Article Text

Statistics from Altmetric.com
A 28-year-old woman was incidentally found to have a large right apical mass (figure 1) on a chest radiograph. She denied having any respiratory symptoms but had noted asymmetric flushing of her face following strenuous exercise (figure 2). On closer questioning she also described hypohydrosis affecting the right side of her face.

Chest radiograph showing a large right apical opacity and evidence of thinning of the right second rib posteriorly.

Well-demarcated unilateral flushing following exercise.
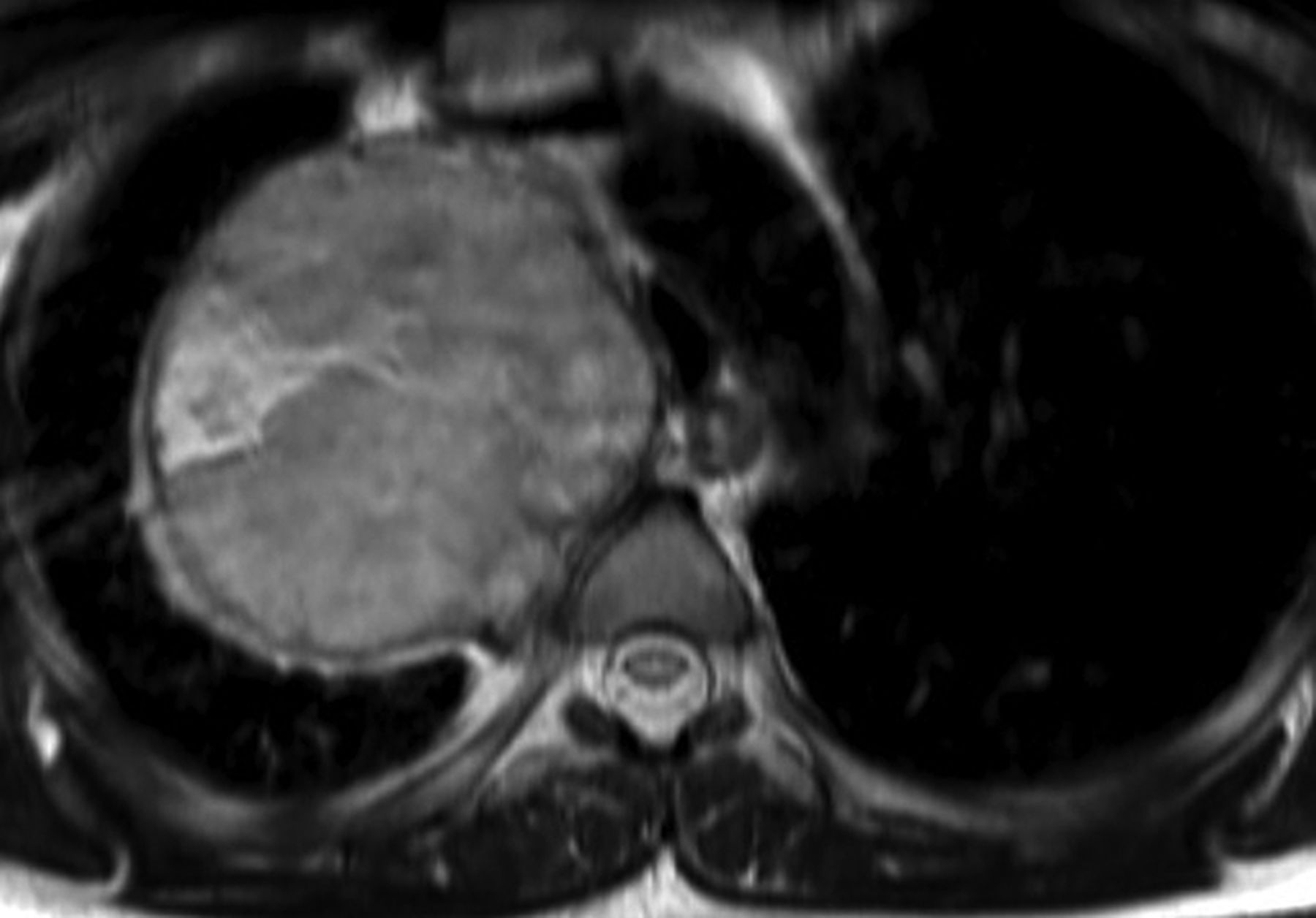
She had further imaging with an MRI scan that was suggestive of a nerve sheath tumour (figures 3 and 4), which was subsequently resected by thoracic surgery. The histology confirmed a schwannoma.

Axial T2-weighted total spin echo MRI image showing a high signal heterogeneous tumour in right apex.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Post-gadolinium T1-weighted MRI sagittal image demonstrating marked tumoural enhancement.
The ‘Harlequin sign’ is characterised by asymmetric flushing and sweating of the face, representing localised ipsilateral autonomic dysfunction, due to a cervical sympathetic deficit located at the preganglionic or postganglionic level on the non-flushing side.1 In our case, unilateral facial flushing was caused by tumour compression of the cervical sympathetic chain. Since resection of the tumour, her symptoms have improved significantly.
Harlequin syndrome is a rare syndrome secondary to autonomic dysfunction resulting in anhydrosis and absent or reduced facial flushing on the affected side. Oculosympathetic paresis maybe present in some cases. Causes of Harlequin syndrome include carotid artery dissection, local trauma and neurotropic viral infections but rarely is idiopathic.2 Traditionally, the side with excessive flushing and sweating was perceived to be pathological, but it is now believed that the excessive flushing and sweating is due to a compensatory over-reaction to regulate heat of the face by the unaffected side of the face.3
Footnotes
-
Collaborator Dr Hilary Archer, Clinical Lecturer in Neurology, University of Bristol.
-
Contributors DDF, AL-L, TB and NAM cared for the patient and wrote the paper. AE reviewed the radiology and critically appraised the paper.
-
Competing interests None declared.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves