Article Text

Abstract
Rationale Chronic systemic infections such as those with Helicobacter pylori (H. pylori) may contribute to the evolution and progression of chronic obstructive pulmonary disease (COPD). Using data from the Lung Health Study (LHS), we determined the relationship of H. pylori infection with the severity and progression of COPD.
Methods Using an immunoassay, we measured H. pylori immunoglobulin G (IgG) antibody titres in serum samples of 4765 patients with mild-to-moderate COPD. We then determined their relationship with the individual's FEV1 and the rate of decline in FEV1 and mortality over 11 years using multiple regression analysis.
Results Approximately 18% of the patients were seropositive to H. pylori and these individuals demonstrated lower FEV1 (L) values at every study visit compared with individuals who were seronegative for H. pylori (p value=0.00012). However, patients with seropositivity to H. pylori were on average 0.012 m shorter than those with seronegativity (p value=0.0015). The significant relationship between FEV1 and H. pylori seropositivity disappeared when FEV1 per cent predicted (FEV1pp) was used (p value=0.45). H. pylori seropositive individuals had greater circulating C reactive protein (CRP) levels compared with H. pylori seronegative individuals (p value=0.012), and had increased risk of cardiovascular mortality (relative risk 1.61, p=0.05).
Conclusions H. pylori infection was associated with reduced lung function that is most likely due to the effect of the bacterium on lung growth earlier in life. It is also associated with systemic inflammation and increased risk of cardiovascular mortality in patients with COPD.
Trial registration numbers NCT00000568 and NCT00000569.
- COPD epidemiology
- Respiratory Infection
Statistics from Altmetric.com
Key messages
What is the key question?
Can Helicobacter pylori infection lead to reduced lung function and/or poor clinical outcomes in patients with mild-to-moderate COPD?
What is the bottom line?
Patients with H. pylori infection have lower FEV1 (L), are shorter on average, have higher circulating C reactive protein (CRP) levels and may be at increased risk of cardiovascular death compared with patients without H. pylori.
Why read on?
This is the largest study to date, with over 4000 patients, to investigate the possible role of H. pylori infection in the systemic inflammatory response and poor health outcomes in COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a major disease burden across the world, affecting 300–600 million individuals and killing 3 million annually.1 Although the pathogenesis of COPD has not been fully worked out, chronic inflammation is believed to be an important component. In addition to lung inflammation, some individuals with COPD demonstrate persistent systemic inflammation, which is associated with increased symptoms and poor health outcomes, including hospitalisation and mortality.2 A major source of persistent systemic inflammation is the gastrointestinal tract, which through the actions of the local bacterial microbiota modulates the body's immune response to viral infections.3 Consistent with this theory, a recent study has shown that manipulation of the gut microbiota with antimicrobials early in the lifespan of ‘asthmatic’ mice alters their disease phenotype.4
One important bacterial player in the gastrointestinal tract is Helicobacter pylori (H. pylori). Previous studies suggest that chronic infection with H. pylori is associated with persistent systemic inflammation and endothelial dysfunction, which are also found in patients with COPD.5 Moreover, large epidemiological studies have shown that patients with COPD have significantly increased risk of peptic ulcers compared with ‘healthy’ smokers.5
There have been prior studies that have investigated a potential role of H. pylori infection in COPD.6 ,7 However, these studies have produced discrepant findings probably owing to small sample sizes and selection bias. Using a large cohort of patients with mild-to-moderate COPD, we determined the relationship of H. pylori infection with clinically relevant endpoints in COPD such as lung function, lung function decline and mortality over time.
Methods
Sample population
We used data and samples from the Lung Health Study (LHS), which has been described in detail previously.2 In brief, LHS recruited smokers between the ages of 35 and 60 years who had Global initiative for chronic Obstructive Lung Disease (GOLD) 1 to GOLD 2 grades of COPD, defined by spirometry. Individuals who had other major diseases, such as cancer, were excluded. Once enrolled, patients were asked to visit the study centre annually for 5 years. At these visits, salivary cotinine levels and exhaled carbon monoxide levels were measured to validate the smoking status of the patients and to objectively verify if they had quit smoking. Detailed information on the study population can be found in previously published reports.2 ,8 This study analysed data on 4765 patients from this cohort.
Blood collection and ELISA measurements
At the 5-year follow-up visit, participants were asked for a blood sample. Blood samples from those who consented were separated into their respective components, transferred to the LHS main coordinating centre and stored in −70°C freezers. Serum samples were thawed, and H. pylori immunoglobulin G (IgG) concentrations were measured using a commercially available ELISA kit (DRG Diagnostics, GmbH, Marburg, Germany) according to the manufacturer's protocol. The lower limit of a positive H. pylori IgG titre, indicative of colonisation, was 18 DU/mL. Values lower than 18 DU/mL were treated as not having an active H. pylori colonisation of the stomach. C reactive protein (CRP) was measured using a commercially available ELISA kit (Alpha Diagnostic, San Antonio, Texas, USA). The results from the CRP measurement have previously been reported.2 The protocols for blood collection were approved by the University of British Columbia/Providence Health Care Research Ethics Committee.
Lung function measurements
Spirometry was performed at recruitment and annually for 5 years. One final measurement was then made approximately 11 years following initial recruitment. Owing to the smoking cessation intervention and the use of an active bronchodilating agent, certain patients experienced a significant increase in lung function in the first 2 years,9 after which, these individuals experienced a linear rate of FEV1 decline.10 For the present analysis, measurements taken after year 1 were considered baseline. For analysis on rapid decliners, a range of cut-off values (20 –160 mL/year) in 20 mL/year increments were used as thresholds, and those below the cut-off were categorised as steady decliners or non-decliners, and those above the cut-off were categorised as rapid decliners. We also determined total mortality and disease-specific mortality (lung cancer, congestive heart disease and cardiovascular disease) in this cohort as previously described.8
Statistical analysis
All statistical analyses were performed using R (V.3.1.2) and R Studio (V.0.98.1091). The study population was first divided into those who were H. pylori IgG seropositive and those who were seronegative. Analysis was performed either on FEV1 (L) or FEV1 per cent predicted (FEV1pp) from year 2 to year 11. For both analyses, a t test was used to determine significance of changes between those with and without positive antibodies to H. pylori at each time point. All of these p values were corrected for multiple comparisons using the Bonferroni method. We then performed a similar analysis among patients in GOLD grade 1 and 2, separately. We compared the prevalence of H. pylori IgG seropositivity between GOLD grade 1 and 2 using a χ2 test. Linear regression analysis was used to evaluate the relationship between serum H. pylori IgG levels and decline in FEV1 (L) or FEV1pp. Patient characteristics between the H. pylori positive and negative groups were compared using t tests for continuous variables and a χ2 test for dichotomous variables. χ2 testing was used to compare the H. pylori prevalence between rapid and steady decliners. For values that fell in the ‘grey’ zone of positivity (H. pylori IgG levels between 15 and 18 DU/mL), the samples were considered equivocal for infectivity (see online supplementary figure S1). Since the equivocal group mirrored the negative group, we combined these two groups for all analyses. There was no significant variation in data across the ELISA plates (see online supplementary figure S2). Multiple linear regression models were used to adjust for sex, smoking status, race, body mass index (BMI) and height. The risks of total mortality and disease-specific mortality between H. pylori seropositive and seronegative patients were compared using a χ2 test. The difference in CRP levels between H. pylori positive and negative patients was compared using a t test, following log-transformation of CRP values.
Results
H. pylori positive and negative patient characteristics
An overview of the patient characteristics can be found in online supplementary table S1, and these characteristics based on H. pylori seropositivity are summarised in table 1. There was no difference in sex, age at which smoking started, pack years, BMI, race or the number of sustained quitters between the H. pylori seropositive and seronegative groups (p value >0.05). However, there was a significant height difference between the H. pylori positive and negative groups (p value=0.0015). The H. pylori positive group was on average approximately 0.012 m shorter than the H. pylori negative group (table 1). The relative risk (RR) of mortality along with the 95% CI can be found in table 2. Individuals with H. pylori seropositivity had a borderline significant increase in the risk of cardiovascular deaths (RR=1.61, p value=0.05). However, there was no significant difference in total or lung-specific mortality between the two groups. Patients with H. pylori seropositivity demonstrated higher serum CRP levels (1.063±0.714 mg/L vs 0.995±0.689 mg/L in logarithmic scale, p value=0.012).
Patient characteristics of the Helicobacter pylori positive and negative groups
Relative risk (RR) breakdown based on Helicobacter pylori seropositivity
Overall lung function decline and H. pylori seropositivity
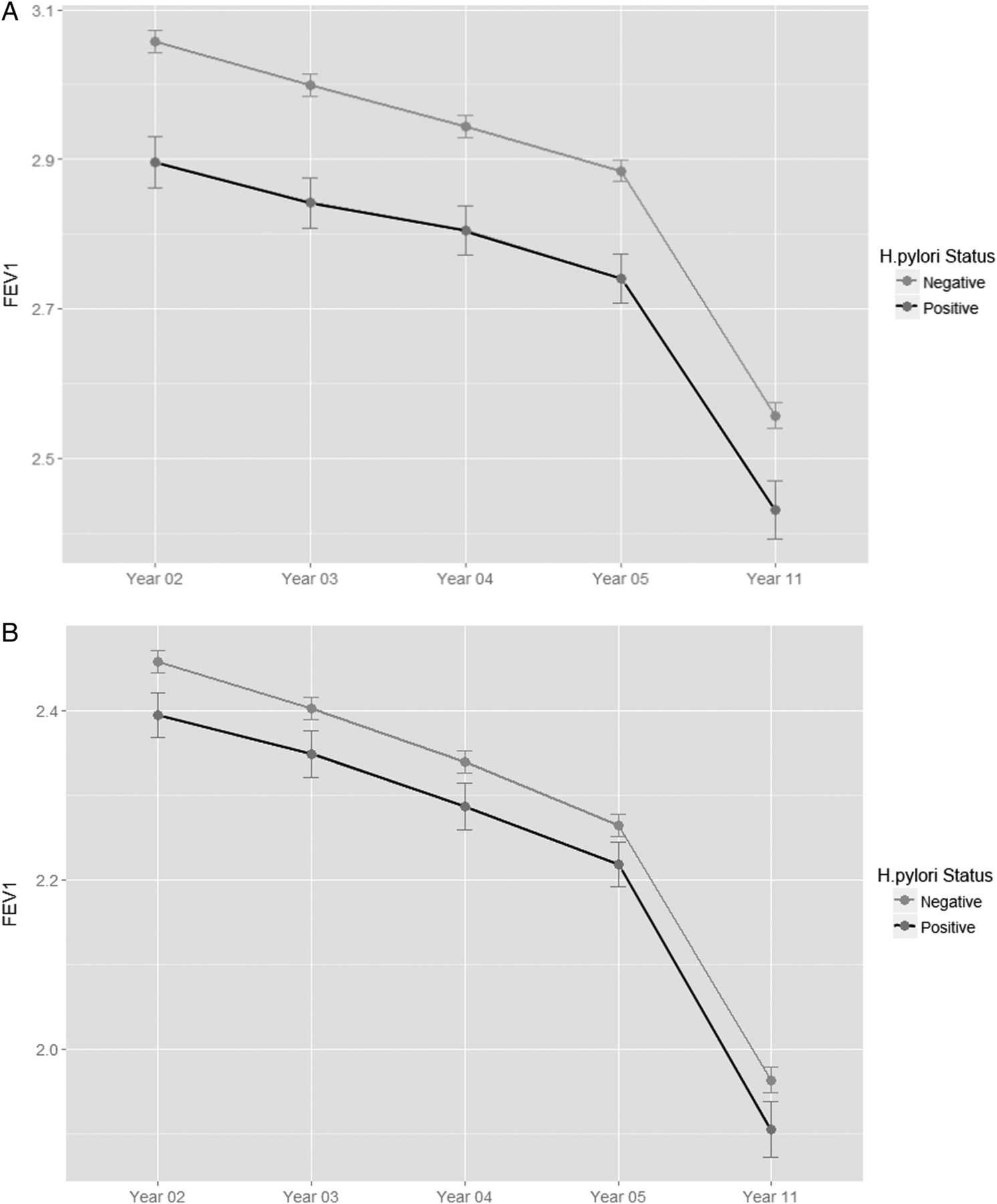
Patients who were H. pylori positive demonstrated reduced FEV1 (L) at baseline compared with those who were negative (p value=6.48×10−6) (figure 1A). Men and women with seropositivity to H. pylori had lower FEV1 (L) than their H. pylori negative counterparts except for men at year 11 (see online supplementary figures S3 and S4). However, there were no differences in the rate of decline (slope) between the two groups (p value=0.35). The baseline FEV1pp values, which corrected for age, race, sex and height, were not significantly different between the groups (p value=0.45) (see online supplementary figures S5 and S6). Similarly, the rate of decline was not significantly different between the two groups (p value=0.67) (figure 1B). Although there was a significant inverse relationship between serum H. pylori IgG concentrations (in a natural log scale) and FEV1 (L) (p value=2.9×10−7), this relationship disappeared when FEV1pp was used in lieu of FEV1 (L) (p value=0.68). There was no significant difference in the risk of H. pylori seropositivity between rapid and slow decliners (average p value=0.31), irrespective of the threshold value employed to define rapid decliners (data not shown).

(A) Mean FEV1 (L) over 11 years according to Helicobacter pylori status. There was no significant difference in the slope of the two lines (p>0.05). However, at every measured time point, those with H. pylori had significantly lower FEV1 after Bonferroni correction (p value <0.009). (B) Mean FEV1 per cent predicted (FEV1pp) over 11 years according to H. pylori status. There was no significant difference in both the slope and mean FEV1pp measured between the two groups (p>0.05).
H. pylori seropositivity and socioeconomic status of patients
To determine the potential influence of socioeconomic status (SES) on H. pylori seropositivity, we evaluated two variables related to SES of the LHS patients: maximal educational attainment11 and median income level at the time of study enrolment.12 Patients who were seropositive to H. pylori had on average 1 year of less schooling and approximately US$3000 less median income than those who were seronegative to H. pylori (table 1). There was also a significant difference in both median income and years of education between the H. pylori seropositive and seronegative groups (p<0.00001) (table 1). To determine the impact of these SES variables on the adult height of these study participants, we constructed a multivariable linear regression model in which the dependent variable was height (in metres), and the independent variables were age, sex, H. pylori serum concentration, median income and maximal years of education achieved (see online supplementary table S2). We found that the educational variable, but not median income, was strongly related to adult height. Interestingly, inclusion of educational attainment variable into the model made the H. pylori concentrations no longer significantly related to the adult height of the study participants. Together, these data suggest that years of education (a proxy for SES during childhood11) are strongly related to H. pylori status and are likely a part of the causal pathway in determining adult height.
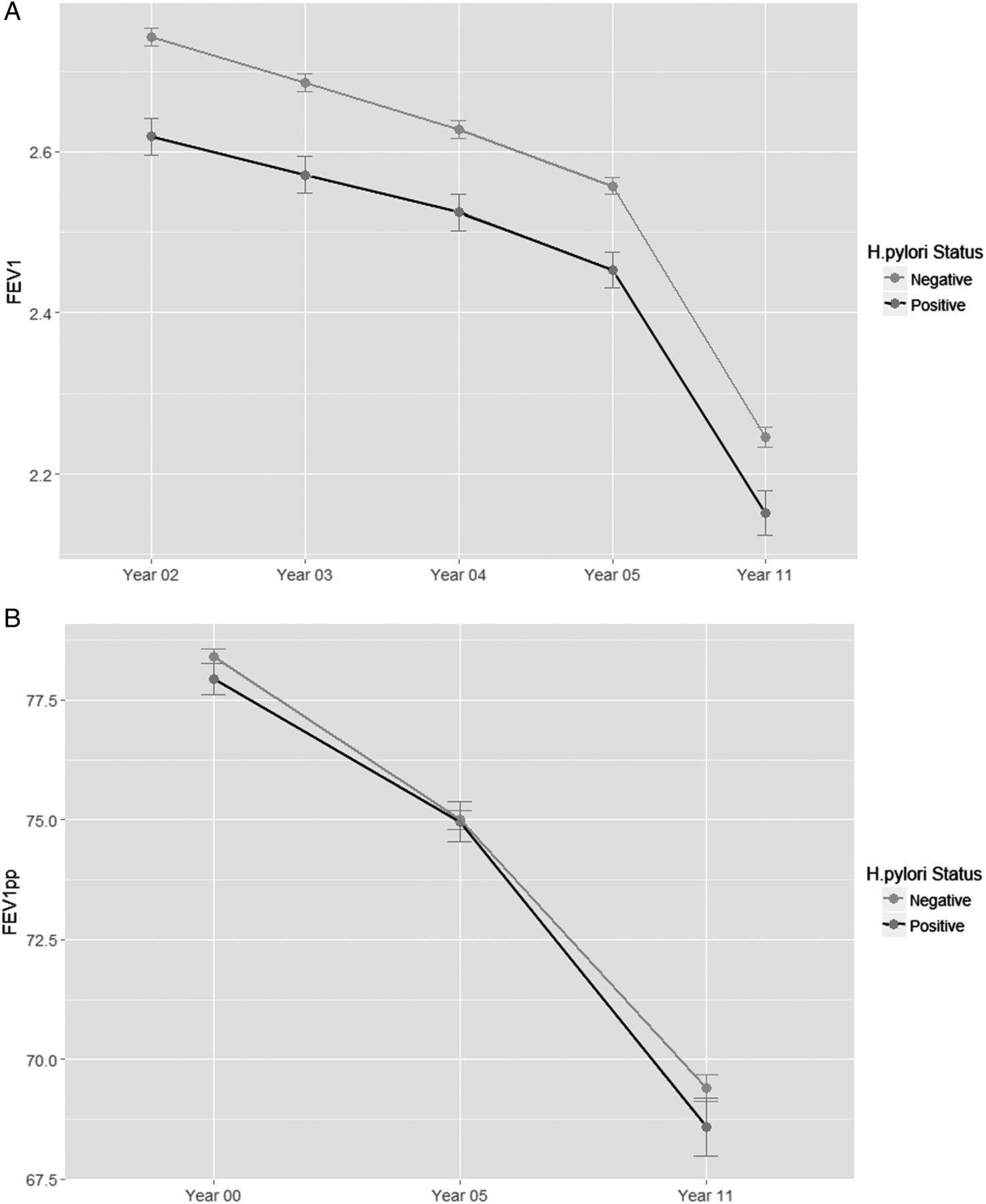
Mild GOLD grade and H. pylori seropositivity
There was no significant difference in H. pylori seropositivity between patients with GOLD 1 and GOLD 2 severity (17.5% and 17.7%, respectively). Patients with GOLD 1, who were H. pylori seropositive, demonstrated lower lung function at every visit compared with seronegative patients (average p value=0.011) (figure 2A). In contrast, for GOLD 2 grade, there was no significant difference in FEV1 between H. pylori seropositive and seronegative individuals (average p value= 0.42) (figure 2B). There was no difference in H. pylori IgG antibody concentration between GOLD 1 and GOLD 2 grade of disease (38.1±111.0 and 38.3±102.2 DU/mL, respectively). There was a significant difference in height between the GOLD 1 H. pylori positive and negative groups (p=0.0029, 1.714±0.09 m and 1.729±0.089 m, respectively). No significant difference in height was found in the GOLD 2 group based on H. pylori seropositivity (p=0.0742, H. pylori positive=1.707±0.084 m, H. pylori negative=1.715±0.089 m).

(A) Linear regression of the natural log of measured Helicobacter pylori immunoglobulin G (IgG) antibodies versus FEV1 (L). A significant negative correlation was found (R2=0.0054, slope=−0.18, p value=2.9×10−7). (B) Linear regression of the natural log of measured H. pylori IgG antibodies versus FEV1 per cent predicted (FEV1pp). No relationship was found between these two variables (R2=0.0002, slope=−0.0009, p value=0.68).
Discussion
The present study is the largest of its kind to evaluate the possible impact of H. pylori infection in patients with COPD. In this cohort, we found that H. pylori infection is relatively common in patients with COPD (approximately 18%) and is associated with systemic inflammation. Importantly, although H. pylori infection does not modify rate of decline in FEV1 over time or respiratory-specific mortality, it increases the risk of cardiovascular deaths, which is the major source of mortality in patients with mild-to-moderate COPD.
Interestingly, we also found that H. pylori infection was associated with reduced adult height. Height has long been known to be a major predictor of absolute lung volume.13 Because of this, FEV1 is height dependent.14 In the present study, the mean difference in height between the seropositive and seronegative individuals was 0.012 m. Our data are in keeping with a large body of literature demonstrating that chronic infection with this bacterium impairs growth during childhood, which manifests as shorter adult height.15 ,16 One study found that the average difference in height between H. pylori positive and negative individuals was 0.035 m.16 Interestingly, another study found that the growth rate in children could be restored on eradication of H. pylori infection with antibiotics.17 The mechanism by which H. pylori stunts the growth velocity in children is not fully known, and is an active area of investigation. We postulate that chronic infection with H. pylori in childhood may have caused impaired growth in lungs, leading to increased risk of COPD in adulthood. However, persistence of infection in adulthood probably does not accelerate progression of COPD. These findings add support to the hypothesis that early-life exposures can have a critical role to play in lung development and overall lung function.18 This hypothesis will need to be tested in a longitudinal cohort with robust follow-up.
Our data support the hypothesis that H. pylori could contribute to systemic inflammation in COPD19 by showing that CRP was elevated in the seropositive group (table 1). Additionally, previous studies have shown that those with H. pylori seropositivity are at an increased risk of myocardial infarction or coronary heart disease.19 ,20 Consistent with these prior observations, we found that those with H. pylori seropositivity had an increased risk of cardiovascular death, albeit at a borderline statistical significance (table 2). However, there were no significant differences in total or respiratory-specific mortality between H. pylori seropositive and H. pylori seronegative patients (table 2). Together, our data support the notion that H. pylori seropositivity is associated with systemic inflammation, and this in turn could lead to increased risk of cardiovascular events in patients with mild-to-moderate COPD.
Although there was no difference in the overall distribution of H. pylori seropositivity between individuals in GOLD 1 and 2 grades, there was a difference in FEV1 (L) at all time points between seropositive and seronegative patients in GOLD 1, but not in GOLD 2 (figure 3). The reason for this observation is not entirely clear. However, there was a significant difference in height in the GOLD 1 group between H. pylori seropositive and seronegative individuals that was not observed in the GOLD 2 group. Additionally, it is notable that the slope of FEV1 decline decreased from GOLD 1 to GOLD 2,21 which may have obscured the small influence of H. pylori on the rate of decline (figure 3B).
{kind=link}
{kind=link}
{kind=link}
(A) Mean FEV1 (L) over 11 years in GOLD 1 for Helicobacter pylori positive and negative groups. No difference in slope was observed (p>0.05); however, at every year, except year 11, the mean FEV1 (L) was lower in the H. pylori positive group versus the negative group (p<0.005). (B) Mean FEV1 (L) over 11 years in GOLD 2 for H. pylori positive and negative groups. No difference was observed between slope and mean FEV1 between the two groups (p>0.05).
There were limitations to the study. First, owing to the high percentage of Caucasians in the study population, the findings of the present study may not be generalisable to other racial groups. Second, we did not have sufficient ability to fully assess the SES of individuals in this study. Previous studies have shown that H. pylori may be linked to SES,22 ,23 and in turn, this could affect adult height. In the present study, we used years of education achieved as a surrogate for childhood SES11 and median income at study enrolment as a surrogate for adult SES.12 These are imperfect measurements of SES. Nevertheless, even using these imprecise SES measurements, we found a strong relationship of these variables with H. pylori status. Most importantly, we found that years of education achieved, but not median income, were significantly related to adult height, and the inclusion of the former variable into a multivariable model made the relationship between H. pylori status and adult height no longer significant. Collectively, these data are consistent with the notion that childhood SES is an important determinant of adult height and that H. pylori status may be in this causal pathway. Further work will be needed to validate this hypothesis. Third, this population was composed of patients with mild and moderate COPD, and it is possible that H. pylori may have a greater role in more severe disease. Fourth, LHS was conducted prior to the widespread availability of antimicrobial treatment for H. pylori, and as such, we could not determine the effects of eradication on lung function decline over time. However, our findings raise the tantalising possibility that early eradication (in childhood) may enable full development of lungs and reduce the risk of COPD later on in life. Fifth, because we do not have serial blood samples, we cannot be certain when patients were first infected with the bacterium. However, prior epidemiological data suggest that most infections occur during the first 5 years of life.24 Thus, seropositivity likely represents childhood infections. Sixth, past antibiotic use could have biased findings towards the null value. It has been well documented that antibiotic treatment to eradicate H. pylori can reduce H. pylori IgG levels.25–27 However, even targeted treatment with triple therapy, depending on country, can have a range of successful eradication rates (20%–80%).28 Furthermore, only specific antibiotics can be used to eradicate H. pylori due to the acidity of the environment in which it lives.28 Because LHS was conducted before the widespread use of triple therapy for H. pylori eradication, we believe that prior antibiotic use probably did not have a major impact on the findings. We also could not determine whether the presence of H. pylori represented active infection or colonisation. However, H. pylori is considered a pathogen and not a normal commensal in the gastrointestinal tract, and 75% of completely asymptomatic individuals harbouring H. pylori can demonstrate active gastritis on biopsy.29 Finally, in the present study, we did not evaluate the relationship of specific strains of H. pylori with clinical outcomes in COPD (eg, CagA). The relationship of specific strains of H. pylori with adverse health outcomes outside of the gastrointestinal tract is complex and controversial, with some studies showing a significant relationship with poor health outcomes30 ,31 while others showing a null or even a beneficial association.32–34 It was beyond the purview of this study to interrogate this complex interaction between specific strains of H. pylori and clinical outcomes in COPD.
Notwithstanding these limitations, the present study resolves the ongoing controversy of the possible role of persistent H. pylori infection in the progression of COPD. Our data suggest that H. pylori infection in adulthood does not impact on rate of decline in FEV1. However, it may play a significant role in adult height, which may result in lower FEV1 (L) in adulthood, predisposing certain individuals to COPD later on in life. Our data support the hypothesis that early-life exposures can play a big role in lung function, and that at this early stage in life, environmental exposures can drastically impact later health. Further, our findings suggest that H. pylori infection may contribute to persistent systemic inflammation in some patients with COPD and to their increased risk of cardiovascular mortality.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors MAS: designed experiments, data analysis, wrote first draft. Y-WRC: performed ELISAs for H. pylori. ST: assisted with assays. DT, RAW, JEC and SFPM: participated in interpretation of data, procurement of samples and data. DDS: participated in the design and execution of the experiments. All contributed to the write-up of the manuscript and approved the final paper.
Funding The study was funded by the Canadian Respiratory Research Network (CRRN), which was funded by the Canadian Institutes of Health Research (Institute of Circulatory and Respiratory Health Emerging Network); the Canadian Lung Association, the Canadian Thoracic Society and the Canadian Respiratory Health Professionals; the British Columbia Lung Association; with industry partner funding from AstraZeneca, Boehringer-Ingelheim (Canada), GlaxoSmithKline and Novartis Pharmaceuticals Canada.
Competing interests None declared.
Ethics approval UBC/PHCRI Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data are available from DDS.