Article Text

Statistics from Altmetric.com
A patient with cirrhosis and hepatocellular carcinoma, on the waiting list for liver transplantation, presented with lung nodule during initial evaluation. A CT-guided core needle lung biopsy under general anaesthesia was performed. Pneumothorax (figure 1) and a large amount of gas within the left ventricle (figure 2) were identified during the procedure. Neurological focal signs (drowsiness, conjugate eye deviation and right hemiparesis) were observed in the anaesthesia-recovery period. A brain CT scan was immediately obtained, showing cerebral air embolism (figure 3). Initial resuscitation and hyperbaric oxygen therapy were performed. Five days later, MRI revealed a massive stroke (figure 4). At 3-month follow-up, the patient recovered motor functions, however, maintained with important cognitive deficits. Systemic air embolism is a rare but potentially life-threatening complication of percutaneous lung biopsy. The incidence ranges from 0.02% to 0.5%.1–3 Coughing during the procedure, cystic or cavitary lesion, positive pressure ventilation and needle-tip placement through a pulmonary vein are the most common predisposing factors. The management involves high-flow 100% oxygen and early hyperbaric oxygen therapy.

CT-guided lung biopsy of the nodule was performed with a 20-gauge needle and the patient in supine position. A small pneumothorax was already seen in this image.

The repeated CT image showed a large amount of gas within the left ventricle.

Axial CT of the brain showed gas locules within the left parietal lobe.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
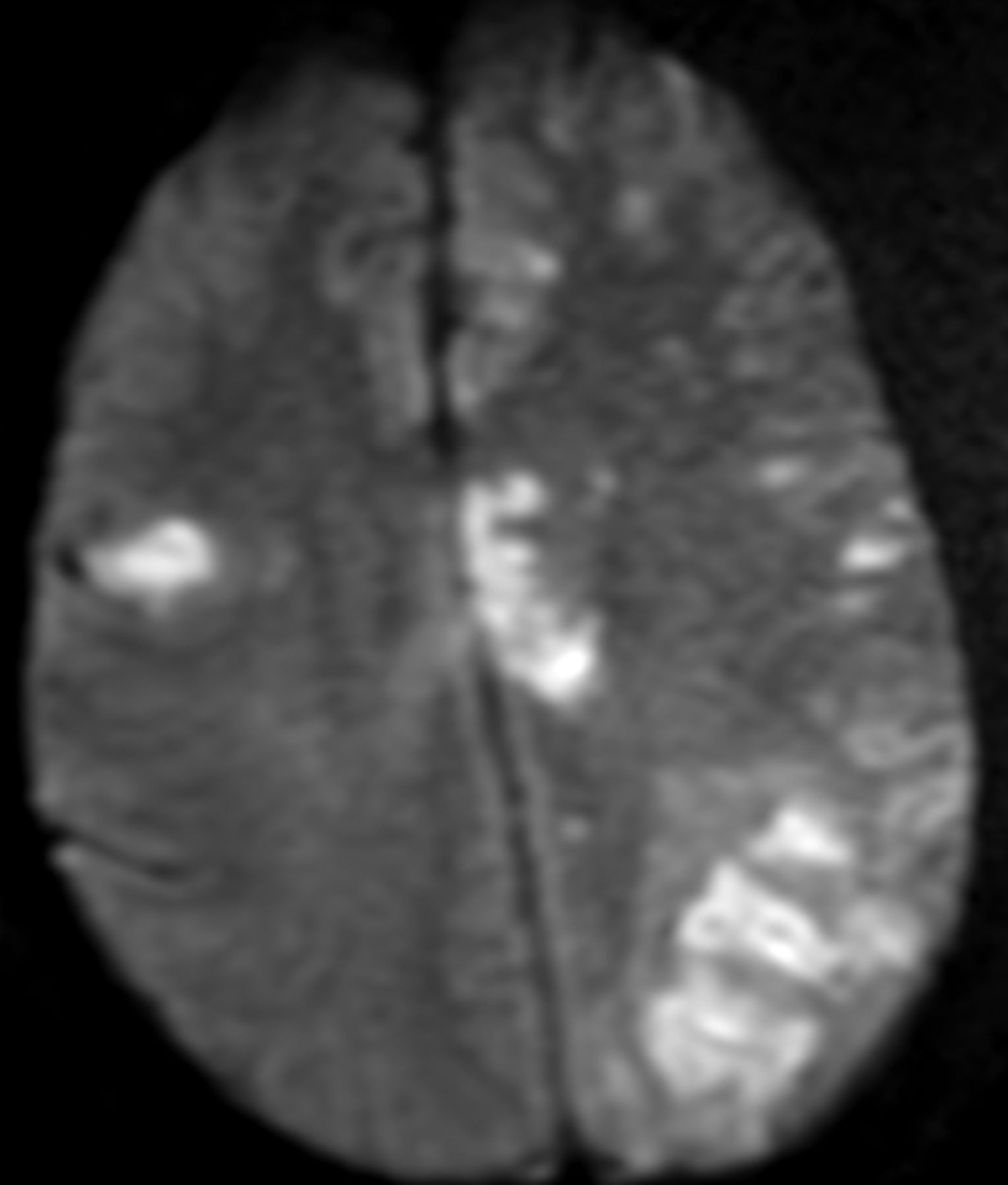
Magnetic resonance image after 5 days revealed the real extension of the embolism. A massive stroke involving both sides of the brain can be seen.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.