Article Text

Statistics from Altmetric.com
- Bronchoscopy
- Cough/Mechanisms/Pharmacology
- Imaging/CT MRI etc
- Lung Physiology
- Respiratory Measurement
- Thoracic Surgery
CLINICAL PRESENTATION
A 50-year-old woman was referred with a three-year history of cough, difficulty clearing secretions and intermittent wheeze. Examination revealed normal breath sounds and a chest radiograph was normal.
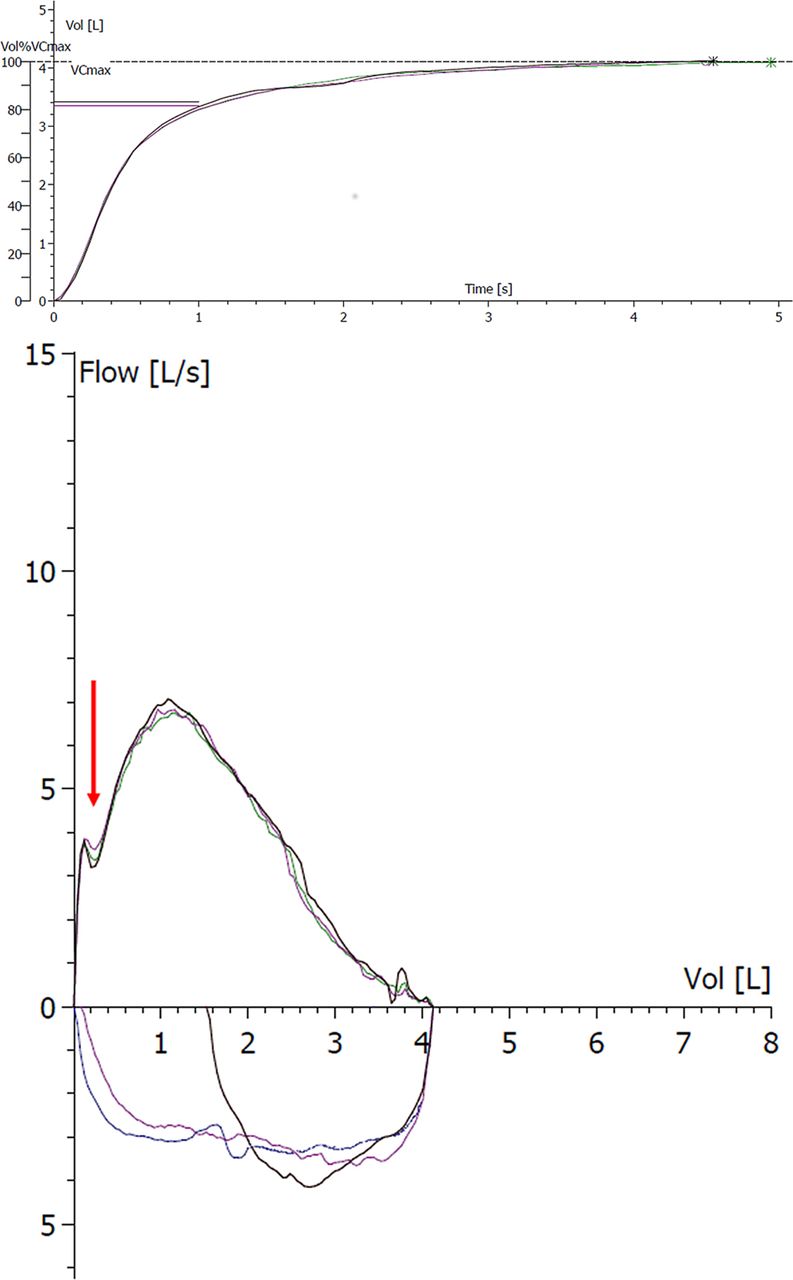
Clinic spirometry revealed a normal volume–time spirogram (figure 1A) with supra-normal indices: FEV1 3.4 L (119% predicted) and FVC 4.1 L (123% predicted).

(A) Volume–time spirograph. (B) Reproducible early expiratory notch (red arrow) on flow–volume loops.
Full lung function testing was arranged and the flow–volume loop was immediately flagged as abnormal; demonstrating a reproducible notch in the early forced expiratory phase of the manoeuvre (figure 1B).
QUESTION
What is causing the highlighted abnormality and how would you investigate further to confirm your suspicions?
For the answer see page 304.
From the question on page 302
ANSWER
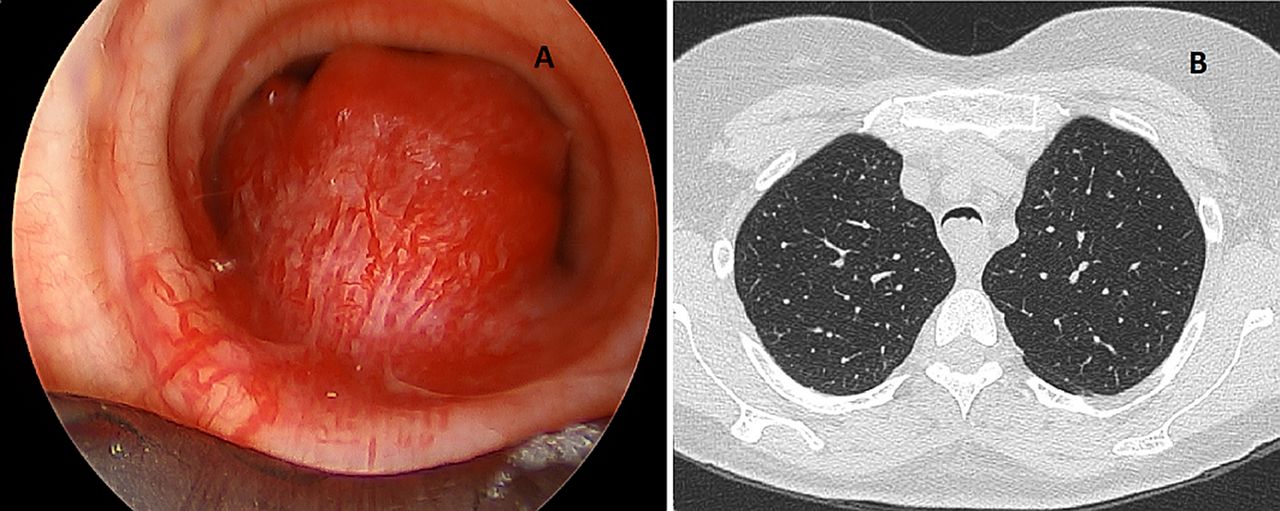
The notch in the flow–volume curve suggested a potential ‘ball-valve’ effect on flow (figure 1B) and triggered a request for a computed tomography scan of the thorax. This demonstrated an obstructive mass, virtually occluding the cervical trachea (figure 2A).
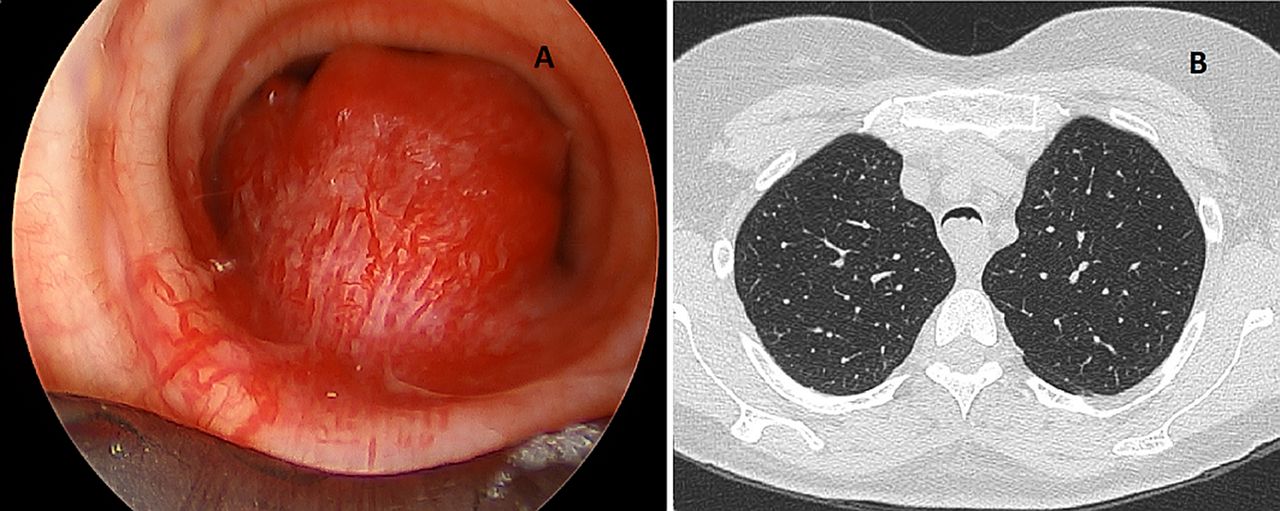
(A) Tracheal mass virtually occluding the airway at the level of the aortic outlet on axial CT thorax. (B) Highly vascular endotracheal mass visualised at bronchoscopy.
Rigid bronchoscopy revealed a highly vascular and pedunculated neoplasm arising from the posterior peri-membranous wall of the trachea (figure 2B). This was de-bulked and histology with immunoprofiling (positive smooth muscle antibody; negative cytokeratin, CD56, Desmin, CD34 and S100) was consistent with a low-grade glomus tumour. These neoplastic proliferations comprise cells resembling smooth muscle of the normal glomus body and are an extremely rare cause of tracheal obstruction, with fewer than 20 reports in the literature.1 Glomus tumours are predominantly benign with little propensity for local invasion or metastatic spread.1 The prognosis for patients with tracheal glomus tumour undergoing surgical resection is good with low recurrence rates if surgical margins are maintained.2
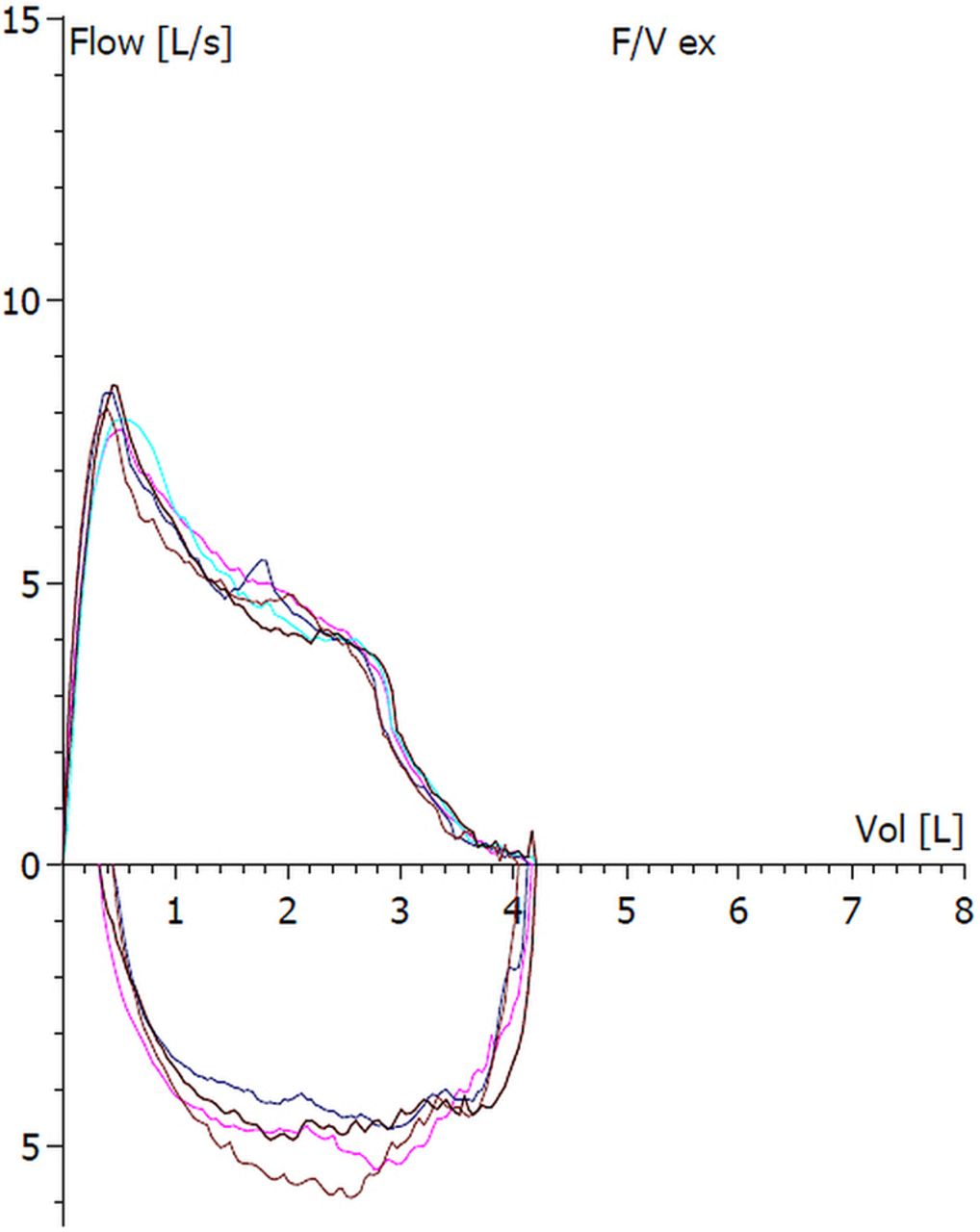
Repeat spirometry demonstrated resolution of the notch with absolute spirometric indices that were unchanged (figure 3).

{kind=link}
{kind=link}
{kind=link}
Flow–volume loop following de-bulking procedure.
It is well recognised that flow–volume loops can highlight the presence of either fixed or variable pathology in the central airways and as such act as a ‘window to the airway’.3 In the case described, close scrutiny of all aspects of the loop revealed a reproducible defect in flow and thus expedited investigation and ultimately the detection of a tracheal neoplasm. The case illustrates that such abnormalities may be overlooked by a clinic approach that simply depends on absolute spirometric indices and evaluation of a volume–time spirogram.
Footnotes
-
Contributors CO: principle author. Responsible for content as guarantor. Wrote first draft of the scientific case report, performed literature review and assessed relevance of report to established literature. SW: interpreted lung function and reviewed article. SJ: contributed endoscopic images of tracheal tumour. AM-G: contributed to article writing and review. JH: article supervisor. Oversaw writing of article and contributed to review process.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Airwaves