Article Text

Statistics from Altmetric.com
A 39-year-old male non-smoking lumberyard worker from northern Mississippi was referred for evaluation of a left lower lobe mass. He had been treated 4 years earlier for papillary thyroid cancer with thyroidectomy and radioactive iodine ablation. Neck dissection after treatment showed 5/54 nodes with metastases and 3 nodes with granulomatous inflammation. He had been followed without evidence of recurrent malignancy until a CT obtained during a respiratory infection showed a left lower lobe mass extending to the hilum (figure 1A).

(A) Chest CT, axial view, at presentation showing a left lower lobe mass, see arrow; (B) 1 year later showing resolution of the left lower lobe mass after itraconazole treatment.
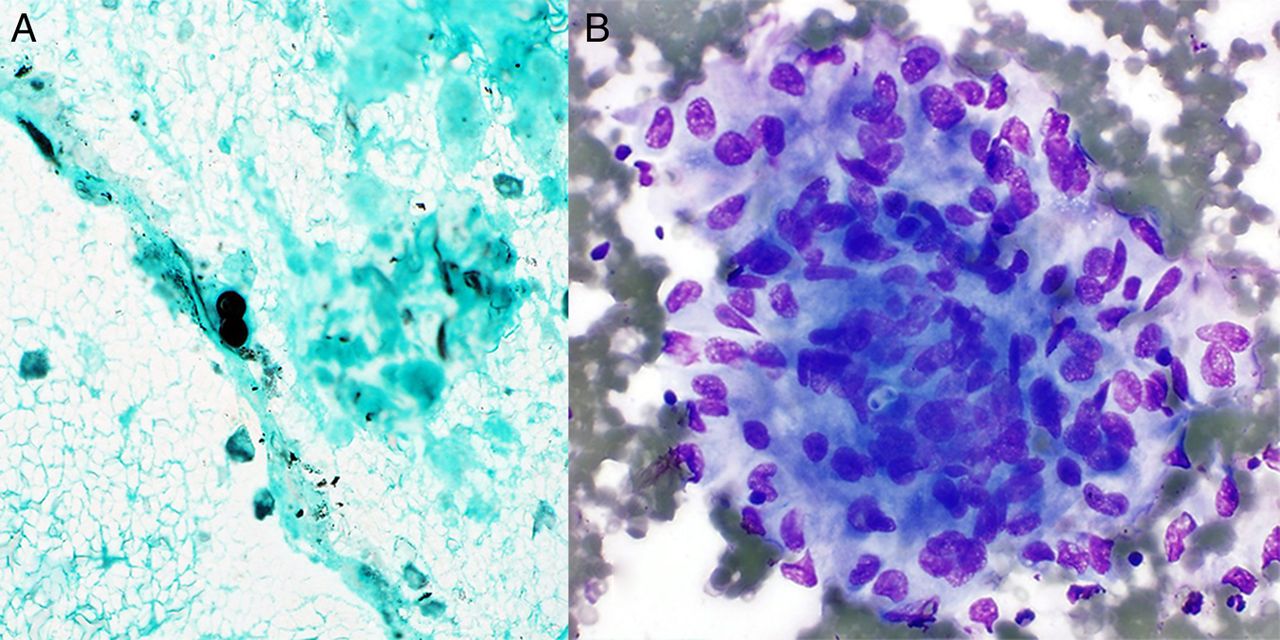
Bronchoscopy with endobronchial ultrasound and transbronchial needle aspiration was performed. Cytological examination revealed characteristic yeast forms with a single broad-based bud (figure 2A, B) consistent with blastomycoses. Blastomyces dermatitidis is a dimorphic fungus endemic to the upper Midwest USA, as well as the Ohio and Mississippi river valleys. Pulmonary blastomycosis may present as an asymptomatic lung mass, which cannot be distinguished from malignancy by radiographic features. Transmission is often associated with disruption of soil or organic matter, including wet or rotting wood.1 In a series of patients from Mississippi with blastomycosis, cytology was the first test to indicate the aetiological agent in 71.8% of those patients with pulmonary disease.2 Itraconazole is the treatment of choice for mild-to-moderate pulmonary blastomycosis.1 We believe our patient was likely infected at work. He was treated with itraconazole for 9 months, and follow-up CT revealed complete resolution of the mass (figure 1B).
{kind=link}
{kind=link}
(A) Gomori's methenamine silver stain), 600× magnification, cell block section, needle aspirate from the left lower lobe mass. Single broad-based budding yeast, 10–15 µm, characteristic of Blastomyces dermatitidis (B) Diff-Quik stain, 400× magnification, direct smear, needle aspirate from the left lower lobe mass. An aggregate of epithelioid histiocytes forming a granuloma contains a single broad-based budding yeast, 8–12 µm. The thick yeast wall is not stained, but the yeast protoplasm is. The morphology is characteristic of Blastomyces dermatitidis.
Footnotes
Contributors MRV and DRL drafted the article. JS contributed with cytology images and interpretation. HBG worked on image design. GAE, CJA and DO did a critical revision and editing of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.