Article Text

Abstract
Background Heterogeneous airway narrowing and closure are characteristics of asthma. However, they have never been quantified by direct measurements of parallel sister airways obtained from image data, and the anatomical basis of these processes remains unknown.
Methods Seven normal and nine asthmatic subjects underwent high-resolution CT, before and after methacholine challenge. Mean lumen areas of the entire airways were measured in 28 and 24 parallel sister airway pairs (a pair of airways arising from the same bifurcation) respectively (range 1.0–8.7 mm diameter). Heterogeneous narrowing was defined as the median difference in percentage narrowing between parallel sister airways. Forced oscillatory respiratory resistance (Rrs) and spirometry were measured before and after methacholine challenge conducted while supine.
Results The airways of asthmatics were smaller at baseline, and following bronchoconstriction there were similar decreases in FEV1, increases in Rrs and mean narrowing of airways for asthmatic and non-asthmatic groups. Non-asthmatics required higher doses of methacholine than asthmatics to achieve the same changes. However, parallel heterogeneity (median (IQR) 33% (27–53%) vs 11% (9–18%), p<0.001) and airway closure (24.1% and 7.7%, p=0.001, χ2) were greater in asthmatics versus non-asthmatics.
Conclusion We found clear evidence of differences in airway behaviour in the asthmatic group. Asthmatic airways were narrower at baseline and responded to inhaled methacholine by more heterogeneous narrowing of parallel sister airways and greater airway closure.
- Asthma
- Imaging/CT MRI etc
- Lung Physiology
- Asthma Mechanisms
Statistics from Altmetric.com
Key messages
What is the key question?
The concept of heterogeneous airway narrowing and ventilation as well as airway closure in asthma have been implicated in imaging, inert gas washout and modelling studies; however, despite a breadth of research in these areas, neither heterogeneity of ventilation nor airway narrowing have been directly observed or measured at the parallel sister airway level.
What is the bottom line?
High-resolution CT measurements of airway lumen area before and after bronchial challenge with methacholine obtained in nine asthmatic and seven normal subjects showed that despite similar methacholine-induced changes in FEV1 and Rrs, the airways of asthmatics narrowed more heterogeneously and closed more than the normal group.
Why read on?
The study provides direct evidence that the branching pattern of medium-sized and small-sized asthmatic airways narrow more heterogeneously, have a trend towards a broader frequency distribution of narrowing (more extreme narrowing and dilatation) and close more than normal airways.
Introduction
Asthma is characterised by intermittent airway narrowing and airway closure evident by changes in vital capacity and on ventilation imaging studies. Asthmatic airways also have an increase in the inherent asymmetry of airway calibres (heterogeneity)1–3 and there is evidence that this increase in heterogeneity is the basis of airway closure in asthma.4 Greater ventilation heterogeneity and airway closure during bronchoconstriction have been observed in asthmatic subjects in studies involving inert gas washouts,5 single-photon emission CT, positron emission tomography and MRI.6–10 Both ventilation heterogeneity and closure are related to asthma control and severity and airway hyperresponsiveness (AHR),1–4 but the anatomical basis of ventilation heterogeneity and closure is poorly understood. We can speculate, however, that there are either localised abnormalities related to remodelling or that there may be heterogeneous airway remodelling or heterogeneous changes to the mechanics of the airway wall or airway smooth muscle that cause sister airways to narrow or bronchodilate asymmetrically.
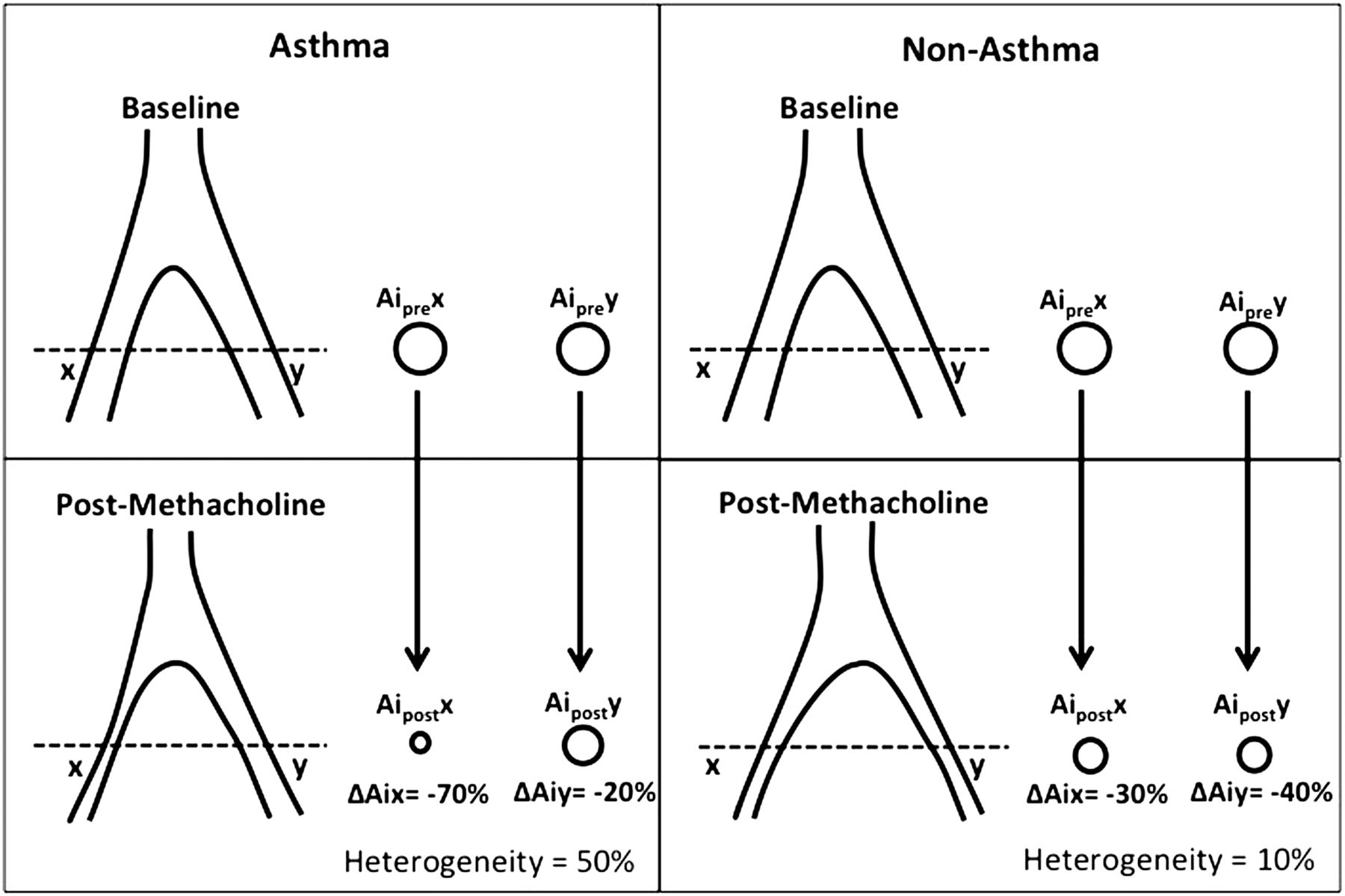
Inert gas washouts and ventilation imaging data are indirect measures of heterogeneity and closure and therefore do not provide definitive information on its anatomical basis. Our previous high-resolution CT (HRCT)11 study demonstrated that methacholine-induced airway narrowing was more heterogeneous in asthmatic subjects compared with non-asthmatic controls. However, that study measured airways that were not necessarily anatomically close and did not examine airway closure. It remains unknown whether parallel sister airways, that is, airways that bifurcate from a common parent airway (figure 1), exhibit more heterogeneous narrowing and closure during bronchoconstriction in asthma.

Circles represent cross-sectional appearance (at the level of the dashed line) of a sister airway pair (airway x and y) that arise from the same parent airway and which are oriented approximately perpendicular to the scanning plane. The percentage change in airway area is calculated for each sister airway and the absolute difference between the percentage changes is the heterogeneity of response.
Knowing whether parallel sister airways narrow heterogeneously and close in asthma is important because the function of airways that are near one another is inter-related via lung parenchymal interconnections between airways.12 These airway-to-airway interactions promote a state of local instability, where narrowing of an airway makes other airways around it more likely to narrow and to close, leading to sizeable parts of the lung that cease to ventilate. Importantly, heterogeneous narrowing and increased airway closure causes an exaggerated increase in lung resistance and stiffness for a given degree of bronchoconstriction,13 ,14 thus increasing the work of breathing.
In the present study, our aim was to compare the distribution of airway narrowing and extent of airway closure from volumetric helical HRCT images in asthmatic and non-asthmatic subjects, before and after methacholine-induced bronchoconstriction. We hypothesised that parallel sister airways arising from a single bifurcation in asthmatic subjects narrow more heterogeneously and are more likely to close during bronchoconstriction, compared with parallel sister airways of non-asthmatic subjects.
Methods
Nine asthmatic and seven healthy non-asthmatic subjects participated in the study. Asthma was defined by ATS/ERS guidelines,15 while all non-asthmatic participants denied a history of respiratory disease, symptoms and medication use. All participants were current non-smokers and had <5 pack-year smoking histories. Long-acting β agonists were withheld for at least 24 h and short-acting β agonists for at least 6 h prior to each visit. All participants provided written informed consent and the study protocol including radiation limit was approved by the Ethics Committee of the Royal Prince Alfred Hospital (Protocol No X01-0077).
Screening study
During the first visit, participants underwent skin prick testing (SPT), lung function testing and methacholine challenge. Atopy was defined as one or more positive reactions (mean wheal diameter ≥4 mm) to 14 common aeroallergens (Hollister-Stier Laboratories, LLC, Spokane, Washington, USA) on SPT. Airway calibre was measured by respiratory system resistance (Rrs) using the forced oscillation technique at 6 Hz and by spirometry (Spirocard, QRS Corp, Minneapolis, Minnesota, USA) in both seated and supine postures. Resistance was measured in both the upright and supine positions with cheeks supported and a noseclip in place during 1 min of tidal breathing from which the mean Rrs was calculated, using a forced oscillation device that has been previously described16 and reported using the predicted values of Pasker et al.17 Spirometry was performed according to ATS standards, using predicted values of Crapo et al.18
Methacholine challenge tests were then performed while participants were supine to replicate their posture during HRCT. Asthmatic participants underwent methacholine challenge tests by the rapid method19 where doubling doses of methacholine were administered by DeVilbiss number 45 hand-held nebulisers in cumulative doses ranging from 0.1 to 12 μmol. Non-asthmatic participants underwent high-dose challenges20 where doubling doses of methacholine were administered by DeVilbiss number 646 nebuliser using a Rosenthal nebulisation dosimeter in cumulative doses ranging from 0.1 to 200 μmol. AHR was measured as the provoking dose causing a 20% fall in FEV1 from baseline (PD20). Rrs then spirometry were measured at baseline and after each dose of methacholine. The challenge test was stopped after either a 20% decrease in FEV1 had occurred or the final dose had been administered, after which 200 μg of salbutamol was given by inhalation to reverse the airway narrowing. This test was used to determine the dose of methacholine to be administered as a single dose during HRCT.
HRCT scanning
Approximately 1 week after the first visit, participants underwent HRCT. Baseline spirometry was measured with the participant in a supine position on the scanning bed. Baseline HRCT scan of 2 cm of the lower lung zone beginning at the level of the carina was then acquired (single slice CTI Scanner, General Electric, Milwaukee, Wisconsin, USA) in helical mode using 120 kVp, 200 mAs, 1 mm collimation and 1 mm/s table speed, which yielded 20 contiguous 1 mm images. Participants were instructed not to move on the scanner table so that the airways would remain in the same orientation to the scanning plane between scans and not to take any deep breaths during the methacholine challenge test and prior to the HRCT scan, in order to avoid the bronchodilator effect of deep inspiration.21 The penultimate dose of methacholine which caused a >20% fall in FEV1 at the screening visit was then administered and the response measured by Rrs to achieve similar increases in Rrs as observed at the screening visit. Further small increments of methacholine were administered if there was insufficient change in Rrs. A second scan of the same 2 cm of lung was then performed. Post-challenge FEV1 was obtained from spirometry measured immediately after the second scan. Total radiation exposure for all HRCT scans was approximately 2.18 mSv.
In order to standardise lung volumes for the pre-challenge and post-challenge scans, participants were scanned at an artificially hyperinflated lung volume at baseline to match the point of expected lung volume post-methacholine. Hyperinflation is known to occur during bronchoconstriction and can influence airway calibre.22 ,23 For the baseline scan, participants inhaled to total lung capacity, then exhaled by the inspiratory capacity (IC) previously measured at the end of the challenge test at the screening visit, and then held their breath for scanning. For the post-methacholine scan, subjects exhaled to the end of a normal tidal breath and held their breath for 20 s during scanning. We assumed there to be a similar degree of hyperinflation during the methacholine challenges at both visits and this was checked by measuring spirometry, which included the IC, immediately following the post-methacholine scan.
Image processing and analyses
Images were reconstructed using a high-spatial frequency algorithm (General Electric ‘bone’ algorithm) at a reconstruction field of view of 20 cm, thickness of 1 mm and matrix size of 512×512 (pixel size 0.39×0.39 mm=0.15 mm2), centred on the right lung. Image data were transferred in Digital Imaging and Communications in Medicine format to a personal computer for image analyses (JRDC). Airway lumen area was measured using a semiautomated, threshold-dependent, edge-detection programme that had been previously calibrated against excised porcine lungs from which the 95% limits of agreement were ±3.2 mm2.24 ,25 The approximate centre pixel of the airway of interest was identified by the mouse cursor, from which all interconnected pixels with a density value of ≤110% of the seed pixel were identified. The average density value of all of these interconnected pixels was then calculated and all pixels that had a value of ≤90% of this value were identified as the lumen. This two-step procedure minimised any variability due to user identification of the seed pixel. The lumen area was calculated by multiplying the number of lumen pixels by the known pixel dimension. Radiological airway closure was determined when the lumen segmentation failed, and the airway lumen area was assigned as zero.
The mean lumen area of each airway (Aimean) was calculated from its origin at the proximal branch point to its end at the distal branch point. Airway narrowing and dilatation were measured as the percentage change in Aimean after methacholine challenge tests. Airway branch points were used as anatomical landmarks to identify the same airways from the baseline and post-methacholine scans and to locate sister (parallel) airways and their start and end.
Statistical analysis
Heterogeneity of changes in airway lumen area (Aimean) in response to methacholine was defined as the difference in percentage change in Aimean between all parallel sister airway pairs (figure 1). Where airway x and y are parallel sister airways arising from the same parent airway, and Aiprex is the mean radiological cross-sectional area of all slices of airway x from proximal to distal branch points at baseline, and Aiprey is the mean radiological cross-sectional area of airway y at baseline, heterogeneity of response to methacholine for parallel sister airway pairs (parallel heterogeneity) is calculated by the following equation:
In the asthma parallel sister airway example from figure 1, heterogeneity=abs(−70% to −20%)=50%.
Since there were no significant differences in heterogeneity between participants within asthmatic and non-asthmatic groups, data from all subjects in each group were combined. These data were non-normally distributed and so differences in heterogeneity between groups were examined using the Mann–Whitney U test and have been reported as the median and IQR.
Differences in mean airway response to methacholine between participants and between airways grouped by size, as defined by the idealised lumen diameter calculated (where  ), were examined using analysis of variance. The relationships between mean airway narrowing and heterogeneity, measured from Aimean and lung function, were examined using Pearson's correlation coefficient. The PD20 values were log transformed to normalise their distributions for all analyses.
), were examined using analysis of variance. The relationships between mean airway narrowing and heterogeneity, measured from Aimean and lung function, were examined using Pearson's correlation coefficient. The PD20 values were log transformed to normalise their distributions for all analyses.
All airways that were visible and approximately perpendicular to the scanning plane (not just the parallel sister airway pairs) were included in the analysis of airway closure. To calculate the differences in airway closure before and after methacholine challenge, all airways within the asthmatic and non-asthmatics groups were pooled. The number of airways that were closed were then expressed as a percentage of all airways measured within a group. Differences in airway closure between groups were compared using a Pearson's χ2 test.
Results
Table 1 shows the baseline lung function data as well as the changes in lung function during the methacholine challenge at the time of HRCT scanning. In the upright position, baseline FEV1 (%predicted) was lower in asthmatics (p=0.020), but there were no significant differences between asthmatic and non-asthmatic participants in Rrs (%predicted) (p=0.081). In the supine position, FEV1 (%predicted) was lower (p=0.025) and Rrs was higher (p=0.012) in the asthmatic subjects. The dose of methacholine administered on the scanning day was higher in the non-asthmatics (p=0.003), but the changes in supine lung function were similar in asthmatics and non-asthmatics, measured by percentage decrease in FEV1 (p=0.511), percentage increase in Rrs (p=0.102) or absolute changes in Rrs (p=0.989). Lung volumes during scanning at baseline and post-methacholine were similar, since IC measured at the baseline and post-methacholine scans were similar (p=0.870).
Demographical and lung function data at baseline and after methacholine challenge
Table 2 shows the characteristics of airway measurements from the HRCT data. At baseline, radiological airway lumen were significantly narrower in asthmatics than in non-asthmatics (p<0.001). In non-asthmatic subjects, 28 parallel sister airway pairs could be identified and analysed from seven subjects, or approximately four airway pairs per subject, and in asthmatics 24 parallel sister airway pairs were identified and analysed from nine subjects, or approximately three airway pairs per subject. Heterogeneity of airway calibre measured as coefficient of variation of parallel sister airway lumen area was similar in asthmatic compared with non-asthmatic subjects (p=0.2) and did not predict heterogeneity of response to methacholine in either group. Baseline Aimean was smaller in asthmatics compared with non-asthmatics (p<0.001). After methacholine mean airway response, measured as percentage change in Aimean was not different between asthmatic and non-asthmatic subjects, but the absolute change in Aimean was greater in non-asthmatics (p<0.001).
Radiological airway characteristics
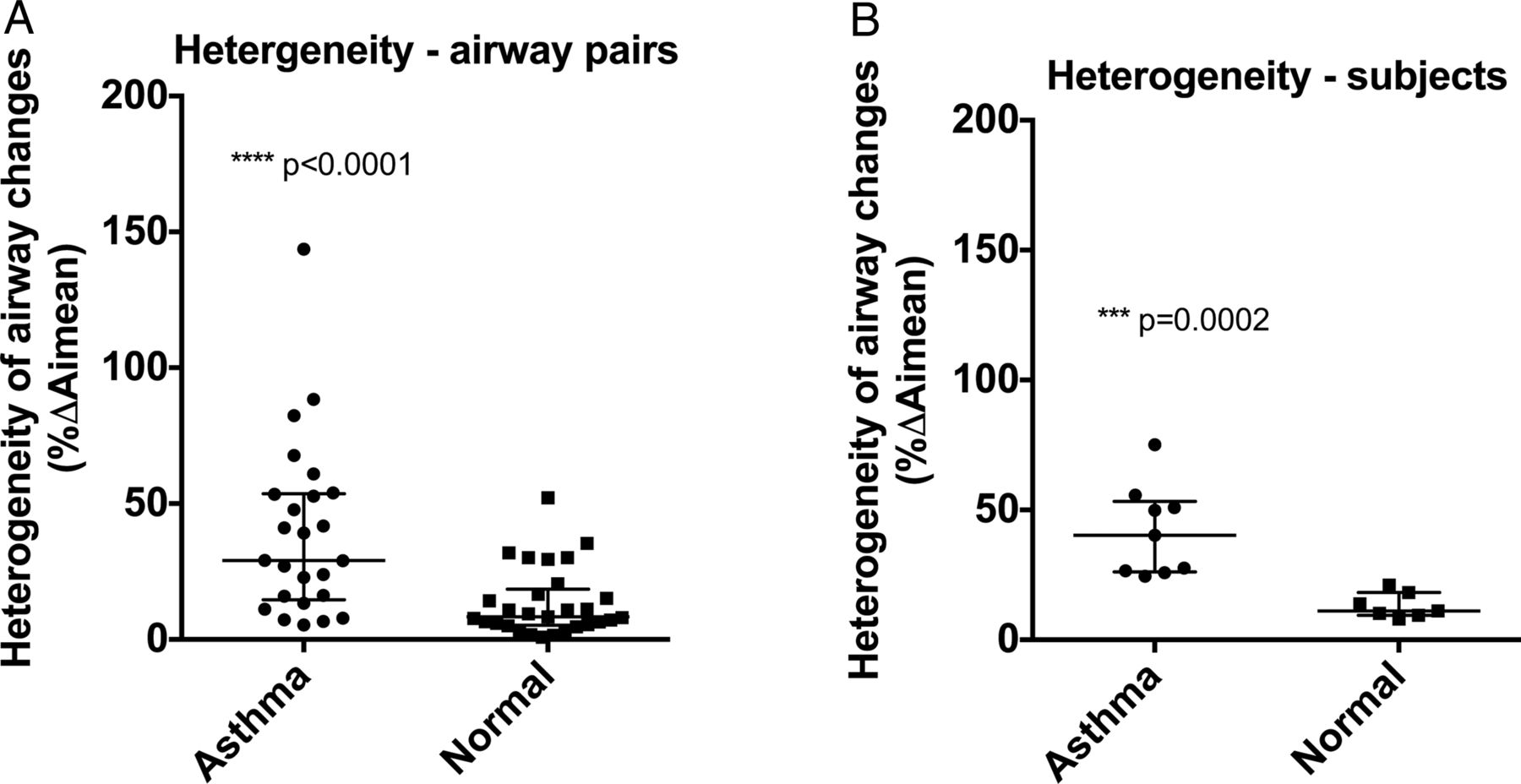
There were highly significant differences between asthmatic and non-asthmatic participants in heterogeneity of airway response (both narrowing and dilatation) between parallel sister airway pairs and airway closure induced by methacholine. Heterogeneity of parallel sister airway response to methacholine was greater in asthmatics, median (IQR) being 33% (27%–53%) compared with that of non-asthmatics of 11% (9%–18%) (p<0.001, figure 2). Radiological airway closure was also greater in asthmatics compared with non-asthmatics following methacholine challenge, with 24.1% of all airways measured appearing closed in the asthmatic group and 7.7% of all airways appearing closed in the non-asthmatic group (p=0.001 χ2, figure 3). An airway that appeared radiologically closed at baseline and which remained closed post-bronchoconstriction was assigned a ΔAimean of 0%. An airway that was open at baseline but closed following bronchoconstriction was assigned a ΔAimean of 100%. All airways that appeared radiologically closed at baseline remained closed following bronchoconstriction.

Heterogeneity of methacholine-induced changes in airway lumen area expressed for each pair of sister airways (A) and for each subject (B). Asthmatic airways had a more heterogeneous response than non-asthmatic airways overall.

Airway closure at baseline and following methacholine challenge in asthmatic (A and C) and non-asthmatic subjects (B and D). Two of the nine asthmatic subjects (A) and three of the seven non-asthmatic subjects (B) had no measured radiological closure at baseline or following methacholine. PostMCH, post-methacholine challenge.
The frequency distribution of airway narrowing and dilatation for asthmatic and non-asthmatic groups is shown in figure 4. There was a trend towards a broader range of airway narrowing and dilatation (p=0.067, χ2) in asthmatic airways. Analysis of the size-dependence of the response to methacholine in airways grouped by baseline airway size (figure 5) showed no size-dependent effects, in either asthmatic or non-asthmatic airways. Dilatation occurred in a similar proportion of asthmatic and non-asthmatic airways (14.6% and 12.1% (not significant), respectively, χ2), but there were greater extremes of dilatation in asthma. Airway dilatation was not correlated with airway size (r2=0.06 for both groups), and airways that dilated were not necessarily paired with airways that were closed or narrowed excessively.
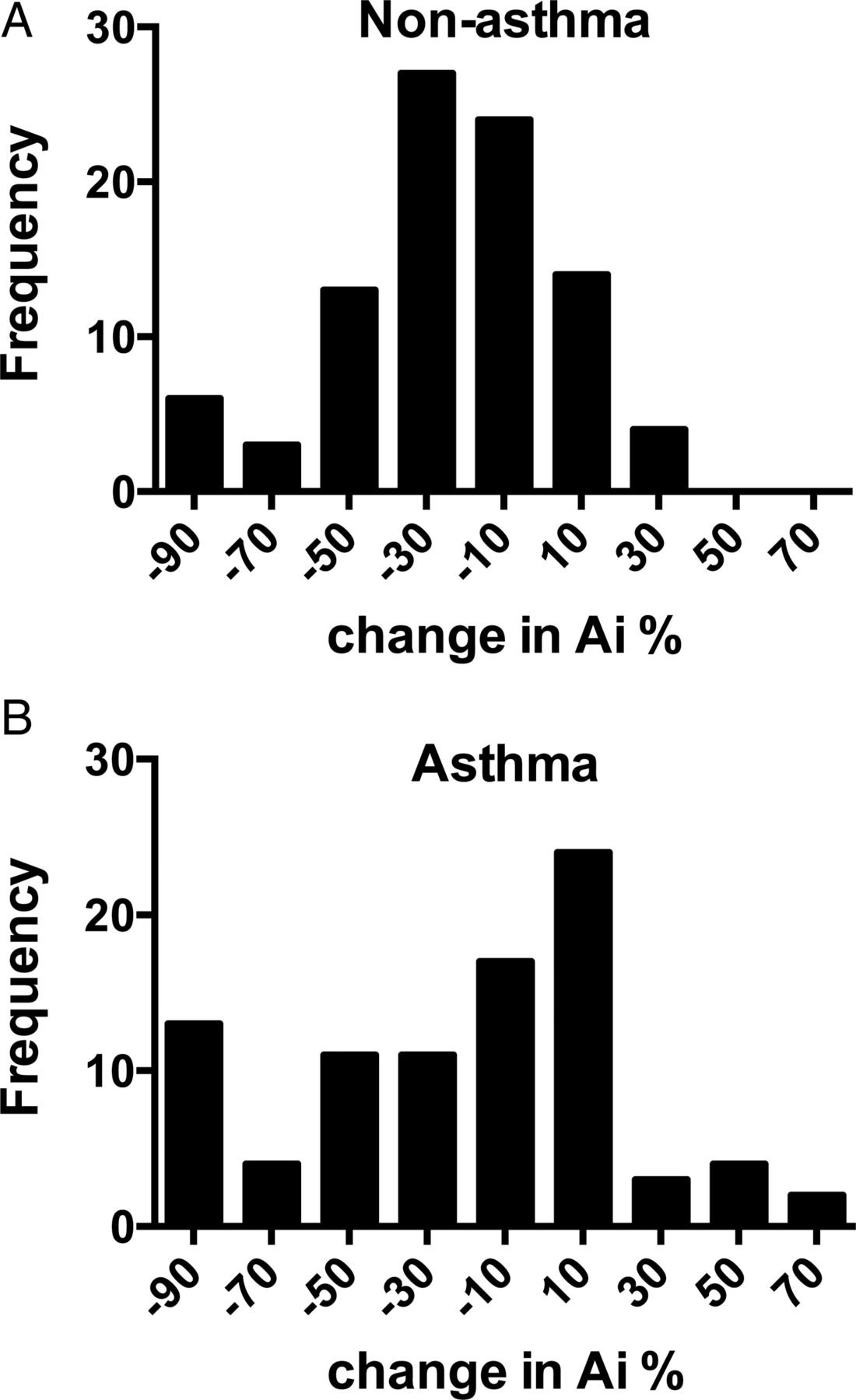
The frequency distribution of airway narrowing and dilatation for asthmatic and non-asthmatic groups is shown. There was a trend towards a broader range of airway narrowing and dilatation (p=0.067, χ2) in asthmatic airways.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Analysis of the size-dependence of the response to methacholine in airways grouped by baseline airway size showed no size-dependent effects, in either asthmatic or non-asthmatic airways. Data expressed as mean percentage change with 95% CI.
Discussion
In this study, we used a three-dimensional analysis of airways from HRCT images to measure the heterogeneous distribution of airway narrowing of parallel airways and the extent of airway closure in asthmatic compared with non-asthmatic subjects. We found that for similar methacholine-induced changes in FEV1 and resistance, the paired sister airways of asthmatic subjects responded with more heterogeneous radiological changes in airway diameter and had more radiological airway closure. Increased heterogeneity of airway narrowing was evident by comparing narrowing between parallel sister airways, as well as by the broader frequency distribution of airway narrowing and dilatation. The results of this study provide direct evidence of differences in behaviour between asthmatic and non-asthmatic airways at similar methacholine-induced changes in FEV1. Importantly, we have shown that these differences exist at the most basic level of airway organisation, that is, in parallel sister airways.
Our study has shown that the sizes of branching airway pairs of medium-sized and small-sized asthmatic airways become more uneven when bronchoconstricted, compared with the response of non-asthmatic airways. These results extend those of our previous study in which we measured heterogeneity of airway narrowing between airways that were more widely separated with the use of two-dimensional airway analyses.11 In the present study, we examined the airway tree starting at sub-segmental airways (approximately from generations 5 to 9). The difference in narrowing or dilatation of one airway compared with its closest neighbour is somewhat surprising, given their proximity and likely similar distending forces applied by the lung parenchyma. Although narrowing and closure could potentially occur in the proximal airways alone as measured in this study and would be consistent with the observed defects in ventilation imaging studies, it is likely that there is widespread distal airway heterogeneity of response as well.12
The functional and anatomical basis of this heterogeneous airway narrowing of sister airways is unknown. One proposed mechanism to explain how heterogeneity affects the lung is one of airway dependence, or that peripheral small airways are interconnected by the parenchymal tissue such that narrowing of one airway may increase the chances of narrowing the airway of its neighbours. This may result in an unstable state that proceeds until large clusters of airways close, rendering large regions of lungs unventilated, when a new stable equilibrium is reached.12 The origin of the ventilation defects would therefore be in the small airways. This may be the case, but these peripheral airways are too small to be measured in the current study. However, this is supported by modelling data only; there are no known experimental data to support this behaviour. An alternative explanation is one of airway independence, or that the differences in remodelling and airway mechanics between sister airways is sufficiently great that a sister airway closes when bronchoconstricted. That is, that the behaviour of any airway is determined purely by its own structural and mechanical properties so that an airway could behave entirely independently of any of its neighbours. Therefore the large ventilation defects that occur in asthma would require medium-to-small airway closure observed in the present study, rather than in more peripheral airways. In one study,26 the patterns of ventilation defects in the lungs and changes in oscillatory mechanics measured in asthmatics following bronchoconstriction could only be modelled by combining defects in both the peripheral and the larger more central airways, and only if heterogeneous narrowing is distributed throughout the entire airway tree. Our resistance measurements did not reflect the radiological measurements; this is to be expected, because they are measuring different regions of the lung.
In this study, we found that asthmatic airways were narrower at baseline and experienced greater baseline radiological closure of medium and small airways down to approximately 1 mm in diameter compared with non-asthmatic subjects. We normalised the change in lumen area for airway size, rather than use the absolute change, because of the wide range of airway lumen area at baseline. Had we not, the changes would have been dominated by the large airways, whereas normalisation by baseline character allowed us to measure the distribution of response to methacholine, across the wide range of airways sizes. Furthermore, more airways closed radiologically when bronchoconstricted in the asthmatic subjects. This was, to our knowledge, the first time airways have been noted to close in HRCT; however, the resolution of anisotropic voxels used in this HRCT study is such that airways that are severely narrowed may appear closed. This limitation could be overcome in future studies using near isotropic scanning. Nevertheless, even if there is severe airway narrowing rather than true closure, there is likely to be a very large difference in function between the two airways in terms of resistance, given that resistance is determined by radius to the fourth power. Asthmatic airways may be more likely to close because of their smaller baseline diameter combined with their greater range of airway narrowing (heterogeneity). That is, closure occurs because asthmatic airways are already narrower to start with and there are more airways that narrow severely in asthmatic subjects (seen by the wider frequency distribution in figure 4). Measurement of closure affected the current analysis of heterogeneity because closure equalled 100% change in airway lumen area, resulting in greater heterogeneity when the sister airway does not also narrow excessively. Airway closure is important in asthma because it is associated with worse AHR, more exacerbations and worse asthma control.1–3
We have previously explored the limitations of HRCT to measure airway dimensions.11 ,25 We found that the error in the HRCT measurement of airways is predictable and dependent on airway size. The assumption must be made that the effect of the error will be similar between asthmatics and non-asthmatics when comparing airways of similar size. To investigate whether the heterogeneity we observed was attributed to the inherent measurement error of HRCT in smaller airways, we compared heterogeneity (differences in % ΔAimean) between non-asthmatics and asthmatics in airways <3.2 mm in diameter, near the previously described limit of accurate measurement capability. We found that the difference in heterogeneity of sister airway response between non-asthmatics and asthmatics in these airways was highly significant (p<0.001). This confirmed that the heterogeneity measured in the current study was not attributable to the inherent measurement error of airways by HRCT. We also tried to minimise the errors associated with HRCT airway measurements by excluding the very smallest airways <1 mm in diameter. In a further effort to minimise the effects of volume averaging we included in analysis only airways that appeared to be oriented roughly perpendicular to the scanning plane.
The constraints of radiation exposure meant that we were limited in our sampling within the lungs. Our analysis was restricted to a 2 cm axial length of the lower lung region, within which we made measurements on airways that branched up to three times. Heterogeneity measured in our study may not be representative of heterogeneity in other regions of the lung, or indeed, of the whole lung. In addition, CT resolution only allowed sampling of medium and proximal small airways, so we could not determine whether this degree of parallel heterogeneity occurs in more distal airways. The function of more peripheral airways is also important because there are strong relationships between small airway function and AHR27 and asthma control.4 ,28 However, since remodelling of asthmatic airways occurs throughout the airway tree,29 it is likely that the increased heterogeneity that we measured in asthmatic subjects using HRCT would be reflected in the lung periphery, consistent with the increased ventilation heterogeneity observed in asthmatic participants.4 ,5
It is also likely that our measurements of ventilation heterogeneity were affected by supine posture in which it has been shown to be increased in normal subjects when measured by single breath washouts of inert gases.30 However, it is possible that supine posture differentially affected asthmatics compared with non-asthmatics, given that the pattern of airway closure differs with closure occurring in basal airways in non-asthmatics in contrast to being unpredictable in asthmatics.6 Unfortunately, it is presently not possible to perform HRCT scans on patients when upright to compare postures. Supine posture has been shown to affect the deposition of particles of a similar size to the size of the aerosolised methacholine generated by the DeVilbiss nebulisers used in the present study. There is a shift of the relative deposition from the alveolar to the bronchial airways, but supine posture does not have a significant effect on the deposition in the small, intermediate or large airways.31 So we believe that methacholine was deposited throughout the airway tree when administered in the supine position in this study and that it acted to constrict airways of all sizes.
In conclusion, we found asthmatic airways to be narrower at baseline and responded to inhaled methacholine by more heterogeneous narrowing of parallel airways and greater airway closure. This is the only data on heterogeneity based on measured differences in airway narrowing of sister airways in asthma. Previous studies, including our previous publication,11 looked at heterogeneity across airways that were unrelated anatomically. Our findings are also relevant if airway narrowing is affected by differences in parenchymal tethering; parallel airways are more likely to be affected by the same parenchymal forces than airways further apart. Our measurements can inform computational models of airway narrowing so that simulations reflect actual airway behaviour in vivo. If this abnormality is being repeated across the entire airway tree, it could have profound implications for understanding the nature of asthma. This could also have implications for the treatment of asthma inasmuch as the deposition of inhaled drugs is dependent on bulk flow of gas.32 ,33
Acknowledgments
The authors thank Dr Aneal Chandra, PhD, for his contributions towards the design and coding of the image analysis software.
References
Footnotes
Contributors JRDC was responsible for data acquisition, analysis and interpretation, drafting and final approval of the manuscript. JSM was responsible for data acquisition and final approval of the manuscript. NB was responsible for clinical/physiological interpretation and final approval of the manuscript. CMS was responsible for data interpretation, drafting and final approval of the manuscript. GGK, the principal investigator, was responsible for conception and design, data acquisition and analysis plan and interpretation, drafting and final revisions of manuscript and final approval as well as guarantor of integrity of the data as well as responsible for Good Clinical Practice.
Funding Funding for this research was provided by NHMRC project grant #153839, University of Sydney U2000 Postdoctoral Research Award and the Cooperative Research Centre for Asthma and Airways.
Competing interests None declared.
Ethics approval The Ethics Committee of the Royal Prince Alfred Hospital, Sydney.
Provenance and peer review Not commissioned; externally peer reviewed.