Article Text

Abstract
Introduction and objectives Radiological detection of pleural malignancy (PM) remains challenging. In early-stage Malignant Pleural Mesothelioma (MPM) a pleural effusion may be the only significant abnormality, indistinguishable from benign asbestos-related pleural effusion (BAPE). PM is associated with neovascularisation. We report the diagnostic performance of a novel perfusion-based Magnetic Resonance Imaging (MRI) biomarker of PM – Early Contrast Enhancement (ECE).
Methods 24 patients with suspected PM were recruited prospectively. All underwent contrast-enhanced Computed Tomography (CT) scanning, 3T Pleural MRI and Thoracoscopy.
18/24 had complete MRI examinations: T1-weighted 3D-spoiled-gradient-echo sequences acquired at baseline, 40 s, 80 s and 4.5, 9 and 13.5 min after intravenous Gadobutrol contrast. Mean signal intensity (SI) of representative parietal pleura was derived from 15 regions of interest placed by two respiratory physicians. ECE was defined objectively by an early peak in mean SI (≤4.5 min) on the resulting SI/time curve (Figure 1). Morphology suggestive of PM on CT and MRI was recorded by two thoracic radiologists. Diagnostic performance and inter-observer agreement for ECE, MRI and CT morphology were compared. All analyses were blinded.
Pleural SI data were correlated against Microvessel Density (MVD) measured in paraffin-embedded pleural biopsies stained with CD34 and Factor VIII immunostains.
Results Mean patient age was 73 (SD 8) years. 18/24 were asbestos-exposed and 12/18 had pleural thickening ≤5 mm. ECE was present in 10/11 patients with PM (MPM (n = 10); lung cancer (n = 1)). The false negative case had MPM. ECE was absent in 6/7 patients with benign pleural disease (BAPE (n = 4), fibrothorax (n = 2), TB (n = 1)). The false positive case had TB.
Overall diagnostic accuracy of ECE, MRI and CT morphology: sensitivity 91%, 91%, 90%; specificity 86%, 71%, 50%; negative predictive value 86%, 83%, 80%; positive predictive value 91%, 83%, 69% respectively. Inter-observer agreement was 0.766 for ECE, 0.727 for MRI and 0.753 for CT.
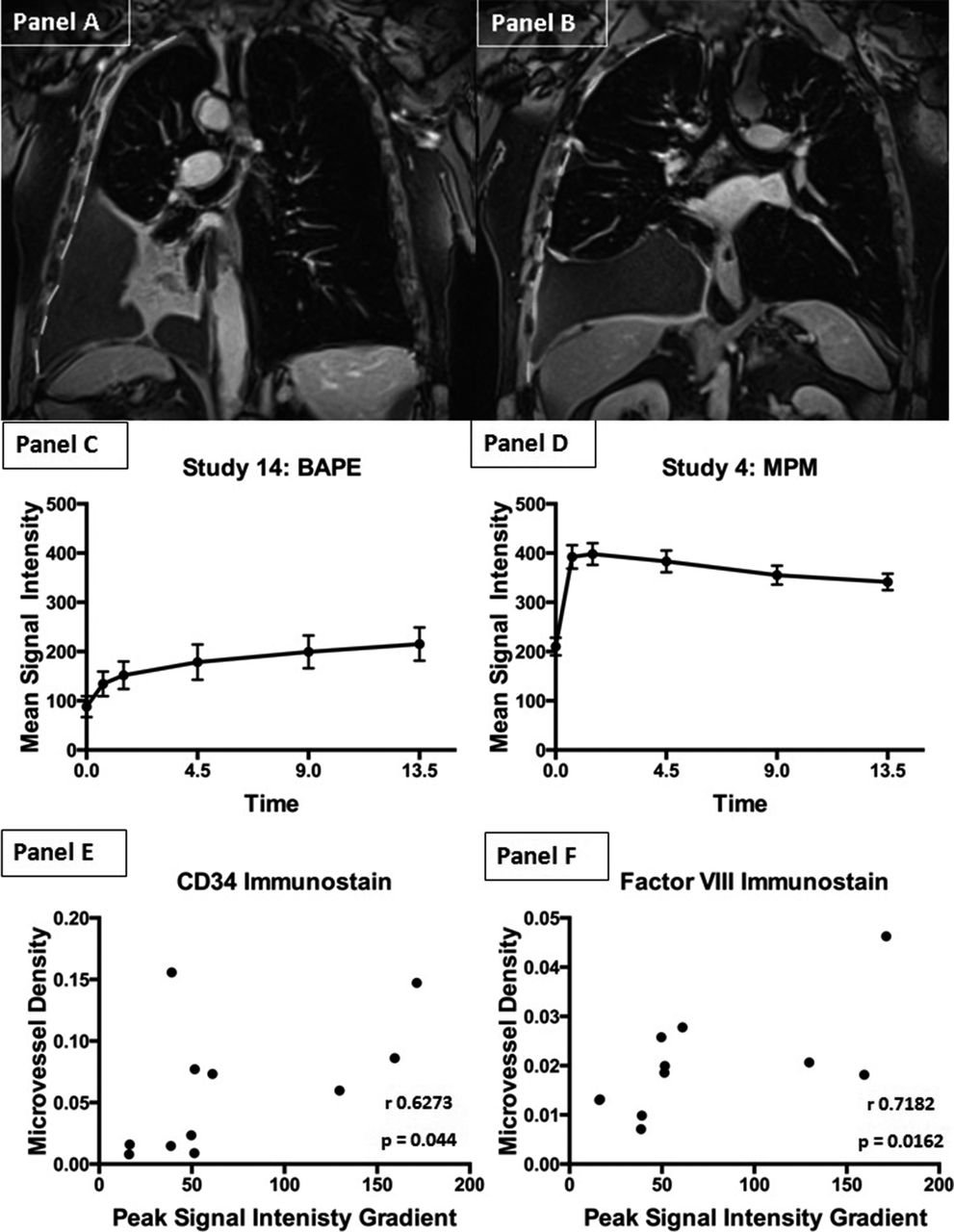
Figure 1 shows the relationship between MVD and Pleural SI.

{kind=link}
Example of 3D T1-weighted Pleural MR images acquired 4.5 minutes post-Gadobutrol in 2 different patients – one with BAPE (Panel A) and one with early-satge MPM (Panel B). Panels C and D show the accompanying partietal pleura SI/time curves for each patient (Panel C: patient with BAPE – ECE absent, panel D: patient with MPM – ECE present). Panels E and F demonstrate the relationship between peak signal intensity gradient in patients with pleural malignancy and Microvessel Density measured in diseased tissue with CD34 immunostain (Panel E) and Factor VIII immunostain (Panel F)
Conclusions ECE appears an accurate and reproducible, perfusion-based, objective biomarker of PM, out-performing subjectively-defined CT and MR morphology. ECE assessment can be performed in patients with minimal pleural thickening, suggesting potential utility as a biomarker of early-stage MPM or low-volume metastatic PM.