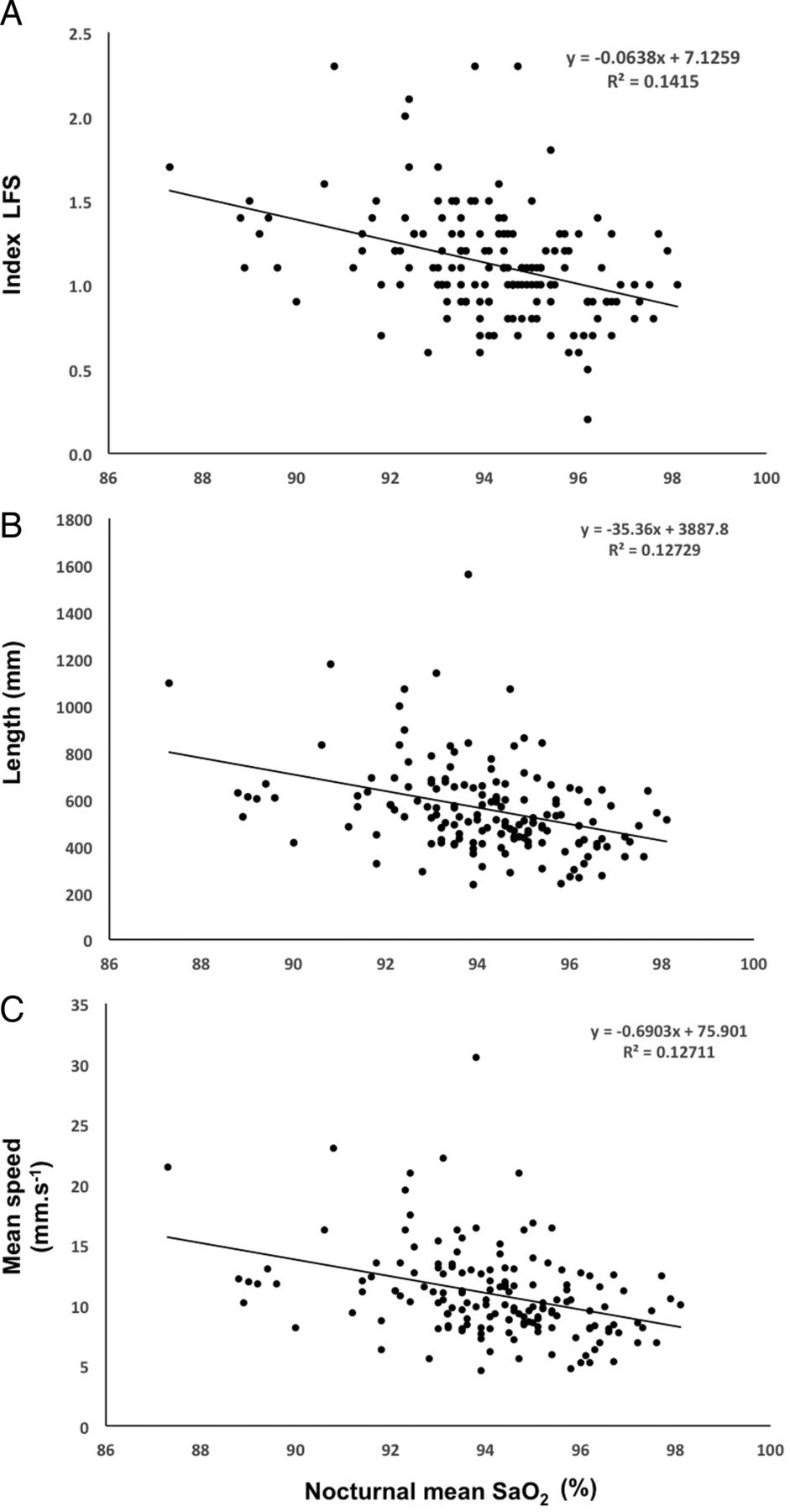
Correlations between nocturnal mean SpO2 and LFS (A) total length XY (B) and mean speed (C).
We also observed a significant and progressive increase in the main postural instability parameters with increasing SDB severity categories (no SDB=AHI <5/h, mild=AHI 5–15/h, moderate AHI 15–30/h and severe AHI >30/h). Post hoc analysis showed a significant difference in these parameters between no SDB (AHI <5/h) and moderate (>15/h) and severe (>30/h) categories (p<0.05 for all). After controlling for age and BMI, there was still a significant increase in LFS, XY length and mean speed with increasing SDB categories (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted means (for age, sleepiness and body mass index) of postural stability parameters according to sleep-disordered breathing (SDB) severity: no SDB apnoea–hypopnoea index <5/h, mild (5–15), moderate (15–30/h) and severe (>30/h).
Since diabetes could generate subclinical polyneuropathy influencing postural stability, we compared diabetic and non-diabetic subjects but no significant differences were found in the main stabilometric parameters (LFS: p=0.77, mean speed: p=0.14 and XY length: p=0.10).
Obesity is also known to affect postural stability. When a subgroup of non-obese subjects (BMI <30 kg/m2, n=87) was analysed using a multiple regression model, the same significant association between AHI and each of the three postural stability outcomes (LFS: p=0.031, mean speed: p=0.013 and mean XY length: p=0.013) were found, suggesting that this association was independent from obesity.
Discussion
The main finding of this study is that daytime postural stability seems to be influenced by nocturnal breathing disorders. To our knowledge this is the first study demonstrating an independent association between SDB severity and objectively measured postural impairment. The magnitude of the differences in stability parameters we observed between SDB and non-SDB participants (+22% increase in LFS, +25.0 increase in XY length and +22.9% increase in mean speed) is even larger than the differences found in Melzer et al28 between elderly fallers and elderly non-fallers: LFS (+11%), mean speed (+10%) and XY length (+5%). We thus believe that SDB-associated postural instability may have a significant clinical impact in the risk of accidental fall and injury. In line with our results, a recent study assessing spatiotemporal gait parameters after 8 weeks of CPAP treatment in patients with SDB found positive associations between SDB and gait quality.29 These results tend to confirm that gait control could be affected by SDB-related brain activity deficiencies as suggested by other studies.30 ,31
The factor showing the strongest independent association with the main postural stability parameters was mean nocturnal SpO2. This suggests that nocturnal hypoxaemia in patients with SDB could impair stability control during wakefulness. These results are in line with studies performed at high altitude showing that hypoxaemia could have an impact on postural stability. Wagner et al32 observed impaired standing balance at oxygen levels consistent with altitudes as low as 2438 m. Moreover, postural control is highly dependent on spindle mediated muscle stretch reflexes, which are considered to be crucial for maintaining the upright human stance.33 Hypoxia seems to directly alter muscle spindle reactivity, which may thus be one of the mechanism through which hypoxaemia may impair postural stability. This concept is supported by the observation of altered sensorimotor stability occurring in patients suffering from respiratory or circulatory insufficiency.34 Moreover, a reduced motor drive to contracting muscle was also noted in human beings during a simulated ascent of Mount Everest35 and in patients with hypoxaemia and chronic respiratory insufficiency.36 This tends to confirm that hypoxia can alter muscle control and thus postural stability, although the mean oxygen saturation level we observed in SDB is not quite as low as in high altitude or in respiratory insufficiency studies. Other mechanisms could thus be involved.
Considering that SDB disrupts sleep continuity, decreases slow wave sleep and total sleep time, we can also suspect that the effects we observed could be partially mediated by a decrease in sleep quality comparable to a sleep deprivation. A previous study by Fabbri et al37 showed an effect of sleep deprivation on LFS ratio and total length of CoP suggesting that sleep curtailment can induce a deactivation of brain areas mediating attention and also of the structures responsible for optimal postural stability. Attention has also been shown to be a key factor to maintain stability during daytime. Bougard et al38 previously showed that postural control fluctuates according to a circadian rhythm. The lack of association we found between the ESS score and the stability parameters does not confirm in our sample this association between postural stability and sleepiness. This may be explained by the subjective aspect of the ESS, which can be influenced by different factors such as depression, for example, and was shown to be poorly correlated with objectively measured sleepiness.39
These results should stimulate further research on stabilometry in patients with SDB in order to assess if SDB-associated postural instability is reversible after treatment. The exact mechanism of the association between SDB and postural instability should also be investigated through experimental studies assessing the effects of induced intermittent hypoxia, constant nocturnal hypoxia or induced sleep fragmentation (without hypoxia) on postural stability.
There are limitations in our study that need to be taken into account. First, this study was observational and these results should be confirmed by an interventional study assessing the effect of SDB treatment on postural stability or by a prospective study on a large cohort of subjects with and without SDB. Second, the absence of objective sleep evaluation in our subjects did not allow assessing the effect of sleep quality and duration on postural stability. Third, the relatively small sample did not allow stratification by gender, even if gender is not recognised as significant factor influencing stability40 and we did not find significant differences in the stability parameters between men and women in our study. Finally, daytime sleepiness was only assessed subjectively through the ESS. Further studies using objective sleepiness assessments and attention tests are needed to determine the effect of SDB-associated daytime sleepiness on postural stability.
Conclusion
Our results suggest the presence of an independent association between nocturnal breathing disturbances and daytime postural stability with a dose–response effect according to SDB severity. We believe that these results should raise awareness among clinicians evaluating patients with SDB that they might suffer from postural instability. Further prospective and interventional studies are needed to confirm this association and assess its reversibility with SDB treatment.
References
Footnotes
This study has been previously reported in abstract form at the the 22nd Congress of the European Sleep Research Society, 16–20 Sept 2014, Tallinn, Estonia.
Contributors The conception and design of the study, or acquisition of data or analysis and interpretation of data: FD, YG and SV. Drafting the article or revising it critically for important intellectual content: FD, JHR, OC and RH. Final approval of the version to be submitted: FD, YG, SV, JHR, OC and RH.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Cantonal Ethics Committee of Lausanne, Switzerland (# 474/12).
Provenance and peer review Not commissioned; externally peer reviewed.