Article Text

Abstract
Background Concerns about increased mortality could question the role of COPD chronic disease management (CDM) programmes. We aimed at extending a recent Cochrane review to assess the effects of CDM on mortality in patients with COPD.
Methods Mortality data were available for 25 out of 29 trials identified in a COPD integrated care systematic review. Meta-analysis using random-effects models was performed, followed by subgroup analyses according to study length (3–12 months vs >12 months), main intervention component (exercise, self-management, structured follow-up) and use of an action plan.
Results The meta-analysis showed no impact of CDM on mortality (pooled OR: 1.00, 95% CI 0.79 to 1.28).
Conclusions These results do not suggest that CDM programmes expose patients with COPD to excessive mortality risk.
- COPD epidemiology
Statistics from Altmetric.com
For more than two decades, chronic disease management (CDM) initiatives have been developed and implemented in many countries. CDM aims at reorganising healthcare systems and medical treatment to address the increasing burden of chronic diseases and provide solutions to organisational, medical and economical problems. A recent Cochrane systematic review showed that in patients with COPD, CDM significantly improved health-related quality of life as well as exercise tolerance (6-min walking test; 6MWT) and decreased the risk of hospitalisation.1 While updating non-Cochrane systematic reviews published in the mid-2000s and conducting a methodologically sound and rigorous Cochrane systematic review, Kruis et al confirmed previous trends in outcomes, indeed. Unfortunately, analyses of secondary outcomes, such as mortality, were not performed comprehensively enough from our perspective. In fact, out of 26 studies included in the review and 3 studies awaiting assessment,2–4 only data from the five randomised controlled trials (RCTs) explicitly reporting mortality as an outcome were considered in the mortality meta-analysis. Mortality results are of crucial importance for those interested in CDM development and implementation in the field, particularly since Fan's publication in 2012.3 In the latter study in fact, health benefits from such a programme were counterbalanced by an unexpected and still unexplained significantly higher mortality in patients with COPD participating in a comprehensive care programme.
The aim of our targeted analyses was to assess mortality of patients with COPD participating in CDM programmes using data from studies included in Kruis’ recent Cochrane review.1 Because all-cause mortality is an indisputable outcome, even if not a targeted study event, we considered all 29 RCTs described in Kruis’ review: 26 RCTs meeting Kruis’ operational definition of CDM (≥2 different types of healthcare professionals actively involved in patients care, ≥2 intervention components, ≥3 months’ duration) and included in the analyses, as well as three studies identified as ‘awaiting assessment’.1 We reviewed the three latter studies and considered them to meet inclusion and exclusion criteria of the systematic review; one of the three was the Fan's RCT.3 Mortality data were available for 25 of the 29 eligible studies described in Kruis’ review. Baseline number of patients included in both CDM and control groups, number of deaths in each group during studies’ periods as well as studies’ length, main intervention component and use of action plan, were extracted. We conducted a random-effects meta-analysis, followed by subgroup analyses according to study length (3–12 months vs >12 months), main intervention component (exercise, self-management, structured follow-up) and specific use of an action plan in the intervention.
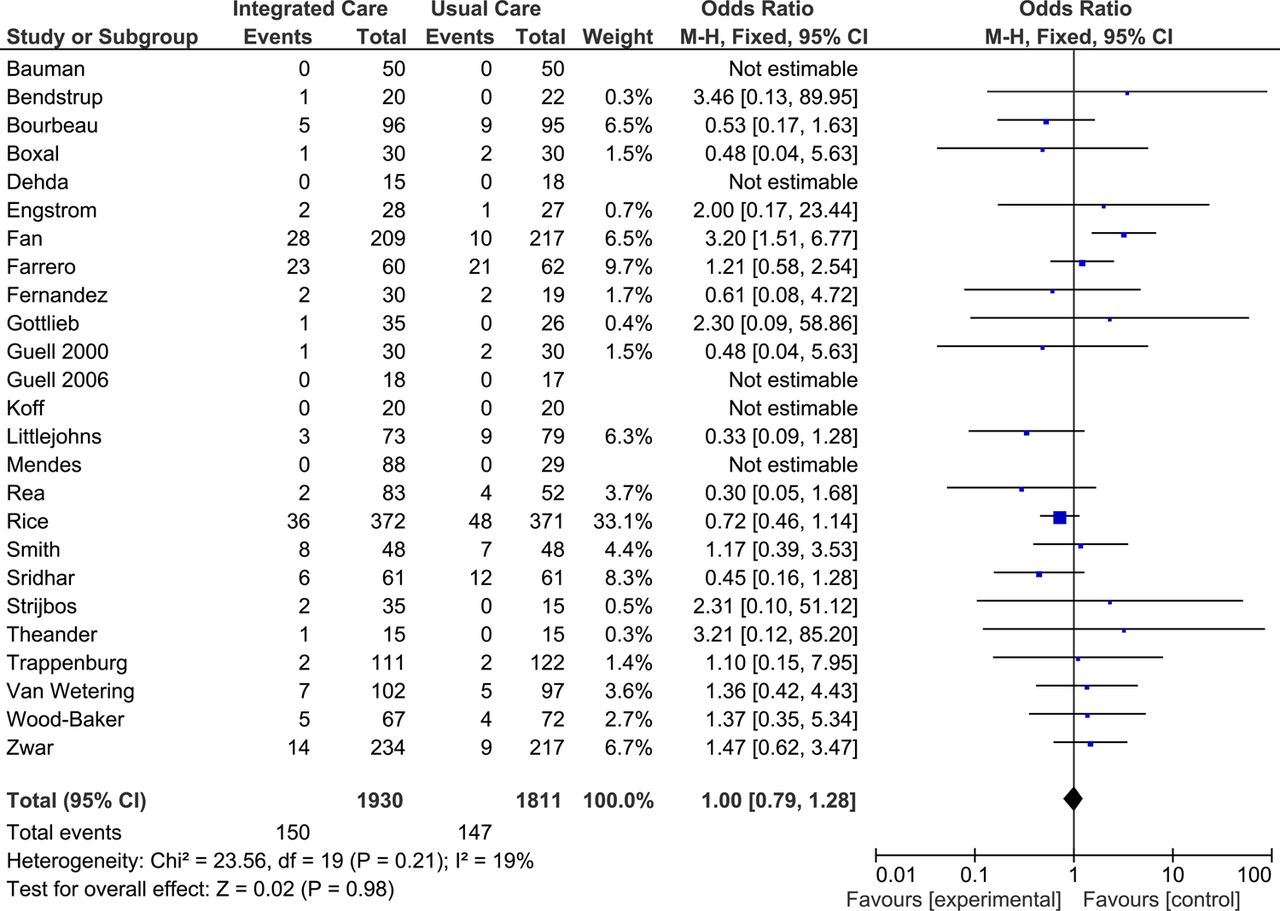
Our enriched meta-analysis showed no impact of CDM on overall mortality (25 studies; pooled OR: 1.00, 95% CI 0.79 to 1.28; figure 1). There was little evidence for heterogeneity (I2 19%) and only discrete asymmetry as assessed by a funnel plot. All subgroup analyses showed non-significant pooled ORs. As event rates were low, we also computed the unweighted estimate of the pooled OR after adding 0.5 to observed frequencies of all studies, as suggested by Bhaumil et al.5 This methodology allows the inclusion of zero total events and has been shown to perform better than the traditional DerSimonian and Laird approach in those situations. Results were however similar to the standard ones (pooled OR=1.07 95% CI 0.58 to 1.84, between-study variance τ2=0.4). Varying the between-study variance (0.08≤τ2≤0.6) did not alter the results, thereby illustrating their robustness.
{kind=link}
Overall mortality forest plot.
Results of this enriched meta-analysis do not suggest that complex interventions such as CDM expose patients with COPD to excessive mortality risk, as feared by a recent RCT.3
Footnotes
-
Contributors IP-B was at the origin of the project, extracted data, conducted analysis and wrote the manuscript. PT performed statistical analysis and participated in the writing of the manuscript. POB and MAP participated in the elaboration of the project, extracted data and participated in the writing of the manuscript. BB participated in the elaboration of the project and provided insightful comments to the manuscript. All authors read and approved the final version of the manuscript.
-
Competing interests IP-B is supported by a grant from the Swiss National Science Foundation (PROSPER no. 32333B-123817 and no. 32333B-139789) and by the Swiss School of Public Health+ (Assistant Professorship grant).
-
Provenance and peer review Not commissioned; externally peer reviewed.