Article Text

Statistics from Altmetric.com
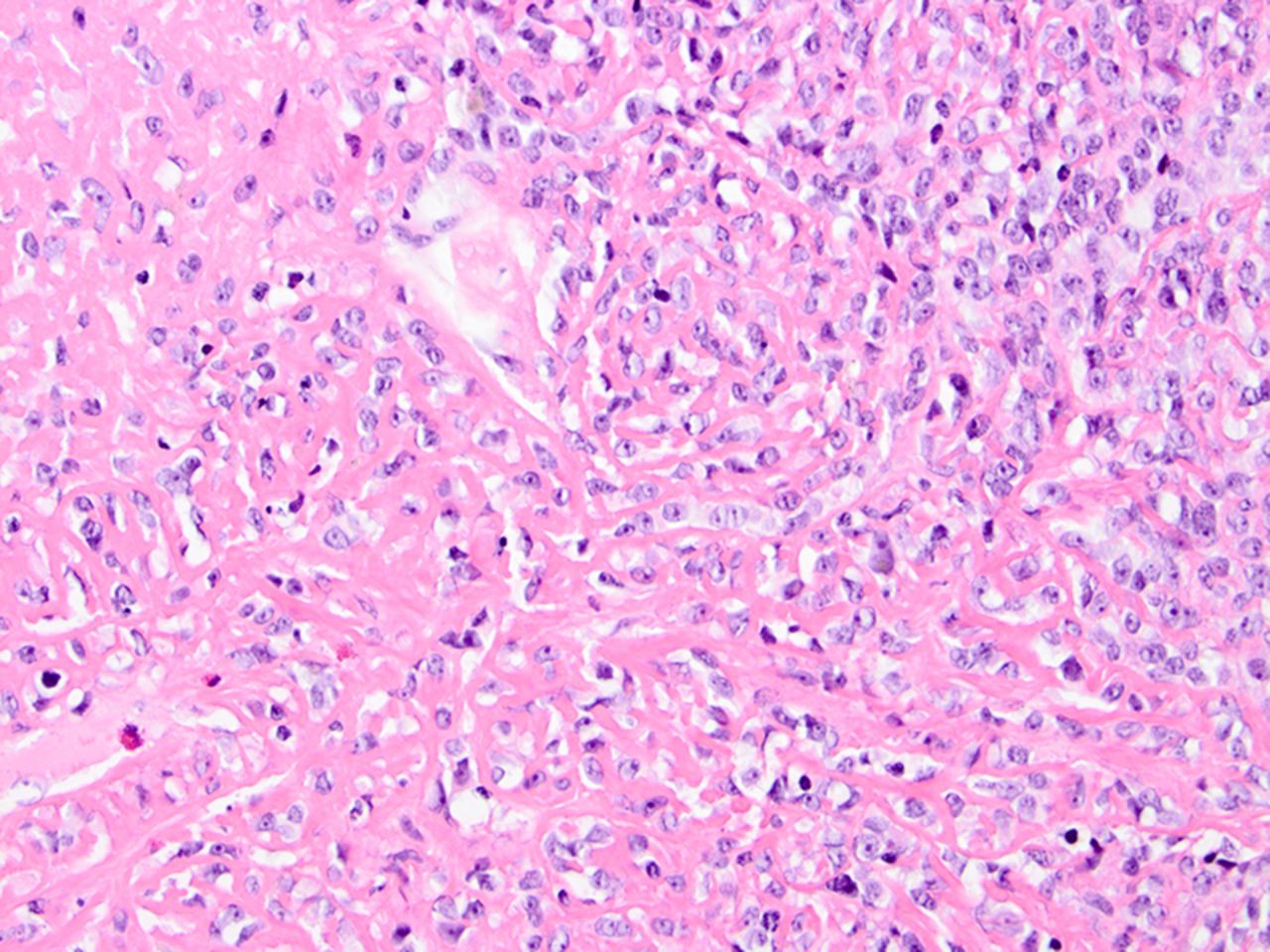
A 63- year-old Caucasian man who smoked presented with lower back pain, dyspnoea and weight loss. A chest CT showed multiple bilateral cavitating lesions, consolidations and ground glass lesions (figure 1). Because a CT-guided pulmonary biopsy elsewhere revealed chronic inflammation with caseating granulomas, he had initially been treated with tuberculostatics and subsequently antifungal medication without clinical improvement. Since the patient had also developed a lesion in the neck, this was biopsied and revealed an undifferentiated round cell tumour. Subsequently, a video-assisted thoracoscopy was performed. Pathological analysis demonstrated metastasis of an osteosarcoma; therefore, the final diagnosis was metastasised extraskeletal small cell osteosarcoma (figure 2).

Cavitating lesions (1), ground glass lesions (2) and consolidations (3).
{kind=link}
{kind=link}
Round cell tumour and osteoid matrix.
Despite treatment with radiotherapy for bone metastasis and doxorubicin-based chemotherapy, he died a few months later.
Extraskeletal osteosarcomas are high-grade mesenchymal soft tissue malignancies accounting for 1% of all soft tissue sarcomas and approximately 2–4% of all osteosarcomas. By definition, they produce osteoid or cartilage matrix in a sarcomatous pattern and originate in soft tissue without attachment to adjacent osseous structures. They typically affect patients in the sixth decade of life with a slight male predominance.1 The lower and upper extremities are most commonly affected, followed by the retroperitoneum and other body sites. Although prior radiation therapy is a known risk factor, 90% of cases are idiopathic. Radiological features include soft-tissue opacities, while calcifications or osteoid matrix. Depending on the degree of necrosis, tumour enhancement is seen on CT or MRI after intravenous contrast.2 Metastases commonly comprise the lungs, bones, lymph nodes, brain, liver and skin. Preferential treatment is surgical resection of the primary tumour. For metastasised disease doxorubicin-based chemotherapy and radiotherapy are commonly used although overall prognosis is poor, with a 5-year survival rate approximately 10%.1
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves