Article Text

Abstract
Prospective epidemiological studies, observational cross-sectional studies and some randomised prevention trials have demonstrated inconsistent findings of the impact of vitamin E on asthma risk. The goals of this study were to explore whether this differing association of vitamin E on asthma risk is due to an interaction of vitamin E isoforms. To address this question, in a population-based asthma incidence study we assessed the interaction between the plasma concentrations of vitamin E isoforms α-tocopherol and γ-tocopherol on asthma risk. Second, to understand the mechanisms of any interaction of these isoforms, we conducted experimental supplementation of α-tocopherol and γ-tocopherol isoforms in mice on the outcome of allergic airway inflammation. We found that in the highest γ-tocopherol tertile, low levels of α-tocopherol were associated with increased asthma risk, while highest tertile α-tocopherol levels trended to be protective. Similarly, in a mouse model of asthma, diet supplementation with α-tocopherol decreased lung inflammation in response to house dust mite (HDM) challenge. In contrast, diet supplementation with γ-tocopherol increased lung inflammation in response to HDM. These human and animal studies provide evidence for the competing effects of the vitamin E isoforms, in physiological concentrations, on asthma and allergic airway disease.
- Allergic lung disease
- Asthma
- Asthma Epidemiology
- Asthma Mechanisms
Statistics from Altmetric.com
Introduction
Prospective epidemiological studies, observational cross-sectional studies and some randomised prevention trials have demonstrated the impact of vitamin E on asthma risk. However, the directionality of the findings has not been consistent. Studies of vitamin E have sometimes included total vitamin E, without evaluating isoform concentrations, and have been conducted both over time and in different countries where the food isoform content of α-tocopherol and γ-tocopherol vary widely. In a recent prospective incidence study of the role of dietary antioxidants on asthma inception, we found a protective association for α-tocopherol, but not with γ-tocopherol. To address these divergent results and investigate the mechanisms through which vitamin E may promote or protect against asthma development, we report on the interaction of α-tocopherol and γ-tocopherol on asthma risk in a human cohort study, and the effect of experimental supplementation of individual isoforms on allergic airway inflammation in an animal model.
Methods
To explore whether this differing association of vitamin E isoforms on asthma risk is due to an interaction of these isoforms and to follow-up these findings to identify differential mechanisms and in vivo interaction, we conducted two studies. First, in the Shanghai Women's Asthma and Allergy Study, the only known study designed and powered to investigate the association of antioxidant defences on adult incident asthma, we assessed the interaction between α-tocopherol and γ-tocopherol in this population-based asthma incidence cohort on asthma risk.1 ,2 Second, to understand the mechanisms of any interaction of these isoforms, we conducted experimental supplementation of α-tocopherol and γ-tocopherol isoforms in mice on the outcome of allergic airway inflammation. The detailed methods of these studies are included in the online supplementary material.
Supplemental material
Results
The interaction of α-tocopherol and γ-tocopherol was assessed as continuous variables using multivariable conditional logistic regression analysis, while adjusting for smoking exposure, fat intake and exercise. α-Tocopherol levels were modelled with restricted cubic splines to assess for non-linear association with asthma risk. We observed a statistically significant interaction for the cross-product term (p-interaction=0.02).
To illustrate the effect modification, we also modelled the combined relationship of α-tocopherol and γ-tocopherol on asthma risk with γ-tocopherol levels grouped into tertiles. Within each γ-tertile, we fit a non-linear model of α-tocopherol levels on asthma risk. The results of these models are shown in figure 1. The relationship of α-tocopherol on asthma risk varied with γ-tocopherol tertile. In the highest γ-tocopherol tertile, low levels of α-tocopherol appear to be associated with a marked elevation in asthma risk, while highest tertile α-tocopherol levels trended to be protective. Across the γ-tocopherol tertiles, asthma risk varied with increasing α-tocopherol. In the medium and highest tertile γ-tocopherol, asthma risk fell steadily with increasing α-tocopherol; in the lowest γ-tocopherol tertile, there was little variation in asthma risk with increasing α-tocopherol levels.

Interaction of plasma levels of α-tocopherol and γ-tocopherol on asthma risk.
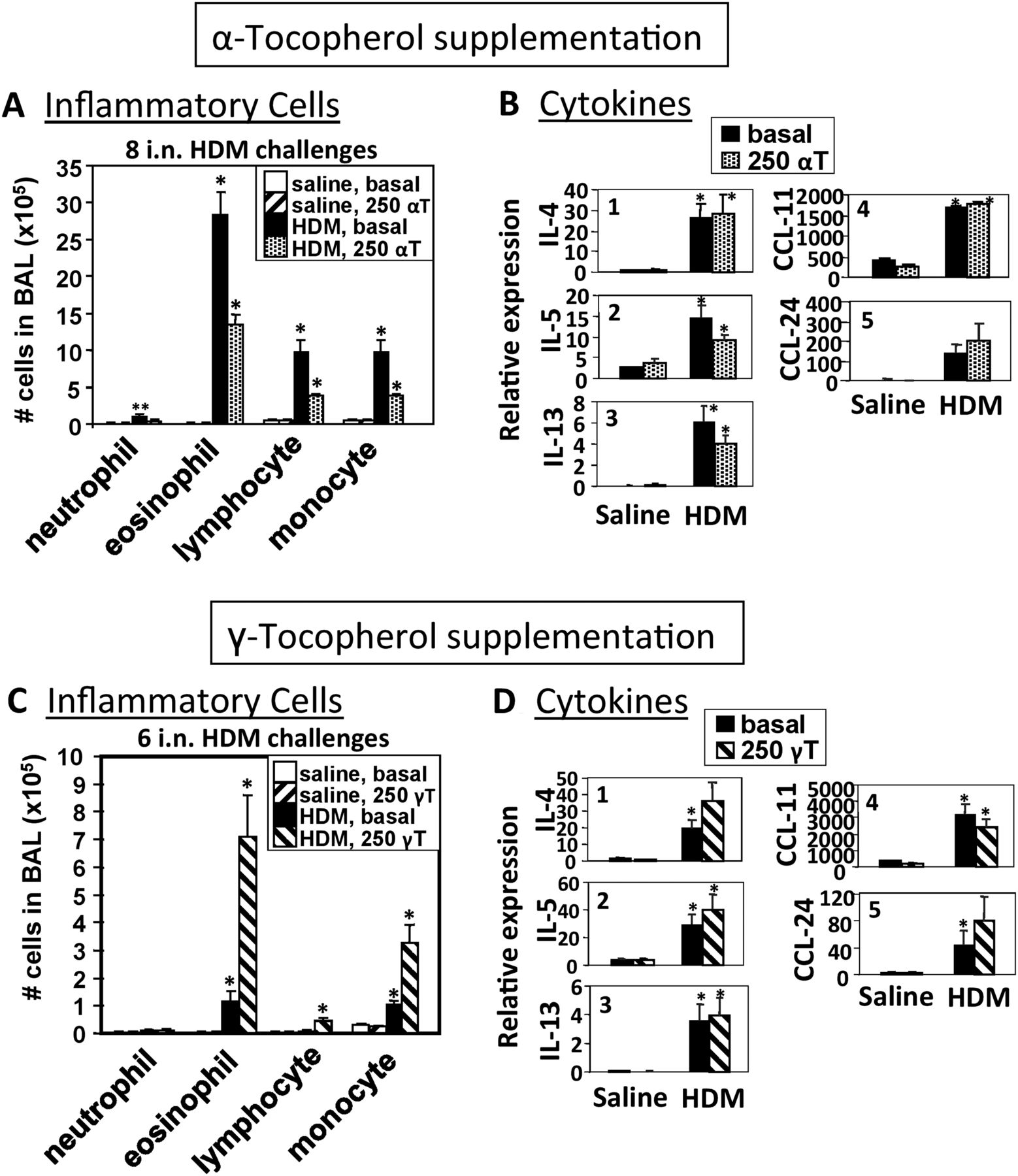
Similarly, in a mouse model of asthma, diet supplementation with α-tocopherol decreased lung inflammation in response to house dust mite (HDM) (figure 2A). In contrast, diet supplementation with γ-tocopherol increased lung inflammation in response to HDM (figure 2B). HDM challenge increased cytokines and chemokines in the lungs (figure 2C). However, supplementation with α-tocopherol and γ-tocopherol did not affect the HDM-induced cytokines and chemokines (figure 2C), which is consistent with our prior reports that tocopherols regulate intracellular signals for leucocyte transendothelial migration without regulation of cytokines.3–6

{kind=link}
{kind=link}
Opposing effects of diet supplementation with d-α-tocopherol (αT) and d-γ-tocopherol (γT) on leucocyte infiltration into the mouse lung, and impact on bronchoalveolar lavage (BAL) cytokines. HDM, house dust mite; IL, interleukin.
Discussion
This set of human and animal studies helps elucidate the opposing roles of vitamin E isoforms on asthma and allergic airway inflammation. In the human cohort study, we observed effect modification of the protective relationship of α-tocopherol on asthma risk at varying levels of γ-tocopherol. In the animal model, we demonstrated a differential response of supplementation of α-tocopherol and γ-tocopherol on lung inflammation in response to HDM challenge, suggesting that these isoforms act in opposing directions on allergic airway responses.
Previous studies of vitamin E on asthma risk have been limited by assessing aggregate levels of isoforms or merely dietary intake across different areas of the world where the α-tocopherol and γ-tocopherol content of diets is dramatically different.7 In addition, in supplementation trials, supraphysiological supplementation has been used, and in α-tocopherol supplementation trials, the carrier is often high in γ-tocopherol, making it difficult to assess the independent effect of the isoforms. Clinically, α-tocopherol has also been associated with higher lung function and γ-tocopherol associated with lower lung function.8
This report is the first rodent study demonstrating that diet supplementation with α-tocopherol inhibits and γ-tocopherol increases eosinophilic allergic inflammation to the clinically relevant antigen HDM. In previous studies with chicken egg ovalbumin (OVA)4 ,5 and the current study with responses to HDM, daily administration of tocopherols did not significantly regulate cytokines and chemokines in the lung tissue. However, α-tocopherol has been reported to inhibit, and γ-tocopherol increase, eosinophil migration across endothelium and into tissues during allergic responses.4 ,6 ,8 In mechanistic studies, we have demonstrated that α-tocopherol is an antagonist of protein kinase C alpha (PKCα) and that γ-tocopherol is an agonist of PKCα.6 PKCα is activated by vascular cell adhesion molecule-1 (VCAM-1) on endothelial cells during VCAM-1-dependent recruitment of eosinophils.9 ,10 Taken together, this suggests that tocopherol isoforms have opposing functions on the signals for eosinophil recruitment. However, there is no perfect clarity on the impact of these isoforms on lung inflammation in animal studies. In a study with intermittent oral gavage α-tocopherol on HDM challenge, α-tocopherol did not alter HDM-induced inflammation; importantly, however, the α-tocopherol was administered after the HDM challenge.11 In other studies with daily subcutaneous tocopherol administration, which raises tissue tocopherols 2–3-fold, α-tocopherol reduced eosinophilic inflammation while γ-tocopherol increased eosinophils in OVA-induced responses that were primarily eosinophilic.4 ,5 In contrast in another study, γ-tocopherol supplementation reduced antigen induction of rat lung inflammation in which there was 2.5-fold more neutrophils than eosinophils.12 It is known that in the presence of lipopolysaccharide (LPS) in OVA inhalations, the lung lavage becomes predominantly neutrophilic (2–3 times more neutrophils than eosinophils), while13 it is also reported that nebulised γ-tocopherol reduces neutrophilia in burn and smoke inhalation injury in sheep.14 In acute models of inflammation with large numbers of neutrophils, such as with LPS or ozone, there is generation of reactive nitric oxide species, known to be15 ,16 scavenged by γ-tocopherol but not α-tocopherol.17–19 Therefore, γ-tocopherol, which scavenges nitric oxide, may be of benefit for acute neutrophilic inflammation, whereas it may increase eosinophilia during allergic responses to OVA and HDM.
There are limitations of these studies that should be considered. The human study was not designed specifically to assess the interaction between the vitamin E isoforms. The animal studies may not simulate what occurs in humans nor account for the human host differences in vitamin E metabolism, and the animal studies were done with either one of the two isoforms to determine their independent effects as a follow-up to the interaction noted in the human study. Lastly, while animal models allow for testing in controlled settings where everything else can be held constant, it is well recognised that murine allergen challenge models do not replicate what occurs in humans. However, despite these limitations, the combination of a human asthma incidence study and a suggested mechanism in an animal model supports the idea of opposing effects of these vitamin E isoforms, which may also help to explain the discrepant findings among studies.
These human and animal studies provide evidence for potential competition of the vitamin E isoforms, in physiological concentrations, on asthma and allergic airway disease. Controlled clinical studies are needed to further elucidate the effects of modifying diet to decrease γ-tocopherol intake, enhance α-tocopherol intake or supplementation of α-tocopherol at physiological concentrations on the prevention of asthma and allergic airway disease.
References
Footnotes
Contributors JC-M was involved in study design, animal experiments, data analysis and writing the manuscript. TG and WDD were involved in study design, data analysis and editing the manuscript. HA-V and JG were involved in the animal experiments and data analysis. EKL, CR-S and TJH were involved in the human study, data analysis and editing the manuscript. XOS was involved in study design and study funding. TH was involved in study design, human study data acquisition, data analysis, writing the manuscript and study funding.
Funding This study was funded by National Institute of Allergy and Infectious Diseases RO1 AI 50884 (TH), K24 AI 77930 (TH), National Institute of Complementary and Alternative Medicine R01 AT004837 (JC-M) and National Institute of Heart, Lung, and Blood R01HL111624 (JC-M). The project described was also supported by the U.S. National Cancer Institute R37 (Dr Wei Zheng) and NO2-CP11010-66 (XOS).
Competing interests None declared.
Ethics approval Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.