Article Text

Abstract
Introduction Patients with COPD commonly exhibit pursed-lip breathing during exercise, a strategy that, by increasing intrinsic positive end-expiratory pressure, may optimise lung mechanics and exercise tolerance. A similar role for laryngeal narrowing in modulating exercise airways resistance and the respiratory cycle volume–time course is postulated, yet remains unstudied in COPD. The aim of this study was to assess the characteristics of laryngeal narrowing and its role in exercise intolerance and dynamic hyperinflation in COPD.
Methods We studied 19 patients (n=8 mild–moderate; n=11 severe COPD) and healthy age and sex matched controls (n=11). Baseline physiological characteristics and clinical status were assessed prior to an incremental maximal cardiopulmonary exercise test with continuous laryngoscopy. Laryngeal narrowing measures were calculated at the glottic and supra-glottic aperture at rest and peak exercise.
Results At rest, expiratory laryngeal narrowing was pronounced at the glottic level in patients and related to FEV1 in the whole cohort (r=−0.71, p<0.001) and patients alone (r=−0.53, p=0.018). During exercise, glottic narrowing was inversely related to peak ventilation in all subjects (r=−0.55, p=0.0015) and patients (r=−0.71, p<0.001) and peak exercise tidal volume (r=−0.58, p=0.0062 and r=−0.55, p=0.0076, respectively). Exercise glottic narrowing was also inversely related to peak oxygen uptake (% predicted) in all subjects (r=−0.65, p<0.001) and patients considered alone (r=−0.58, p=0.014). Exercise inspiratory duty cycle was related to exercise glottic narrowing for all subjects (r=−0.69, p<0.001) and patients (r=−0.62, p<0.001).
Conclusions Dynamic laryngeal narrowing during expiration is prevalent in patients with COPD and is related to disease severity, respiratory duty cycle and exercise capacity.
- Respiratory Measurement
- Exercise
- COPD ÀÜ Mechanisms
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is the key question?
-
What is the role of laryngeal narrowing in the regulation of ventilation during exercise in patients with COPD?
What is the bottom line?
-
Dynamic laryngeal narrowing during expiration is prevalent in subjects with moderate or severe COPD and relates to lung emptying and dynamic hyperinflation during exercise, suggesting this could be a newly identified mechanism by which patients offset intrinsic positive end-expiratory pressure.
Why read on?
-
This is the first study to describe the active role of the larynx in regulating lung emptying and ventilation during exercise in COPD and highlights potential implications for exercise intolerance.
Introduction
Dynamic hyperinflation (DH) and in particular the loss of inspiratory reserve volume are recognised features in the aetiology of the dyspnoea and exercise limitation in COPD.1–3 Strategies which reduce DH, including drugs4 and lung volume reduction5 improve exercise performance in COPD.
Pursed-lip breathing is a strategy which patients can employ to create intrinsic positive end-expiratory pressure (PEEPi).6 Although the mechanics of this manoeuvre have not been fully studied, pursed lip breathing at rest is associated with a prolonged expiratory time, an increased tidal volume (VT) and reduced end expiratory chest wall volumes, presumably because the creation of PEEPi allows greater expiratory flow.7 The adoption of a pursed lip breathing strategy may also be associated with improved exercise tolerance.8
In health, the functional neural control of the larynx and respiratory musculature are closely aligned, so that diaphragmatic contraction and laryngeal abduction occur in virtual synchrony. Nevertheless, even in healthy subjects, there is a minor reduction in glottic aperture during passive expiration9–11 and a tight coupling between the movement of the vocal cords and the phase and pattern of volume change within the respiratory cycle.9
Little is known about the behaviour of the larynx in patients with COPD; Higenbottam and Payne12 studied 34 patients with obstructive lung disease and observed expiratory narrowing of the glottis at rest, while Campbell et al13 hypothesised a similar mechanism based on measures of upper airway resistance. The laryngeal response to physical exertion in patients with COPD has never been studied. However, the occurrence of laryngeal narrowing during the expiratory phase of respiration may be relevant and, by increasing PEEPi, serves to ‘splint’ the airway12 ,14 ,15; this may be relevant in the presence or absence of pursed lip breathing, that is, glottic narrowing is a possible additional mechanism acting to optimise operational lung mechanics in COPD.
Technical advances now permit accurate continuous recording of laryngeal movement during exercise. More specifically, a technique termed the continuous laryngoscopy during exercise (CLE) test provides a feasible and safe method with which to obtain continuous acquisition of laryngeal movement from a nasendoscope view in a fixed position.16 This technique allows a comparative assessment of dynamic laryngeal movement in response to exposure to physiological stress, for example, exercise.
The aim of this study was to evaluate dynamic movements of the larynx in patients with COPD and to evaluate relationships with static and dynamic lung function measures and exercise tolerance using a CLE technique. We hypothesised that laryngeal narrowing, during the expiratory phase of respiration, would be more prevalent in patients with COPD than healthy age-matched controls and relate to airflow obstruction. We also hypothesised that this laryngeal narrowing would occur predominantly at the vocal cord level and become more pronounced during exercise, relating to indices of DH.
Methods
Study population
Subjects with confirmed COPD on the basis of a positive smoking history, symptoms and lung function17 were recruited from the Royal Brompton Hospital at a time of clinical stability; that is, no exacerbation in the month prior to study. Subjects with a present or past history of cardiac disease, laryngeal disease or use of maintenance oxygen or ventilatory support were excluded. In addition, healthy age-matched volunteers, free from significant respiratory (FEV1>80% predicted), cardiovascular or metabolic disease were recruited from a departmental database. Subjects provided written informed consent and the study was approved by the Local Research Ethics Committee (11/LO/1404).
Study design and procedures
Subjects attended the laboratory on one occasion for clinical assessment including COPD assessment test,18 lung function measures and a CLE test. Anthropometric characteristics were recorded and spirometry was performed on the day in all patients and controls in accordance with recommendations19 (Microlab 3300 Spirometer, Micro Medical, Rochester, UK). Static lung volumes and gas transfer measures were used if they had been taken within 1 year of the assessment date.
Exercise procedures: laryngoscopy during exercise
Continuous laryngoscopy testing was performed based on previous methodology.16 In brief, the larynx was visualised by placing a fibreoptic nasenodoscope (Olympus ENF-VQ, Olympus, Japan) in the posterior nasopharynx and securing it using specialist headgear (see figure E1 in the online data supplement). Video images were thereafter continuously recorded (MediCap USB 200, Medicapture, USA). Subjects then performed an incremental maximal cycle-ergometer cardiopulmonary exercise test with cardiorespiratory measurement according to accepted definitions.20 Operational lung volumes were determined from inspiratory capacity (IC) manoeuvres performed every 2 min, to calculate the dynamic hyperinflation index (DHI).21
Laryngeal movement analysis
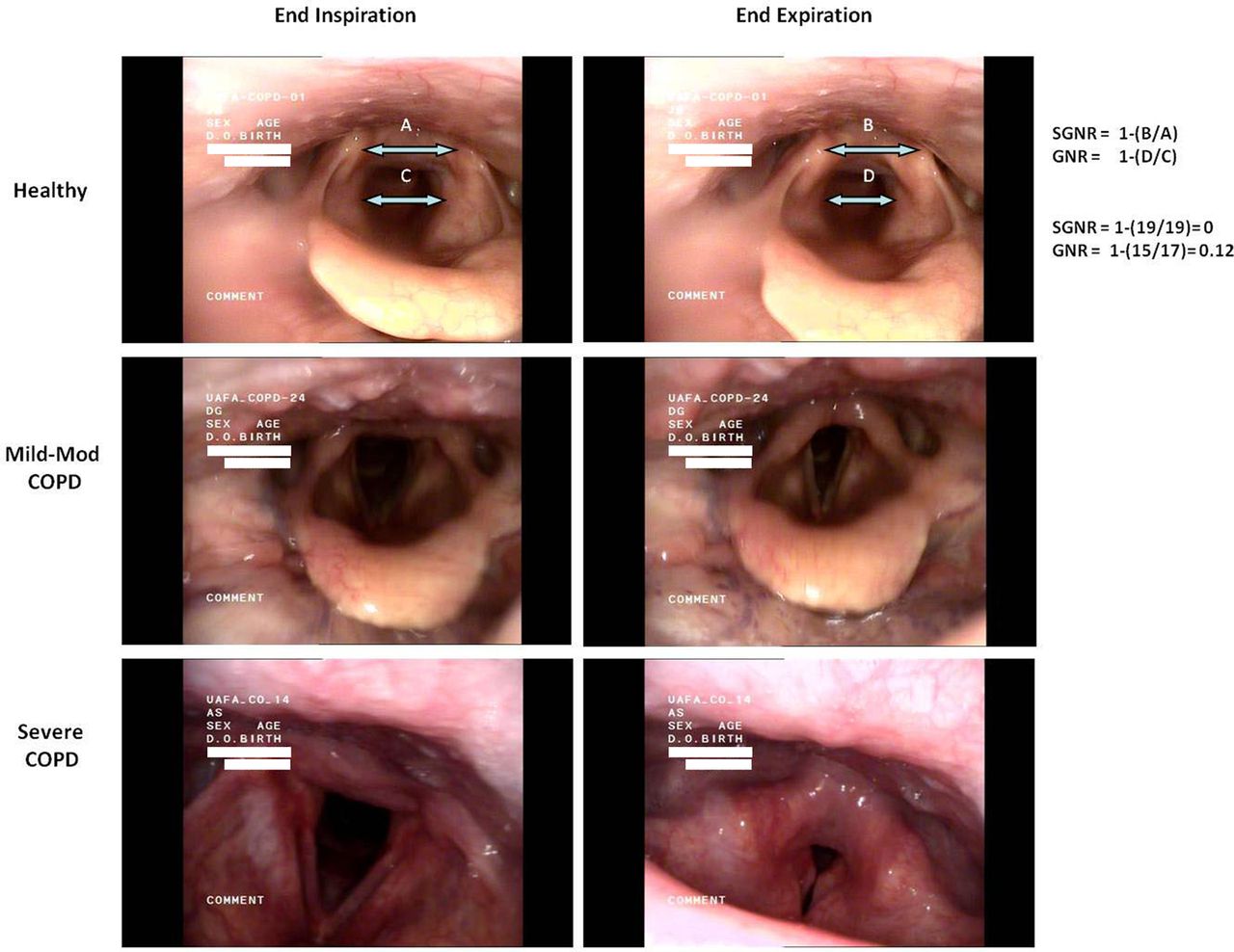
Image stills were taken from the continuous recording, at end inspiration and end expiration. Breathing cycle was verified by corresponding pneumotachograph flow data. An expiratory narrowing ratio was calculated for the glottic (distance between vocal folds at the mid-point of their length, glottic narrowing ratio, GNR) and supra-glottic apertures (distance between the medial margin of the arytaenoid cartilage, SGNR) as equal to 1-aperture measurements at end expiration divided by the width at end inspiration (figure 1); whereby a narrowing ratio of 1=complete narrowing and 0=no change. This ratio provides a measure of the narrowing of the laryngeal structures in relative terms during one breathing cycle, which is independent of the distance between the laryngoscope and the glottis. Peak exercise images were taken from a breath sequence considered representative of the last 30 s of exercise and free of artefact (eg, coughing).

Example cases illustrating dynamic expiratory laryngeal narrowing and method for calculation of glottic and supra-glottic narrowing ratio.
Narrowing scores were determined as the mean of scores reported independently by two observers (AMG and GH), blinded to subject characteristics.
Statistical analysis
Data are expressed as mean (SEM) unless otherwise stated. Differences in continuous variables were assessed using Student's t test and/or one-way analysis of variance with Tukey post hoc analysis or the non-parametric equivalent. Groups were analysed as healthy, mild–moderate COPD (Global Initiative for Chronic Obstructive Lung Disease (GOLD) 1–2) and severe COPD (GOLD 3–4). Correlation was assessed by Pearson or Spearman's rank methods. Statistical calculations were made with GraphPad Prism V.5.0 (GraphPad Software, San Diego, California, USA) and SPSS V.21 (SPSS Inc., Chicago, Illinois, USA). Significance is reported at p<0.05.
Results
Subject characteristics and resting measurements
Thirty-four subjects were recruited, however technically adequate data were only obtained for 30 subjects (n=11 healthy; n=8 mild–moderate COPD; n=11 severe COPD) (table 1). Reasons for inadequate data were poor visualisation secondary to secretions (n=2) and inability to complete CLE (n=2). All patients were prescribed regular inhaled β-2 agonist therapy and 79% were prescribed long-acting β agonist/inhaled corticosteroid and long-acting muscarinic antagonist maintenance therapy. Patients had a median (range) 35 (15–60) pack-year smoking history.
Subject characteristics and pulmonary function
Patients and controls were well matched for age, sex, height and body mass index (BMI, all p>0.05). However, as expected, patients reported a heightened symptom burden; median (range) CAT score in healthy subjects, 4 (0–9) and patients 19 (4–31) (p<0.001). They also had impaired pulmonary function (p=0.0086) and baseline oxygen saturation (p=0.013) compared with control subjects (table 1).
Exercise measurements
As expected, patients demonstrated a reduced peak work rate and oxygen uptake compared with healthy controls: 60±8 W and 13.7±0.8 mL/min/kg and 133±15 W and 24.6±1.8 mL/kg/min respectively (both p<0.001). The majority of patients (79%) stopped exercise because of dyspnoea and exhibited evidence of ventilatory limitation to exercise capacity.
IC manoeuvres during exercise were not satisfactory in two patients; the remainder demonstrated evidence of DH as indicated by a mean (SEM) reduction in IC of COPD group +0.35±0.07 L (p<0.01 compared with controls) and DHI, healthy −0.01±0.06 compared with all patients with COPD 0.75±0.18 (p<0.01) (table 2). DHI was directly related to FEV1 for all subjects (r=−0.46, p=0.024).
Selected parameters at peak exercise
Laryngeal movement analysis
Rest
In healthy subjects, there was a median (range) percentage reduction in GNR during expiration of 10% (0–52%) (figures 1 and 2 and table 3). This narrowing was more pronounced in patients: 50% (4%–92%) (p<0.001) (table 3). A similar relationship was apparent at the supra-glottic level, although overall narrowing was less marked in all subjects; that is, predominant narrowing was at the glottic level. There was no relationship between either GNR or SGNR and age, height, BMI (all p>0.05). Likewise there was no difference in GNR or SGNR between male and female subjects.
Laryngeal narrowing ratios at rest and peak exercise

Laryngeal narrowing ratio at rest and peak exercise at glottic (A) and supraglottic (B) level.
There was a correlation between the resting GNR and the FEV1 in the whole cohort (r=−0.71, p<0.001) and the patients with COPD considered alone (r=−0.53, p=0.018) (figure 3A). In all subjects a correlation was seen between markers of gas trapping and GNR, however this was not seen for patients with COPD alone.

Relationship between FEV1% predicted and glottic narrowing ratio at rest (A) and peak exercise (B), and supra-glottic narrowing ratio at rest (C) and peak exercise (D).
In patients, there was no relationship between GNR and SGNR and COPD assessment tool. Moreover, an analysis of a subgroup of patients with excessive resting laryngeal narrowing (ie, >GNR 0.5 based on mean +2 SD of control data) revealed no significant difference in clinical or physiological characteristics (data not shown). A high level of inter-observer agreement for GNR scoring measures (r=0.93, p<0.0001) was observed (see figure E2 in the online data supplement).
Exercise
Exercise GNR and SGNR data are shown in table 3. There was no change in either GNR or SGNR between the resting and exercise phase in either healthy controls or patients (p>0.05) (table 3). Exercise GNR was inversely related to peak ventilation in all subjects (r=−0.55, p=0.0015) and patients (r=−0.71, p<0.001) and peak exercise VT (r=−0.58, p=0.0062 and r=−0.55, p=0.0076, respectively). Likewise exercise GNR was inversely related to peak VO2 (% predicted) in all subjects (r=−0.65, p<0.001) and patients alone (r=−0.58, p=0.014). A similar relationship was apparent for SGNR.
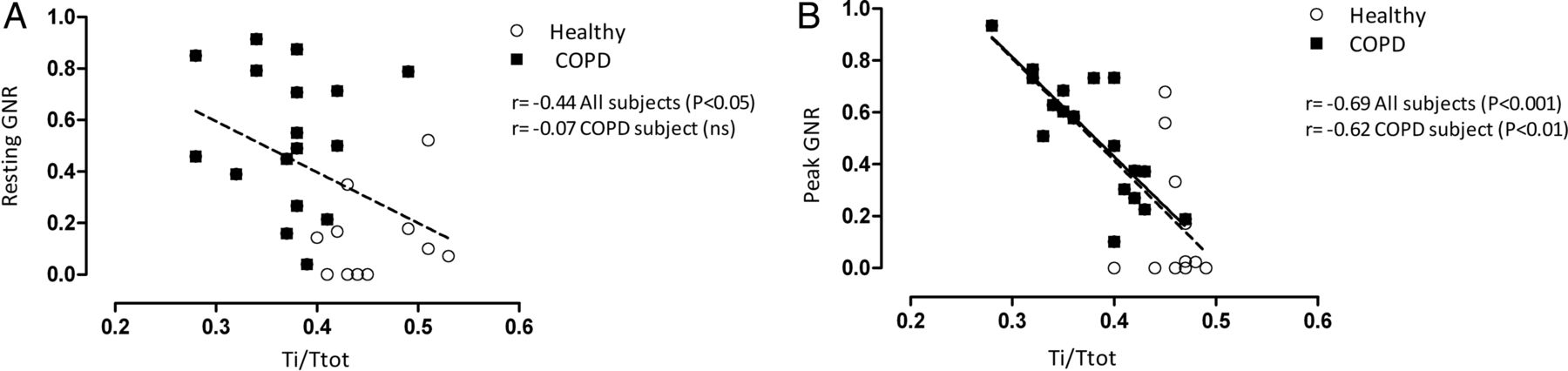
Exercise inspiratory duty cycle related to exercise GNR for all subjects (r=−0.69, p<0.001) and patients (r=−0.62, p<0.001) (figure 4). Change in GNR rest-peak and change in TI/TTOT were not related.

Relationship between respiratory duty cycle (TI/TTOT) and glottic narrowing ratio at rest (A) and peak exercise (B).
Patients with COPD and a significant exercise GNR (ie, >0.5) were no more likely to stop secondary to dyspnoea or report a higher peak exercise dyspnoea BORG score (p>0.05). Peak exercise GNR related to DHI if all subjects were considered together (r=0.45, p=0.018) but not if patients with COPD were considered alone (r=0.24, p=0.35) (figure 5). There was no difference in peak exercise GNR or SGNR between patients who demonstrated DH based on reduction in IC. There was no relationship between peak GNR and oxygen saturation and no significant difference in peak GNR between patients who de-saturated, that is, SpO2<94% (n=6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between peak glottic narrowing ratio (GNR) and dynamic hyperinflation index (DHI) in controls (•), patients with mild–moderate COPD (□) and patients with severe COPD (▪). Data are presented as mean values with error bars representing 1 SEM. *p<0.05 from controls.
Discussion
Dynamic laryngeal narrowing during expiration is prevalent in patients with COPD and is directly related to disease severity and exercise capacity. The reduction in laryngeal aperture arises predominantly from narrowing at the glottic level (ie, vocal cord narrowing) and was evident during quiet breathing at rest. During exercise, glottic narrowing relates to indices of DH and interestingly the relationship between GNR and TI/TTOT became closer during exercise suggesting that glottic narrowing exerts functional consequences which may be beneficial if associated with increased PEEPi.
Critique of the method
It has been posited that close neurophysiological coupling between anatomical components of the airway tract and the expiratory muscles functions to optimise airflow and respiratory loading at rest and during exercise.9 ,22 ,23 Moreover it has been proposed that, because of its variable resistance, the larynx may aid the post-inspiratory activity of the diaphragm to control end-expiratory lung volume.24 In animal studies the recurrent laryngeal nerve demonstrates impulse traffic during expiration and the laryngeal adductors or the arytaenoid cartilages show heightened expiratory phase activity.22 Of note in patients with COPD, expiratory muscle recruitment is heterogeneous, perhaps explaining observed variance in glottic narrowing.25 ,26
Our observation that glottic narrowing did not worsen with exercise was unexpected. Our patients knew that they were about to exercise and we therefore acknowledge that this observation may also be explained by the fact that there is early neural activation with glottic adaptation prior to exercise onset. However, we suspect more likely that, for patients with severe disease, it is possible that the larynx is providing optimal flow control consistent with balancing the need to expire air whilst simultaneously creating PEEPi even at rest. This concept would also explain why, on exertion, some patients use pursed-lip breathing to provide additional resistance. It would be informative to evaluate laryngeal narrowing indices during steady-state exercise at iso-ventilation and in addition during walking exercise. Laryngoscopic examination without a mouthpiece in situ would also be informative to evaluate the relationship and interaction between any development of pursed lip breathing and glottic narrowing.
Previous studies in healthy adults specifically evaluating the influence of lung volume change indicate that glottic aperture increases in line with lung inflation,11 ,27 ,28 so we do not think this would explain the current findings. Our patients with severe COPD had evidence of hyperinflation on their static lung function tests; it is unclear what influence this has over glottic function.
Blood gas tensions could potentially influence glottic function. England et al29 evaluated the role of altered oxygen and carbon dioxide tensions on laryngeal function in healthy humans. They concluded that hypoxic stimulation of peripheral chemoreceptors precipitated expiratory glottic narrowing and resulted in a relatively high laryngeal airflow resistance. In contrast, hypercapnia was accompanied by a low expiratory laryngeal resistance. Although we did not obtain arterial gas tensions in the current study, oxygen saturation was assessed as part of the cardiopulmonary exercise testing performed and we found no relationship between exercise oxygen saturation and glottic narrowing.
It is conceivable that the testing methodology employed (ie, direct laryngoscopy during exercise) may have played a role in precipitating the development of the laryngeal narrowing, although prior studies in which laryngeal resistance has been measured would argue against this, and would not explain observed differences between patients and controls. Moreover, it is possible that use of a flow turbine mouthpiece during exercise testing and the requirement to perform periodic IC manoeuvres influenced laryngeal function and respiratory-laryngeal neural recruitment. To address this consideration, we obtained video recording images in patients with and without the mouthpiece in situ and found no significant difference in the degree or magnitude of glottic narrowing in these individuals, either at rest or near to peak exercise. Moreover, in contrast to prior studies,14 every care was taken to ensure local anaesthetic was only applied to the nares.
Our analysis was based on the GNR and SGNR as detailed above. We also undertook analysis expressing the inspiratory and expiratory distances as a percentage reduction in aperture (ie, {(b–a)/a}×100) as opposed to (1–b/a) but our conclusions were unchanged (data not shown).
Significance of the findings
Prior research has evaluated respiratory movement of the glottis, using either direct visualisation techniques or indirectly inferring laryngeal narrowing from alterations in upper airway resistance measures,12 ,13 ,30 ,31 which provide no information regarding the level at which obstruction occurs. Specifically, Higenbottam and Payne12 demonstrated a relationship between spirometric indices of airflow and glottic narrowing using a bronchoscopic technique in patients, but at rest in a semi-recumbent position with laryngeal anaesthetic applied.
Our findings, in a clinically pragmatic setting, specifically the seated position with no sedation or laryngeal anaesthesia, reveal dynamic laryngeal narrowing to be present both at rest and during exercise in a well characterised population of patients with COPD. A direct relationship was found between glottic narrowing and disease severity, as classified by FEV1, lung volumes or gas transfer. Moreover, this is the first study to provide a description of the anatomical location of glottic narrowing. This is pertinent given that in the condition of exercise-induced laryngeal obstruction, it is recognised that narrowing occurs predominantly at the supraglottic level (ie, arytaenoid level).16 In contrast, in our patients, it is apparent that while expiratory narrowing occurs at both the glottic and supraglottic levels, glottic narrowing predominates.
The current study is also the first to describe laryngeal performance in patients with COPD during exercise. Exercise hyperpnoea results not only in increased minute ventilation but has sequelae for airway turbulence, pulmonary receptor activation and respiratory muscle loading, as well as upstream neural activation relevant to the control of breathing.32 Several important functional adaptations are recognised to occur in the larynx in the context of exercise notably increased activity of the laryngeal abductor muscles, acting to minimise turbulence and airways resistance.33
We hypothesised that in COPD the laryngeal aperture would close further in response to exercise in patients with COPD to counter the development of DH. However, in contrast, we found no significant change in glottic dimensions during exercise and certainly little further reduction in glottic aperture in patients at peak exercise. Despite the absence of a macroscopic change in glottic aperture it is noteworthy that the relationship between GNR and both FEV1% predicted and TI/TTOT is closer during exercise than at rest (figure 4B). We speculate that this represents fine-tuning of the glottic aperture to preserve a balance between optimal expiratory flow and PEEPi. In a prior study in six healthy subjects and three with mild airflow obstruction, Pellegrino et al34 found evidence of flow limitation during tidal breathing. Moreover they observed that the addition of an expiratory threshold load resulted in a reduction in end-expiratory lung volume; likely relating to an impact on the time constraints of lung emptying. The laryngeal narrowing observed in the current study would be consistent with the hypothesis that the glottis acts similarly to modulate loading. In the future we suggest this could be explored by studying the relationship between PEEPi measured using an oesophageal balloon and applied levels of external PEEP during CLE. This is in contrast to findings during hyperpnoea in young healthy subjects in which this provocation is associated with glottic dilatation.10
In a model, which in some respects simulates COPD, Brancatisano et al24 previously demonstrated that breathing with an expiratory resistive load also enhanced glottic narrowing during expiration in healthy subjects. The authors commented that the expiratory glottic narrowing in response to expiratory resistive loads was in proportion to the prolongation in expiration (as in our patients) and that this effect appears due to a reflex modulated by change in the rate of lung emptying.
The role of expiratory loading on glottic function in COPD is yet to be studied. Non-invasive ventilation has an established role in the treatment of patients with COPD, both in terms of acute and chronic hypercapnic respiratory failure but also to improve exercise tolerance. Most modern devices enforce some expiratory positive airway pressure (EPAP); the present data suggest that the relationship between glottic aperture and the optimal applied EPAP requires further study.
It has been previously commented that glottic narrowing may contribute to reduced indices on effort dependent measures.12 In healthy subjects, glottic widening has been observed during a forced manoeuver,35 indicating that simultaneous recruitment of the expiratory muscles and laryngeal abductors. Forced expiratory manoeuvres are associated with activation of the posterior cricoarytenoid and laryngeal adductors.
In patients with COPD, the use of breathing techniques that increase positive expiratory pressure such as ‘pursed-lip’ breathing has been recognised for decades, however the precise benefit of this technique remains debated.36 Garrod et al37 found no significant difference in 6-min walking distance in those employing pursed-lip breathing, but noted that pursed-lip breathing during exercise and recovery resulted in a lower respiratory rate after exercise and results in a quicker resolution of exercise-induced breathlessness compared with exercise without pursed-lip breathing. One would hypothesise that pursed-lip breathing would be less useful in patients with substantial glottic narrowing, however we speculate that variability in pursed-lip breathing may represent heterogeneity of underlying glottic function.
Conclusion
Dynamic laryngeal narrowing during respiration, to some degree, appears to be almost ubiquitous in subjects with moderate or severe COPD. This expiratory phase narrowing occurs at the glottic level predominantly and changes little between rest and exercise. Further work should focus on establishing the mechanisms underlying this glottic narrowing and in particular its relationship with flow limitation and PEEPi. We believe that understanding laryngeal physiology better will allow the development of new therapies, and permit optimal application of existing therapies, in particular non-invasive ventilation.
Acknowledgments
We wish to thank the Lung Function Department Staff at the Royal Brompton Hospital for their assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
MB and GSH contributed equally, and MIP and JHH contributed equally.
-
Contributors All authors contributed to the design of the study, analysis of data and preparation of the final manuscript. MB, MIP and JHH conceived the idea and act as guarantors of the paper, taking responsibility for the integrity of the work as a whole, from inception to published article.
-
Funding The work was supported by the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College, London UK who part fund the salary of MIP. MB was supported by an ERS Long Term Research Fellowship (2012).
-
Competing interests None.
-
Ethics approval NRES London-Fulham Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.