Article Text

Statistics from Altmetric.com
A 14-year-old female patient affected by ataxia telangiectasia (AT) syndrome presented with mild dyspnoea and chest discomfort of a few days duration. After a short course of antibiotic therapy, which yielded no significant clinical improvement, a chest MRI was requested to evaluate possible acute or chronic pulmonary infections. The choice fell on MRI first because the patient’s conditions was not critical, and, second, to avoid further exposure to ionising radiations, as the patient had undergone a chest X-ray 2 weeks earlier for a similar episode.
The MRI study unexpectedly revealed a spontaneous right-sided pneumothorax of moderate size (figure 1). The pneumothorax was successfully treated with a chest tube and the patient recovered in 10 days.

{kind=link}
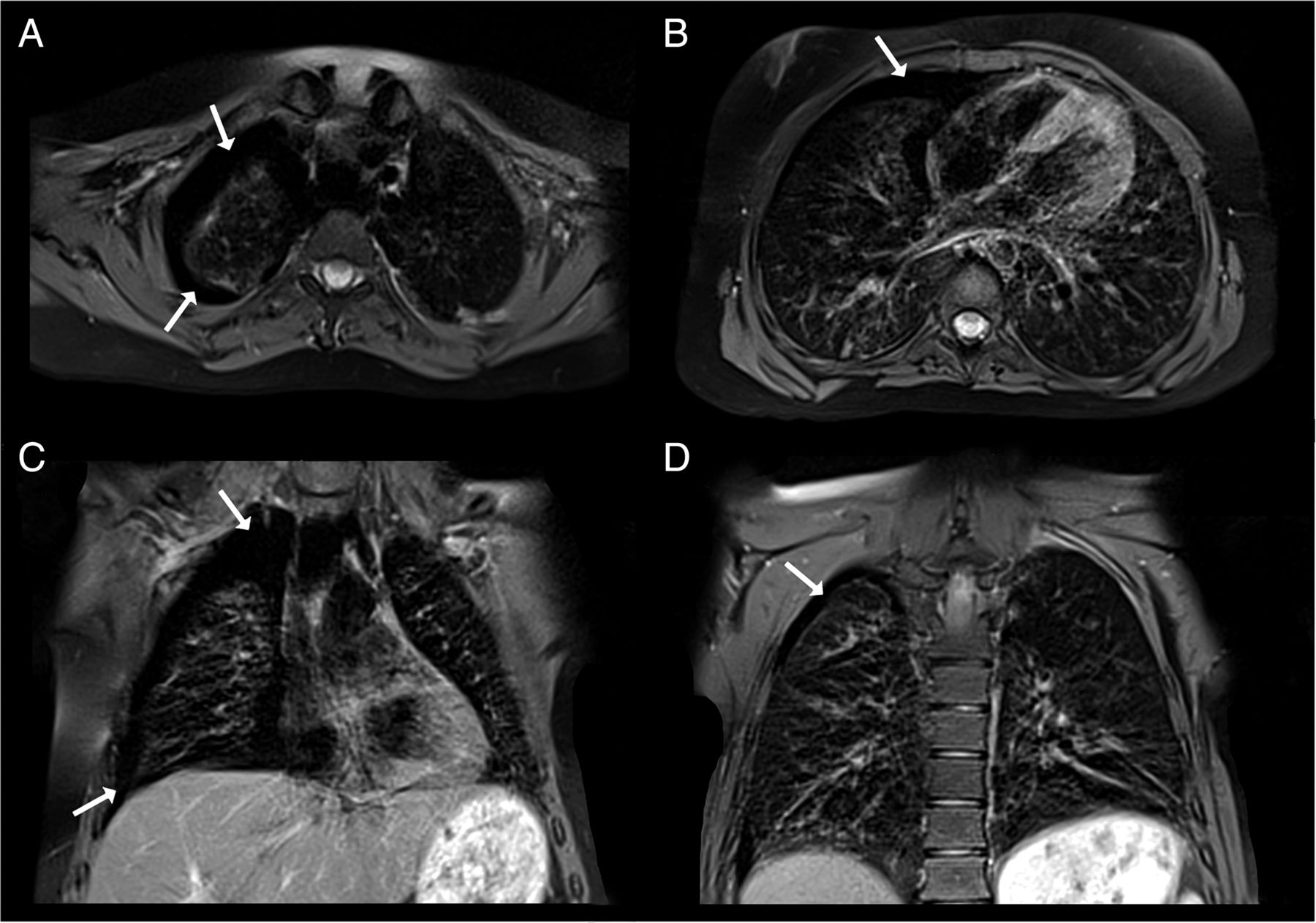
Free-breathing proton density BLADE sequences acquired on a 1.5 T unit (MAGNETOM Avanto, Siemens) on axial views (TR 3564 ms, TE 27 ms, slice thickness 5, 5 mm interslice gap, field of view 303×303 mm, matrix 256× 256; A and B) and on coronal views (TR 2466.5 ms, TE 27 ms, slice thickness 5, 6.5 mm interslice gap, field of view 310×310 mm, matrix 256×256; C and D) show a right-sided pneumothorax of moderate size (white arrows). The air rim between the pleura and the chest wall is mainly disposed along the ventral side. Mediastinum is not shifted to the opposite side. Free-breathing proton density BLADE sequences acquired on axial views (A and B) and coronal views (C and D) show a right-sided pneumothorax of moderate size (white arrows). The air rim between the pleura and the chest wall is mainly disposed along the ventral side. Mediastinum is not shifted to the opposite side. TR, repetition time; TE, echo time.
Lung involvement with progressive pulmonary disease is a major cause of morbidity and mortality in AT. Early pulmonary assessment is mandatory as 50% of patients with AT die in adolescence from overwhelming bronchopulmonary infections. Even in the absence of infections, these patients can develop pulmonary fibrosis. Schroeder et al1 reported that pneumothorax is not uncommon in patients with AT and pulmonary fibrosis and its early detection is crucial for both short-term and long-term survival.
AT is an autosomal recessive disease caused by mutations in the ATM gene, which induces abnormal DNA repair mechanisms and consequently genomic instability. AT cells have high sensitivity to ionising radiations and chemotherapeutic agents that cause double-stranded breaks in DNA, which leads to an increased risk of cancer. This is the reason why diagnostic tests involving X-rays should be avoided to minimise the risk of somatic mutations and consequent malignancy. Nevertheless, those studies are sometimes necessary to assess the extent and severity of lung structural damage and provide optimal patient management.
In this context, chest MRI has been recently demonstrated to be an alternative available tool to assess lung abnormalities and complications in patients with AT. Notably, MRI represents a useful diagnostic tool in supporting the decision to start a more aggressive airway therapy and in monitoring lung disease over time, particularly in patients with AT and airflow obstruction.2
MRI seems to be a promising tool in patients with AT who can benefit from its diagnostic accuracy in a continuously growing number of situations without the drawbacks of ionising radiation.3
Footnotes
Contributors All authors were involved in literature review, drafting of manuscript and critically reviewing it for intellectual content.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves