Article Text

Abstract
Background Strategies for identifying normotensive patients with acute symptomatic PE at high risk of PE-related complications remain to be defined.
Methods This prospective cohort study aimed to determine the role of plasma lactate levels in the risk assessment of normotensive patients with acute PE. Outcomes assessed over the 7 days after the diagnosis of PE included PE-related mortality and haemodynamic collapse, defined as need for cardiopulmonary resuscitation, systolic blood pressure <90 mm Hg for at least 15 min, need for catecholamine administration, or need for mechanical ventilation.
Results Between December 2012 and January 2014, the study enrolled 496 normotensive outpatients with acute symptomatic PE. PE-related complications occurred in 20 (4.0%; 95% CI 2.5% to 6.2%) of the 496 patients. These patients had higher baseline lactate levels (median 2.66 mmol/L; IQR 1.56–5.96 mmol/L) than patients without complications (1.20 mmol/L; IQR 1.20–2.00 mmol/L) (p<0.001). Overall, 135 patients (27.2%) had plasma lactate ≥2 mmol/L. Fourteen (10.4%) of them had PE-related complications versus 6 of 361 patients with low lactate (negative predictive value 98.3%; p<0.001). Patients with elevated plasma lactate had an increased rate of PE-related complications (adjusted OR 5.3; 95% CI 1.9 to 14.4; p=0.001) compared with those with low lactate. The combination of elevated plasma lactate with markers of right ventricular dysfunction (by echocardiogram) and myocardial injury (by cardiac troponin) was a particularly useful prognostic indicator (positive predictive value 17.9%; 95% CI 6.1% to 36.9%).
Conclusions Plasma lactate represents a powerful predictor of short-term PE-related complications and may provide guidance for decision-making in PE care.
- Pulmonary Embolism
Statistics from Altmetric.com
Key messages
What is the key question?
-
What is the role of plasma lactate levels in the risk assessment of normotensive patients with acute PE?
What is the bottom line?
-
Plasma lactate measurement represents a powerful method of predicting short-term PE-related complications.
Why read on?
-
The combination of high troponin, echocardiographic right ventricular dysfunction and high lactate may provide guidance for decision-making in PE care.
Introduction
Haemodynamic status has significant prognostic implications for patients diagnosed with acute PE. Patients with acute symptomatic PE presenting with shock or refractory arterial hypotension (systolic blood pressure <90 mm Hg or a pressure drop of ≥40 mm Hg for ≥15 min), indicating overt right ventricular (RV) failure, are particularly at high risk of early death and should therefore undergo prompt recanalisation treatment.1–3 For haemodynamically stable patients with PE, the categorisation of risk for subgroups may assist with decision-making regarding PE therapy.4
In the subgroup of normotensive patients with PE, rapid and accurate prognostication and risk stratification have focused mainly on RV dysfunction or injury to the myocardium as a result of acute pressure overload.4–7 However, although some evidence suggests that a subset of normotensive patients with acute symptomatic PE may have a reasonable risk-to-benefit ratio for thrombolytic therapy, single markers of RV dysfunction and myocardial injury have an insufficient positive predictive value for PE-specific mortality to drive decision-making toward such therapy.8 ,9
Plasma lactate concentration is a marker of the severity of the tissue oxygen supply-to-demand imbalance. Similar to other scenarios, such as sepsis or trauma, lactate concentration might increase in patients with acute PE before overt haemodynamic impairment.10–13 One small single-centre study found an association between high plasma lactate levels and short-term all-cause mortality in patients with acute PE, independent of the presence of haemodynamic instability or markers of RV dysfunction or injury.14 ,15 Thus, lactate may be potentially useful for identifying normotensive PE patients at high-risk of PE-related adverse clinical events.
This study was designed to prospectively assess the prognostic significance of elevated lactate in a cohort of haemodynamically stable patients with acute symptomatic PE. Furthermore, we aimed to determine the optimal combination of prognostic tools for detecting patients with preserved systemic arterial pressure deemed to be at higher risk of PE-related complications.
Methods
Study design
This was a prospective, multicentre, observational cohort study (NCT01908231) designed by the authors. The institutional review board of each centre approved the protocol and consent forms.
Setting
Patients were recruited from the emergency department of seven academic and two general urban hospitals in Italy and Spain between 1 December 2012 and 31 January 2014.
Study eligibility and patients
The study required confirmation of the PE diagnosis with a positive contrast-enhanced, PE-protocol, multidetector CT pulmonary angiography.16 Patients with any of the following conditions were excluded: haemodynamic instability at presentation (defined as systolic blood pressure <90 mm Hg); treatment with thrombolytic agents at the time of PE diagnosis; life expectancy <3 months (ie, terminally ill patients); pregnancy; geographic inaccessibility that precluded follow-up; age younger than 18 years.
Plasma lactate determination
The plasma lactate concentration was determined on arterial blood samples (the type of test used was determined by the department of clinical chemistry at each participating site). Based on previous data, we considered plasma lactate levels ≥2 mmol/L to be abnormal.14 ,15
Transthoracic echocardiography
The study required that patients undergo transthoracic echocardiography within 24 h after diagnosis of PE. Trained and certified local physicians, blinded to the patient's clinical data and laboratory test results, interpreted each echocardiogram. RV dysfunction was assessed by echocardiography.2 ,4 ,7 The study defined RV dysfunction as presence of at least one of the following: (1) RV dilatation (end-diastolic diameter >30 mm or right/left ventricular end-diastolic diameter ratio ≥1 in apical four-chamber view); (2) pulmonary hypertension (estimated RV–right atrial transtricuspidal gradient over 30 mm Hg); (3) hypokinesis of the RV free wall (any view).
Cardiac troponin testing
Participant sites used different biomarkers for myocardial injury (troponin I and T) and different cut-off points for abnormal levels. Four of the participating centres used the same assay (cardiac troponin I (cTnI); Abbot, USA) with a cut-off point of 0.05 ng/mL, while three centres used the same assay with a cut-off point of 0.10 ng/mL. The remaining centres used a highly sensitive troponin T immunoassay (Roche, Germany) with a cut-off point of 14 pg/mL. In most of the sites, the cut-off points for troponin assays were defined according to standard criteria, which were values exceeding the 99% centile of healthy subjects with a coefficient of variation of 10%.
Treatment and follow-up
Clinicians at enrolling sites managed patients according to their local practice (ie, no standardisation of treatment). Most patients received initial anticoagulation with intravenous unfractionated heparin (UFH), subcutaneous low-molecular-weight heparin (LMWH) or fondaparinux, and overlap and long-term therapy with an oral vitamin K antagonist. In patients whose clinical status deteriorated after enrolment, the clinicians administered thrombolytic treatment and/or inotropic support as deemed appropriate. This study analysed outcomes over the 30 days after diagnosis of PE.
Study outcomes
This study used a clinical composite (ie, PE-related complications) of PE-related death or non-fatal haemodynamic collapse within 7 days of diagnosis as the primary outcome. PE was considered the cause of death if there was objective documentation or if the cause was unexplained and PE could not be confidently ruled out. Haemodynamic collapse was defined as at least one of the following: (i) need for cardiopulmonary resuscitation; (ii) systolic blood pressure <90 mm Hg for at least 15 min, with signs of end-organ hypoperfusion (cold extremities, or urinary output <30 mL/h, or mental confusion) or need for catecholamines (except for dopamine at a rate of <5 µg/kg/min) to maintain adequate organ perfusion and a systolic blood pressure of >90 mm Hg; (iii) need for invasive or non-invasive mechanical ventilation. Secondary outcomes included 30-day all-cause and PE-related death. An adjudication committee, composed of three independent experts who were blinded to patients’ clinical characteristics and the results of prognostic testing, adjudicated on all adverse events.
Statistical analysis
The study reported categorical data as proportions, and continuous data as mean+SD or median (first–third IQR). We used unpaired two-tailed t tests or the Mann–Whitney U test (for those variables found not to follow a normal distribution) for comparisons of the distributions of continuous variables between patients with or without elevated plasma lactate, and χ2 or Fisher's exact tests for comparisons of categorical data between the two groups. Sample size was calculated for the primary end point. We calculated a priori a power of 80% (two-sided type 1 error, 5%) to reject the null hypothesis that the presence of elevated plasma lactate will not predict the primary end point in the available sample of 494 patients, using the following assumptions: presence of elevated plasma lactate in 30% of the sample; a difference in mortality rate of 10% between patients with and without elevated plasma lactate; a drop out of 10%.14
We used logistic regression to assess independent associations between potential baseline predictors and the outcome in the cohort.7 For the manual backward stepwise multivariable logistic regression model, we assessed variables that had a significance level of p<0.20 in univariable analyses. The model primarily assessed the prognostic information of lactate and cardiac predictors (ie, echocardiography and troponin testing) and adjusted for clinical confounders deemed statistically significant on univariable analysis. The final model retained variables associated with the outcome at a significance level of p<0.05.
In addition, to evaluate the role of a strategy combining lactate with cardiac biomarkers and echocardiography for identifying normotensive patients with acute symptomatic PE at high risk of PE-related complications, we used multiple logistic regression analysis to compare the complication rate of three patient groups: (1) troponin elevation and RV dysfunction; (2) troponin elevation, RV dysfunction and no lactate elevation; (3) troponin elevation, RV dysfunction and lactate elevation. No adjustments for other baseline variables were made in the latter model.
To assess the test and performance characteristics of combinations of the simplified PE Severity Index (sPESI),17 lactate, cardiac troponin and echocardiogram variables, we estimated the positive predictive value and the positive likelihood ratio, as well as the sensitivity, specificity, negative predictive values and negative likelihood ratio for predicting the primary outcome.
Statistical significance was defined as a two-tailed p value of <0.05 for all analyses. We performed our calculations using the SPSS statistical package (V.19.0).
Results
Study sample
Study staff screened 539 consecutive outpatients with acute PE for eligibility. Haemodynamic instability ruled out 29 (5.4%) patients from participation. Of the remaining 510 haemodynamically stable patients, the study excluded 14 (2.7%) because they had received initial recanalisation procedures. The remaining eligible 496 patients (242 men and 254 women) were enrolled in the study (figure 1). Of these 496 patients, 319 (64.3%) received initial therapy with LMWH, 156 (31.5%) received UFH, and 21 (4.2%) received an inferior vena cava filter.

Patient flow diagram.
Table 1 shows the patients’ clinical symptoms, predisposing conditions, and relevant findings at presentation. On admission, lactate levels ranged from 0 to 18.2 mmol/L and had a median value of 1.3 mmol/L (IQR 0.93–2 mmol/L). Of the 496 enrolled patients, 135 (27%) had elevated serum lactate levels (lactate-positive group) and the remaining 361 patients had normal serum lactate levels (lactate-negative group). Patients in the lactate-negative group were younger and had fewer signs of clinical severity (eg, tachycardia, RV dysfunction, myocardial injury) than those in the lactate-positive group (table 1).
Clinical symptoms and relevant findings at presentation in 496 consecutive normotensive patients diagnosed with acute symptomatic PE in the emergency department
Outcome
The study had complete outcome information for all patients at the end of follow-up. The primary outcome occurred in 20 of the 496 (4.0%; 95% CI 2.5% to 6.2%) normotensive patients with acute symptomatic PE who entered the study (table 2). PE-related death occurred in 7 (1.4%) patients, while haemodynamic collapse occurred in 13 (2.6%) patients. These patients had higher baseline lactate levels (median 2.66 mmol/L; IQR 1.56–5.96 mmol/L) than patients with an uncomplicated course (1.20 mmol/L; IQR 1.20–2.00 mmol/L) (p<0.001). Fourteen events (10.4%; 95% CI 5.8%−16.8%) occurred in the group of patients entering the study with acute PE and elevated serum lactate levels, whereas six events (1.7%; 95% CI 0.3% to 3.0%) occurred in the group with normal serum lactate levels (absolute difference 8.7%; 95% CI 3.9% to 12.2%; p<0.001).
Clinical events after diagnosis and treatment of 496 normotensive patients with acute symptomatic PE
Based on univariable logistic regression analyses, significant baseline (at the time of acute PE diagnosis) predictors of the primary outcome during follow-up included plasma lactate levels ≥2 mmol/L (OR 6.9; 95% CI 2.6 to 18.2; p<0.001), RV dysfunction (OR 3.6; 95% CI 1.4 to 9.6), tachycardia (OR 3.6; 95% CI 1.4 to 9.0; p=0.010), and systolic blood pressure 90–100 mm Hg (OR 3.4) (table 3). Increasing lactate concentrations were associated with an increased risk of the primary outcome (OR 1.48; 95% CI 1.25 to 1.75, p=0.017) (figure 2). When RV dilatation was considered as the only criterion for RV dysfunction, the results were similar (OR 3.2; 95% CI 1.2 to 8.5). Multivariable logistic regression confirmed that elevated lactate (OR 5.3; 95% CI 1.9 to 14.4; p=0.001) had an independent association with risk of PE-related complications during 7 days of follow-up, after adjustment for the other significant covariates of RV dysfunction and tachycardia at the time of acute PE diagnosis (table 3). A lactate concentration of 2 mmol/L or more at the time of presentation was also independently significantly associated with 30-day all-cause (OR 2.5; 95% CI 1.1 to 5.5; p=0.024) and PE-related (OR 4.6; 95% CI 1.3 to 15.8; p=0.015) death.
Unadjusted and adjusted ORs for 7-day PE-related complications in normotensive patients with acute symptomatic PE

Frequency of the primary outcome according to baseline lactate levels.
Incremental prognostic value of plasma lactate
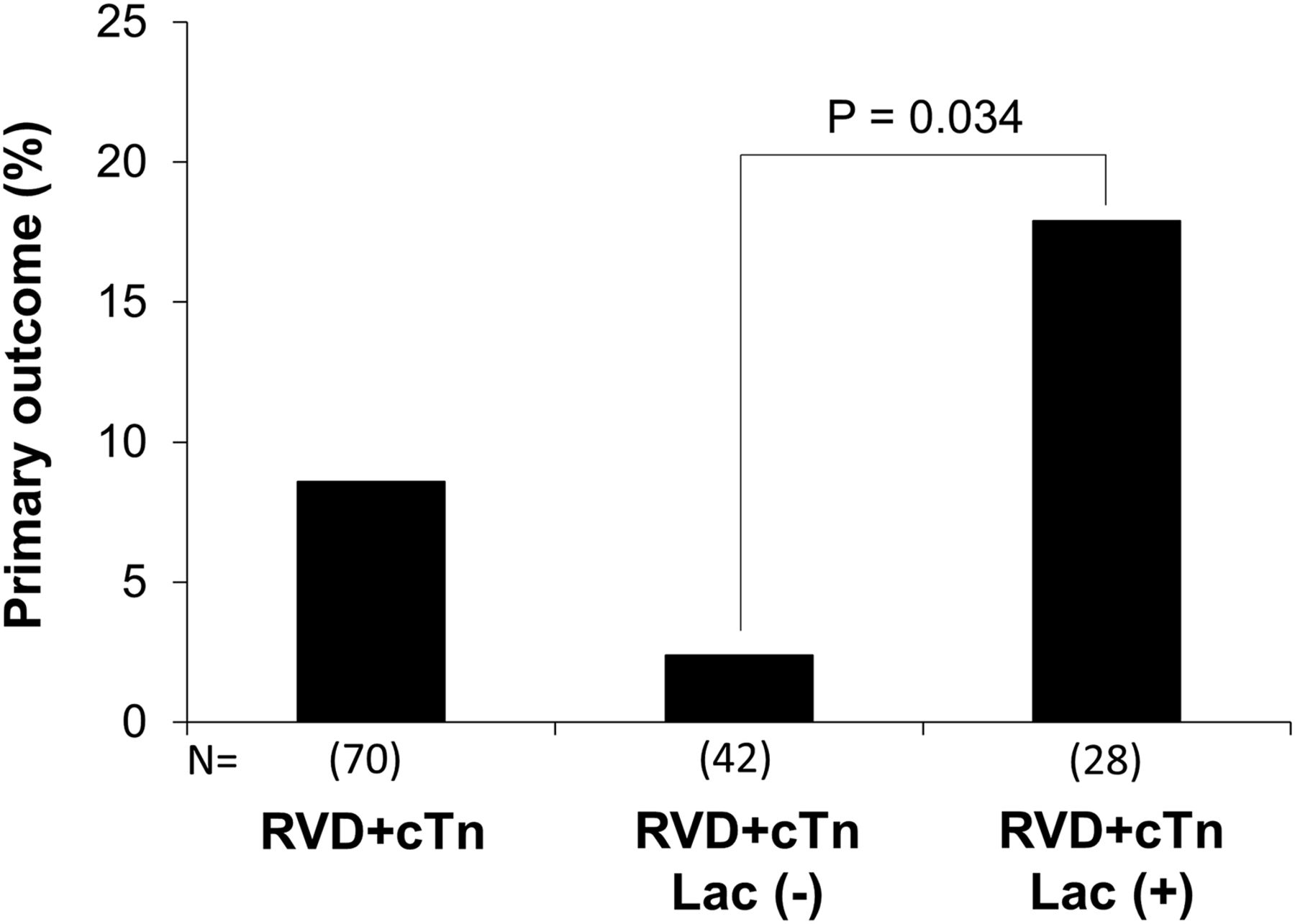
The above results suggest that lactate levels alone are per se independent predictors of the primary outcome. Overall, the positive predictive value of lactate (with the use of the above cut-off point) was 10.4% for the primary end point (table 4). By combining the prognostic information provided by sPESI and lactate, we found that, of 108 patients (21.8% of the entire study population) with an sPESI ≥1 point and lactate levels ≥2 mmol/L, 12 (11.1%; 95% CI 7.0% to 13.9%) experienced the primary outcome (table 4). Multiple logistic regression analysis revealed that the combination of RV dysfunction and a positive troponin was associated with a 2.8-fold (95% CI 1.0 to 7.4) elevated risk of the primary outcome, which increased to 6.6-fold (95% CI 2.2 to 19.6) in the presence of lactate elevation. The primary outcome rate of the combination of an RV dysfunction and a positive troponin was 8.6%, but increased to 17.9% for patients also presenting elevated lactate levels (p=0.034; table 4; figure 3).
Prediction rule test characteristics for 7-day PE-related complications in 496 normotensive patients with acute symptomatic PE

{kind=link}
{kind=link}
{kind=link}
Escalation of PE-related complication rates depending on lactate levels in combination with echocardiography and troponin. cTn, elevated cardiac troponin; Lac (+), lactate ≥2 mmol/L; Lac (−), lactate <2 mmol/L; RVD, right ventricular dysfunction.
Discussion
This large European multicentre prospective cohort study shows that raised lactate is an independent predictor of PE-related mortality or clinical deterioration in normotensive patients with PE. The combination of RV dysfunction, elevated troponin and increased lactate predicted a 6.6-fold increase in the risk of adverse short-term PE-related adverse events.
A validated explicit clinical prediction rule that recognises a group of normotensive patients at high risk of adverse clinical events that might benefit from recanalisation procedures is still lacking. Previous observational studies have suggested a role for RV dysfunction and injury markers, either alone4–7 or in combination with clinical variables.18–20 The PE Thrombolysis Trial (PEITHO) determined the efficacy and safety of early thrombolytic treatment in normotensive patients with RV dysfunction and myocardial injury.9 This trial clarified the risk of death in patients with acute PE who were initially normotensive and had myocardial injury and RV dysfunction. The rate of death from any cause during the first 7 days was low (1.2% in the fibrinolysis group and 1.8% in the placebo group). The low mortality rate among patients who received anticoagulants strengthens the case for fine-tuning risk stratification.
Persistent tissue hypoxia, by favouring the transition from a reversible to an irreversible cell injury, is one of the main determinants of adverse outcome in critically ill patients,21 and plasma lactate concentration is one of the most sensitive markers of tissue hypoxia.22 ,23 Serum lactate levels ≥2 mmol/L reflect inadequate tissue oxygenation,23 and this cut-off value has been proposed for PE and other disease states (eg, sepsis).11 ,24 ,25
Prior evidence suggests an association between elevated lactate at the time of PE diagnosis and prognosis.14 ,15 For example, the Vanni et al15 prospective study of 270 consecutive stable and unstable patients with PE found an independent association between plasma lactate and 30-day all-cause mortality. Our study found normal plasma lactate concentrations (<2 mmol/L) in 63% of the 496 investigated cases, and these patients had a 98.3% negative predictive value for PE-related complications. Although our results indicate that lactate testing identifies patients with stable PE who are at very low risk of PE-related medical outcomes, prognostic tools should ideally predict all-cause mortality, recurrent venous thromboembolism, and major bleeding soon after diagnosis (eg, in the first 7–14 days) in patients being considered for outpatient therapy for PE.
In this study, patients with elevated lactate had a PE-related complication rate of ∼10%. This positive predictive value did not significantly differ from that of other single tests (eg, cTnI, echocardiogram) for prediction of short-term PE-related complications.26 ,27 Hence, high lactate per se should not significantly drive the decision to give thrombolytic therapy, and the current evidence does not support the use of lactate levels for such decision-making. Instead, our results show that lactate levels are likely to be most useful when used in combination with echocardiographic evidence of RV strain, and with markers of myocardial injury. Indeed, we found that the association of elevated troponin, RV dysfunction and elevated lactate predicted a 6.6-fold increase in the risk of 7-day PE-related adverse events, with a positive predictive value of 17.9%. Thus, the combination of RV dysfunction and elevated troponin and lactate levels contributed to fine-tuning of risk stratification for normotensive patients with acute symptomatic PE.
Strengths of our analysis that increase the precision and validity of the present findings are that (a) we included data from a large number of participants, (b) baseline variables were recorded at enrolment rather than retrospectively, and (c) participants were followed prospectively. Furthermore, an adjudication committee accurately diagnosed outcomes. Compared with previous studies,14 ,15 our study's large sample size, the adjustment for potential confounders (eg, troponin, RV dysfunction), and the robustness of the findings provides strong evidence supporting the concept that measurement of lactate at the time of acute PE diagnosis is a predictor of short-term PE-related complications.
Some methodological limitations should be considered. First, the incidence of the primary outcome was lower than expected, partially reducing the statistical power of the sample size. Second, we did not address the prognostic relevance of repeated measurements of lactate, which are reported to have higher accuracy than a single one.23 In addition, the model did not address the prognostic relevance of other factors that may affect decision-making, such as assessment of the thrombotic burden (eg, concomitant deep vein thrombosis, extension of emboli in the pulmonary tree, RV dysfunction assessed by multidetector CT)28 ,29 and of haemorrhagic risk factors. Finally, although some clinicians might perceive an arterial blood gas analysis as an invasive procedure, it is a common investigation for patients with suspected PE. Future studies might address whether clinicians ought to conduct an arterial analysis only for selected PE patients (eg, high-risk sPESI patients) and whether venous lactate determination could replace arterial analysis30 for the sake of conducting appropriate testing, avoiding unnecessary testing and treatments, and improving cost-effectiveness.
In summary, the present study demonstrates that plasma lactate measurement represents a powerful predictor of short-term PE-related complications. In normotensive patients with acute PE, the combination of high troponin, echocardiographic RV dysfunction and high lactate identifies a small subgroup of normotensive patients at high risk of short-term PE-related adverse events. Prospective studies should further address the safety and efficacy of early recanalisation procedures for normotensive patients with PE who are identified using these criteria.
References
Footnotes
-
Contributors Study concept and design: SV, DJ, PN and SG. Acquisition of data, analysis and interpretation of data, statistical analysis: SV, DJ, PN, FM, MP, ED, RL, PB, JLL, LJ-P, AKP and SG. Drafting of the manuscript: SV and DJ. Critical revision of the manuscript for important intellectual content: SV, DJ, PN, FM, MP, ED, RL, PB, JLL, LJ-P, AKP and SG. Study supervision: SV and SG.
-
Funding NEUMOMADRID (2012) and SEPAR (2012) provided funding for the study.
-
Competing interests None.
-
Ethics approval Ethics Committee of Azienda Ospedaliero Universitaria Careggi.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The corresponding author, SV, had full access to all the data in the study.