Article Text

Abstract
Background Human bone marrow-derived mesenchymal stem (stromal) cells (hMSCs) improve survival in mouse models of acute respiratory distress syndrome (ARDS) and reduce pulmonary oedema in a perfused human lung preparation injured with Escherichia coli bacteria. We hypothesised that clinical grade hMSCs would reduce the severity of acute lung injury (ALI) and would be safe in a sheep model of ARDS.
Methods Adult sheep (30–40 kg) were surgically prepared. After 5 days of recovery, ALI was induced with cotton smoke insufflation, followed by instillation of live Pseudomonas aeruginosa (2.5×1011 CFU) into both lungs under isoflurane anaesthesia. Following the injury, sheep were ventilated, resuscitated with lactated Ringer's solution and studied for 24 h. The sheep were randomly allocated to receive one of the following treatments intravenously over 1 h in one of the following groups: (1) control, PlasmaLyte A, n=8; (2) lower dose hMSCs, 5×106 hMSCs/kg, n=7; and (3) higher-dose hMSCs, 10×106 hMSCs/kg, n=4.
Results By 24 h, the PaO2/FiO2 ratio was significantly improved in both hMSC treatment groups compared with the control group (control group: PaO2/FiO2 of 97±15 mm Hg; lower dose: 288±55 mm Hg (p=0.003); higher dose: 327±2 mm Hg (p=0.003)). The median lung water content was lower in the higher-dose hMSC-treated group compared with the control group (higher dose: 5.0 g wet/g dry [IQR 4.9–5.8] vs control: 6.7 g wet/g dry [IQR 6.4–7.5] (p=0.01)). The hMSCs had no adverse effects.
Conclusions Human MSCs were well tolerated and improved oxygenation and decreased pulmonary oedema in a sheep model of severe ARDS.
Trail registration number: NCT01775774 for Phase 1. NCT02097641 for Phase 2.
- ARDS
Statistics from Altmetric.com
Key messages
What is the key question?
-
Will intravenous delivery of bone marrow-derived human mesenchymal stem (stromal) cells reduce the severity of lung injury in a clinically relevant 24 h sheep model of severe pneumonia-related acute respiratory distress syndrome (ARDS)?
What is the bottom line?
-
Treatment with human mesenchymal stem (stromal) cells reduced the severity of inhalational and bacterial inoculation induced lung injury as measured by improved oxygenation and decrease of extravascular lung water without adverse effects on haemodynamics.
Why read on?
-
Because this preclinical study provides additional data to support the potential value of testing human bone marrow-derived mesenchymal stem (stromal) cells in patients with moderate to severe ARDS.
Introduction
The acute respiratory distress syndrome (ARDS) is a common cause of acute respiratory failure and is often caused by pneumonia and/or sepsis.1–3 ARDS is characterised by severe pulmonary oedema, leading to arterial hypoxaemia (PaO2/FiO2<300 mm Hg).4 Advances have been made in understanding the pathophysiology of ARDS, but therapies remain limited. Supportive care with lung protective ventilation,5 prone ventilation6 and a conservative fluid management strategy7 have improved clinical outcomes, but no specific therapy has improved survival. Thus, new treatments are needed.
In this regard, cell-based therapies may be promising for treatment of patients with ARDS. Bone marrow-derived mesenchymal stem (stromal) cells (MSCs) have shown therapeutic value in preclinical studies of myocardial infarction,8 diabetes,9 sepsis,10 hepatic failure,11 acute renal failure12 and acute lung injury (ALI).13 Work from our laboratory demonstrated that intravenously administered clinical grade, allogeneic human bone marrow-derived mesenchymal stem cells (hMSCs) restored alveolar fluid clearance to a normal level and decreased inflammation in an ex vivo isolated human lung preparation injured with live bacteria.14 We also reported that intravenous hMSCs increased survival in a rodent model of gram-negative peritoneal sepsis15 and in a mouse model of pneumonia.16
In the present study, we hypothesised that clinical grade hMSCs would reduce the severity of lung injury and would be well tolerated in a sheep model of ARDS induced by cotton smoke inhalation and instillation of live Pseudomonas aeruginosa into both lungs.
Materials and methods
This study was approved by the Institutional Animal Care and Use Committee of the University of Texas Medical Branch and conducted in compliance with the guidelines of the National Institute of Health and the American Physiological Society for the care and use of laboratory animals.
Surgical procedures
Adult sheep were surgically prepared 5–7 days before the experiment. The surgical protocol has been described in previous studies.17 ,18 Briefly, under isoflurane anaesthesia (Aestiva/5, Compact 7100, Tec 7 vaporizer, Datex Ohmeda, Madison, Wisconsin, USA) administered via endotracheal tube, the right femoral artery was cannulated for arterial access (Intracath, 16GA, 24IN, Becton Dickinson, Sandy, Utah, USA) and a thermodilution catheter (Swan Ganz, model 131F7, Baxter, Edwards Division, Irvine, California, USA) was introduced through the right common jugular vein into the pulmonary artery. A catheter (Duralastic Silicone Tubing DT08, 0.062 in. ID, Allied Biomedical, Paso Robles, California, USA) was also positioned in the left atrium through the fifth intercostal space. To determine pulmonary transvascular fluid flux (lung lymph flow), a thoracotomy in the sixth intercostal space was performed and the efferent vessel of the caudal mediastinal lymph node was cannulated with Silastic medical grade tubing (0.025 in. ID, Dow Corning, Midland, Michigan, USA). Following the operative procedures, sheep were awakened and the catheters were connected to monitors through pressure transducers. During the 5-day recovery period, the condition of the sheep was checked three times daily to ensure good recovery as demonstrated by lack of fever, appropriate eating and drinking, and good physical appearance.
Experimental protocol
After 5 days of recovery, baseline values were obtained and a tracheostomy was done under ketamine/isoflurane anaesthesia. Smoke inhalation injury was produced by insufflation of cotton smoke as previously described.19 ,20 Four sets of 12 breaths of smoke were delivered. Following the inhalation injury, P. aeruginosa (American Type Culture Collection) was instilled through a bronchoscope (Model PF-P40, Olympus America Inc., Melville, NY). The P. aeruginosa (strain 12-4-4) had been cultured overnight and centrifuged at 2000 rpm for 15 min. The bacteria were mixed with saline and their numbers adjusted to ∼2.5×1011 CFU in 30 mL solution. Aliquots (10 mL) of the bacterial mixture were instilled into the right middle, right lower and left lower lobes (30 mL total).19 ,20 After the injury, the sheep were ventilated (Servo Ventilator 300C, Siemens-Elema, Sweden) with positive end-expiratory pressure (PEEP) of 5 cm H2O and a tidal volume of 15 mL/kg throughout the 24 h experimental period. The inspiratory concentration of O2 was maintained at 100% for the first 3 h following injury and adjusted thereafter according to blood gas analysis. The respiratory rate was initially set at 20/min, and it was adjusted according to arterial CO2 concentration. All sheep received maintenance intravenous fluid during the study period, initially with lactated Ringer's solution at 4 mL/kg/h, after which the infusion rate was adjusted to maintain the haematocrit close to baseline levels (± 3%).
Control and hMSC-treated groups
Two or three sheep were injured at one time and then studied simultaneously. After injury, each sheep was randomly allocated to one of three groups1: control (treated with PlasmaLyte A only, n=8)2; lower dose hMSCs (treated with 5×106/kg hMSCs, n=7); and3 higher dose hMSCs (treated with 10×106/kg hMSCs, n=4). Each experimental group always included one control sheep. Clinical grade hMSCs were obtained from the NHLBI Production Assistance for Cellular Therapies at the University of Minnesota. Prior to administration, the cryopreserved hMSCs were thawed in a water bath, washed with PlasmaLyte A and centrifuged to remove the DMSO and cell debris in the supernatant. They were then resuspended in PlasmaLyte A and counted prior to infusion. The cells were administered intravenously over 1 h via central line, starting 1 h after injury.
Measurements
Several cardiopulmonary variables were measured continuously, including pulmonary arterial, central venous, systemic arterial and left atrial pressures. Cardiac output was measured by thermodilution technique using a cardiac output computer (COM-1TM, Baxter, Edward Division). Peak airway and pause airway pressures (similar to plateau airway pressure in patients ventilated with volume control ventilation) were measured hourly. Arterial blood gases were analysed at multiple time points (GEM Premier 3000, Instrumental Laboratory, Lexington, Massachusetts, USA). Lymph flow and lymph and plasma protein concentrations were measured hourly from hours 1 through 6, and every third hour thereafter. It was assumed that lymph flow remained constant during the 3 h intervals. The pulmonary transvascular fluid flux was evaluated every 3 h based on the lung lymph flow measurements.17 ,18 Systemic vascular resistance index (SVRI) was calculated using standard equations. Urine output was measured every 3 h.
Chemistry measurements
Serum BUN, creatinine, ALT, AST, lactate and glucose were measured at baseline, 12 and 24 h.
Prespecified criteria for euthanasia
Systolic blood pressure <50 mm Hg, heart rate <40 beats per minute over 1 h, arterial PaO2 <50 mm Hg at FiO2=1.0 over 1 h or an arterial PaCO2>90 mm Hg were prespecified as criteria for euthanasia. Sheep that did not require euthanasia prior to the end of the experimental period were sacrificed under deep anaesthesia 24 h after injury.
Postmortem bronchoalveolar lavage
A modified 14 French Foley catheter was wedged in a subsegmental division of the left lower lobe, and 40 mL of room temperature normal saline was instilled and the lavage fluid was aspirated. Unspun samples were used to determine the bacterial and neutrophil counts (Hemavet HV950FS, Drew Scientific, Inc., Oxford, Connecticut, USA).
Postmortem lung wet-to-dry weight ratio
The right lung and the upper half of the left lower lobe were used for determination of bloodless wet-to-dry weight ratio.21
Statistical analyses
Bivariate analysis was used for baseline data. Continuous variables are expressed as mean ±SE and compared using one-way ANOVA tests with Bonferroni adjustments for multiple comparisons. Wet-to-dry weight ratios and bacterial and neutrophil counts in BAL fluid are presented as median with IQRs; they were compared using Kruskal–Wallis one-way analysis of variance, followed by Wilcoxon–Mann–Whitney tests with Bonferroni adjustments because they were not normally distributed.
For variables measured repeatedly over 24 h, the data are presented as mean and SEs at different time points, and include available data from the four sheep that expired prior to 24 h. To assess the impact of hMSC treatment on each measurement at the 24 h time point, analyses of covariance (ANCOVA) was performed, controlling for the baseline level. Only the 15 sheep that survived the full 24 h were included in the ANCOVA analyses at 24 h. Furthermore, a generalised estimating equation (GEE) approach was used to test the impact of hMSC treatment over time, taking repeated measurements into account and using an exchangeable correlation matrix with robust variance estimator. An interaction term with treatment group and time was introduced into the full model and was removed for p-values>0.05. A two-sided p-value <0.05 was considered statistically significant.
Results
There were no differences among the three study groups in any of the variables at baseline.
Mortality
Four sheep required euthanasia by the prespecified criteria before the end of 24 h, including 2 of 8 control sheep (at 12 h and 15 h), 1 of 7 lower-dose hMSC-treated sheep (at 18h) and 1 of 4 higher-dose hMSC-treated sheep (at 21 h).
Systemic haemodynamics
Heart rate increased in all three groups after injury compared to baseline (figure 1A). At 24 h, sheep treated with higher-dose hMSCs had an attenuated increase in heart rate compared with control sheep (p=0.01). In the 15 sheep alive at 24 h, systemic blood pressure (mean) was higher in sheep treated with higher-dose hMSCs at 24 h compared with controls (p=0.05). Systemic blood pressure in the high-dose group was also higher over the entire 24 h compared with controls (p=0.004) (figure 1B). The cardiac output did not differ among the three groups during the experimental period (table 1). Systemic vascular resistance index (figure 1C) was not different among the three groups. At 24 h, the pulmonary capillary wedge pressure (figure 1D) was lower only in the lower-dose hMSC-treated sheep (p=0.007). Except for one time point, the haematocrit was not different among the three groups (table 1). There were also no differences in arterial pH levels after the injury among the three groups (table 1).
Cardiac output, haematocrit and arterial pH in the three sheep groups over 24 h

(A) Heart rate in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3).*p=0.01 in the higher-dose hMSC group vs the control group at 24 h by ANCOVA. There were no significant differences among the treatment groups by the GEE. Data are expressed as mean±SEM. (B) Systemic arterial blood pressure (MAP) (mean) in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). *p=0.004 in the higher-dose hMSC group vs the control group at 24 h by ANCOVA. $p<0.05 in the higher-dose hMSC group vs the control group during the 24 h period by the GEE. There was no significant difference between the lower-dose hMSC group and the control group by the GEE. Data are expressed as mean±SEM. (C) Systemic vascular resistance index (SVRI in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). No difference was found among the three groups at 24 h by ANCOVA or during the 24 h by the GEE. Data are expressed as mean±SEM. (D) Pulmonary capillary wedge pressure (PCWP) in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). *p=0.007 in lower-dose hMSC-treated sheep compared with control sheep by ANCOVA at 24 h. There were no significant differences among the treatment groups by the GEE. Data are expressed as mean±SEM.
Pulmonary haemodynamics
The mean pulmonary arterial pressure increased after injury in all three groups and remained elevated throughout the study period (figure 2A). At 24 h, the surviving sheep treated with either lower or higher dose hMSCs had significantly attenuated increases in pulmonary arterial pressure compared with sheep in the control group (p<0.001 and p=0.008, respectively). Pulmonary arterial pressure was also lower during the 24 h period in the high-dose hMSC-treated sheep compared with the control sheep (p=0.04) (figure 2A). Pulmonary vascular resistance index (figure 2B) was not different at 24 h or during the experimental period.

(A) Pulmonary arterial pressure (PAP) in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). *p=0.008 in higher-dose hMSC-treated sheep compared with control sheep by ANCOVA at 24 h. #p<0.001 in lower-dose hMSC-treated sheep compared with control sheep by ANCOVA at 24 h. $p=0.04 in the higher-dose hMSC group vs the control group during the 24 h period by the GEE. There was no significant difference between the lower-dose hMSC group and the control group by the GEE. Data are expressed as mean±SEM. (B) Pulmonary vascular resistance index (PVRI) in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). No difference was found among the three groups at 24 h by ANCOVA. There were no significant differences among the treatment groups by the GEE. Data are expressed as mean±SEM.
Airway pressures
The peak and pause airway pressures increased in all three groups compared with baseline, but there were no differences among the groups over time or at 24 h (figure 3A and B). While peak airway pressures were numerically lowest in the higher-dose hMSC group, this difference did not quite reach significance (p=0.08).

(A) Peak airway pressure in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). There were no statistical differences in the lower-dose and higher-dose hMSC-treated sheep vs control sheep by ANCOVA at 24 h. There were no significant differences among the treatment groups by the GEE. Data are expressed as mean±SEM. (B) Pause airway pressure in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3). There were no differences in the lower and higher hMSC-treated groups vs the control group at 24 h by ANCOVA or during the 24 h experiment period by the GEE. Data are expressed as mean±SEM.
Lung lymph flow and protein balance
Lymph flow and lymph protein flux increased in all groups but there were no statistical differences among the groups (see online supplementary material).
Total fluid balance
The control sheep accumulated 3 L over 24 h and sheep treated with lower dose hMSCs accumulated 2.5 L, while sheep treated with the higher dose hMSCs had an even fluid balance (figure 4). The fluid intake was similar in all three groups, but the higher-dose hMSC-treated sheep had numerically more urine output. The differences in fluid balance were not statistically significant.
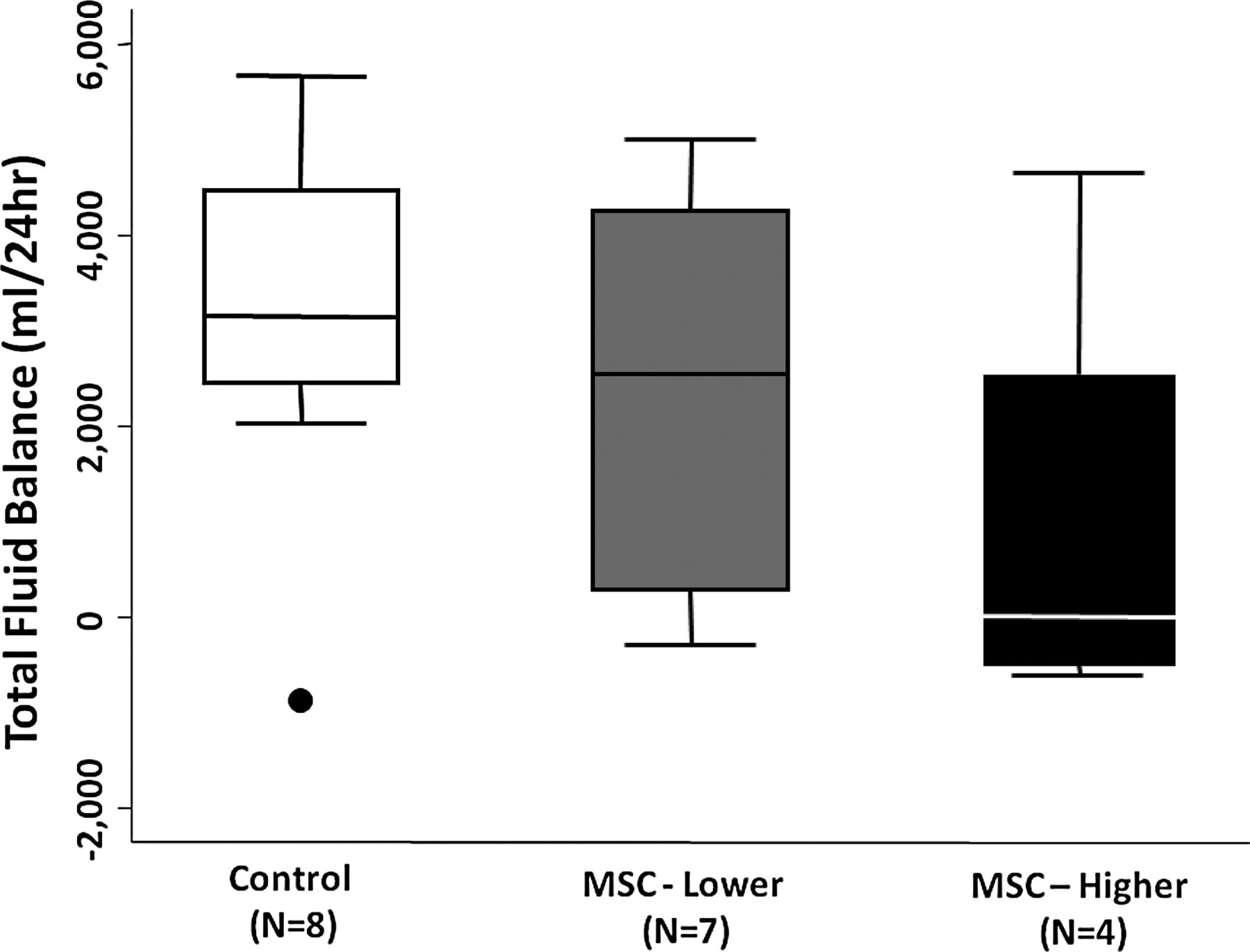
Total fluid balance (fluid in—urine output) in mL over the 24 h period in sheep treated with PlasmaLyte A alone (control) (n=8), lower-dose hMSCs (5×106 cells/kg) (n=7) and higher-dose hMSCs (10×106 cells/kg) (n=4). There were no differences among the three groups by Kruskal–Wallis equality-of-populations rank test. Data are expressed as median with 25–75% centiles.
Chemistry measurements
There were no differences in the serum BUN, creatinine, ALT, lactate or glucose among the three groups at baseline, 12 or 24 h (table 2). Serum AST was significantly lower in the sheep treated with lower dose hMSCs vs control sheep (p=0.03).
Serum measures of kidney and liver function, glucose and lactate in the three groups of sheep at baseline, 12 and 24 h
Oxygenation
The control sheep developed severe hypoxaemia that progressed throughout the experimental period; at 24 h the PaO2/FiO2 ratio was 97±15 mm Hg (figure 5). In the 15 sheep that remained alive at the 24 h time point, the PaO2/FiO2 ratio was significantly higher in both hMSC-treated groups compared with the control group (lower dose: 288±55 mm Hg (P=0.003); higher dose: 327±2 mm Hg (P=0.003)) (figure 5). The PaO2/FiO2 ratios in both the lower-dose and higher-dose hMSC groups were also numerically higher than in the control group over the 24 h period; this difference almost reached statistical significance (p=0.07 and p=0.053, respectively).

The PaO2/FiO2 ratio (mmHg) in sheep treated with PlasmaLyte A alone (control) (T0: n=8; T24: n=6), lower-dose hMSCs (5×106 cells/kg) (T0: n=7; T24: n=6) (n=7) and higher-dose hMSCs (10×106 cells/kg) (T0: n=4; T24: n=3) (n=4). *p=0.003 in higher-dose hMSC-treated sheep compared with control sheep by ANCOVA at 24 h. #p=0.003 in lower-dose hMSC-treated sheep compared with control sheep by ANCOVA at 24 h. There were no significant differences among treatment groups over the 24 h period by the GEE. Data are expressed as mean±SEM.
Bronchoalveolar lavage fluid bacterial and neutrophil counts
There were no differences in the median number of bacteria in control sheep or in the number of neutrophils (see online supplementary material).
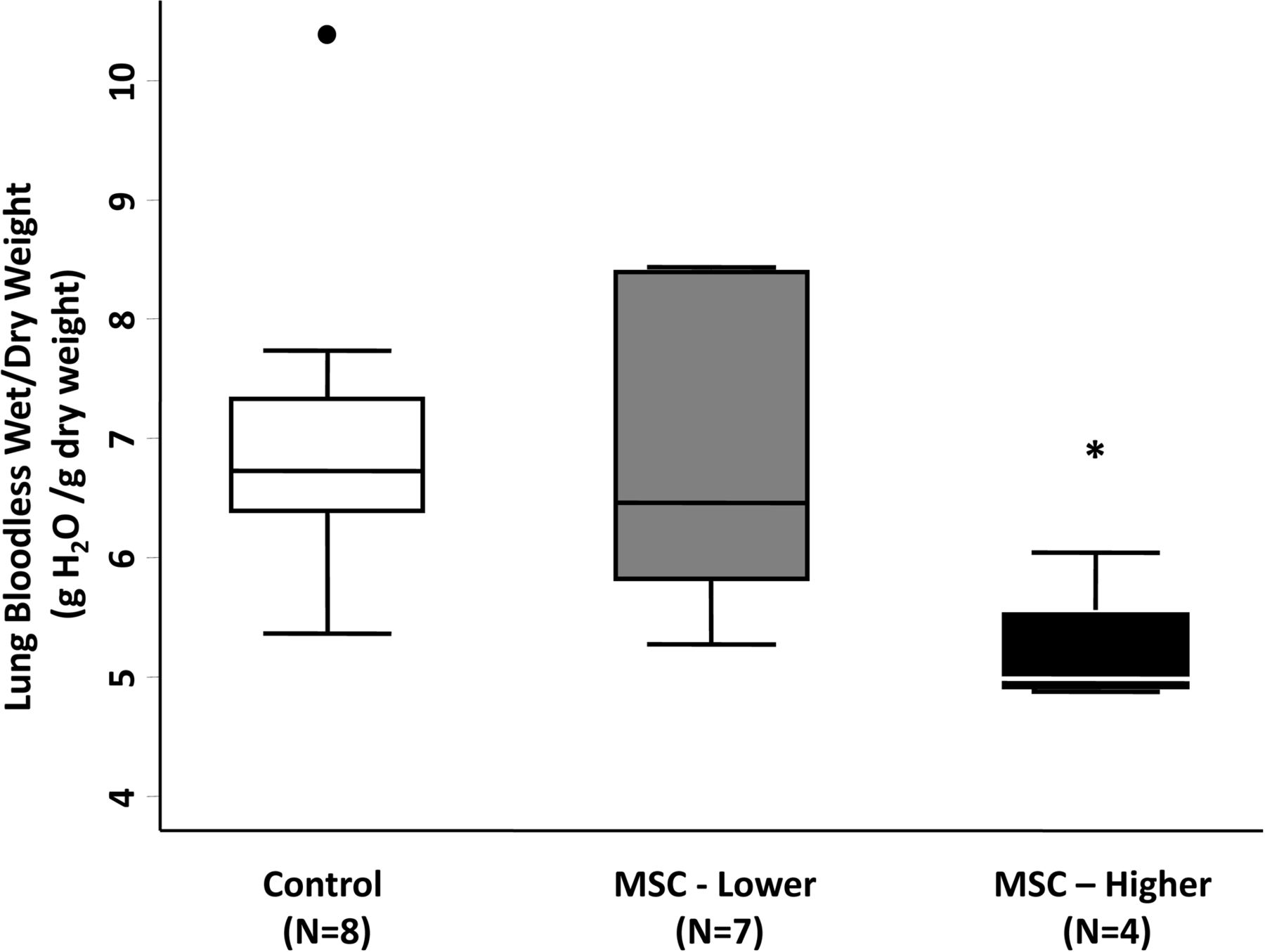
Postmortem extravascular lung water
Lung water content was lower in the higher-dose hMSC-treated group (median=5.0 g wet/g dry [IQR 4.9–5.8]) compared with the control group (median=6.7 g wet/g dry [IQR 6.4–7.5]) (p=0.01). There was no statistical difference in lung water content in the lower-dose hMSC-treated group compared with the control group (p=0.73) (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postmortem lung bloodless wet/dry weight ratio in sheep treated with PlasmaLyte A alone (control) (n=8), lower-dose hMSCs (5×106 cells/kg) (n=7) and higher-dose hMSCs (10×106 cells/kg) (n=4). *p=0.01 in higher-dose hMSC-treated sheep compared with control group by Mann–Whitney rank-sum test with Bonferroni adjustments. Data are expressed as median with 25–75% centiles.
Discussion
There were two primary objectives of this preclinical large-animal sheep study. The first was to test the safety of hMSCs in critically ill sheep with ALI. The second was to test the efficacy of hMSCs in the treatment of ALI with the primary focus on lung fluid balance and oxygenation, and to determine whether there were any significant differences between a lower and a higher dose of hMSCs. Both doses of hMSCs were well tolerated. Both doses of hMSCs were associated with improved oxygenation (PaO2/FiO2) at 24 h, and the higher dose of hMSCs decreased the quantity of postmortem pulmonary oedema. These results provide the foundation for translation to test hMSCs in critically ill patients with moderate-to-severe ARDS in a phase 1/2 clinical trial.22
We and other investigators have completed several preclinical studies in small animal models, as well as studies in an ex vivo perfused human lung preparation. Prior to this study, however, there had been no clinically relevant studies of hMSCs in a large animal model of ALI. This model is analogous to the clinical setting because the sheep were managed as if they were in an intensive care unit; three investigators stayed with the sheep at all times throughout the 24 h time period, adjusting the ventilator settings and fluid administration, and monitoring haemodynamics, gas exchange and several other variables. Additionally, the sheep received positive pressure ventilation and PEEP, similar to patients with ARDS. Thus, multiple features allowed by this large animal model make it more a more relevant comparison to human patients with ARDS; most of these features simply cannot be replicated in small animals or in the ex vivo perfused human lung.
Equally important, the sheep model made it possible to measure several clinically relevant physiological endpoints for both pulmonary and systemic circulation, and to obtain laboratory data regarding kidney function, liver function, and acid base status. Finally, we were able to measure peak and pause (plateau) airway pressure, as well as to obtain postmortem data on the quantity of pulmonary oedema, adding to our ability to test for safety and efficacy.
The testing of hMSCs in critically ill large animals with ALI for safety is perhaps most important. The safety record of hMSCs in several clinical trials has been excellent, but we wanted to determine whether intravenous administration of hMSCs would result in a significant increase in pulmonary arterial pressure (an effect that could decrease in right ventricular stroke volume and cause systemic hypotension). The results demonstrate that there were no differences in pulmonary vascular resistance, cardiac output or systemic vascular resistance among the three groups. In particular, mean pulmonary arterial pressure was significantly lower at 24 h in both the lower-dose and higher-dose hMSC-treated sheep compared with the control sheep. Thus, hMSCs did not compromise pulmonary haemodynamics and may have even exerted a favourable effect on the acutely injured pulmonary circulation. Similarly, the systemic arterial pressure was higher at 24 h in the higher-dose hMSC-treated sheep compared with the control and lower-dose hMSC-treated sheep, suggesting no deleterious effect of hMSCs on systemic haemodynamics, and potentially a favourable effect on systemic blood pressure with the higher hMSC dose. Taken together, these results provide some reassurance that testing of this cell-based therapy in patients with moderate-to-severe ARDS is warranted in terms of anticipated tolerability.
In regards to efficacy, oxygenation was significantly improved at 24 h in the sheep treated with either dose of hMSCs compared with the controls. There was also a trend for oxygenation to be higher in both hMSC-treated groups throughout the entire 24 h period, although this trend did not achieve statistical significance. Additionally, the postmortem measurement of extravascular lung water (a standard measure for the quantity of pulmonary oedema) showed a significant decrease in sheep treated with the higher dose of hMSCs. Although both doses were effective in improving oxygenation, the evidence that extravascular lung water was significantly reduced in the higher-dose hMSC group provides a rationale for making the higher dose (10×106 cells/kg) the target dose for testing tolerability and efficacy in a clinical trial of hMSCs for ARDS.
There are several limitations to this study. First, this study of ALI in sheep models only the first 24 h of human ARDS. Logistically it was not possible to sustain this model for more than 24 h. Second, it will not be possible to administer hMSCs in the clinical setting of ARDS within 1 h of injury to the lung. Thus, when tested in patients, the time window for treatment after ARDS develops will be longer. Third, although the sheep model includes the lung physiologic abnormalities that occur in patients with ARDS, and also replicates some of the process-of-care variables (positive pressure ventilation and intravenous fluid administration), it does not reflect the comorbidities that complicate the course of many patients with ARDS (eg, diabetes, immunosuppression and advanced age). Moreover, we did not test the effect of antibiotics in this model, although we have recently reported the differential effect of antibiotics and hMSCs in our ex vivo perfused human lung experiments.14 Finally, although investigators were not aware of the treatment arm to which sheep would be assigned before injury, they were not blinded to treatment group after injury.
In summary, administration of hMSCs in sheep with severe lung injury demonstrated no safety issues. Moreover, there was evidence of efficacy in terms of improved oxygenation with either dose of hMSCs, and a decrease in the quantity of pulmonary oedema in the sheep treated with the higher dose of hMSCs. Based on these results, our plan is to proceed to clinical testing of allogeneic bone marrow-derived hMSCs in patients with moderate-to-severe ARDS with an FDA-reviewed clinical trial22
Acknowledgments
This work was supported by NIH Grant GM097480-01A1 (PE), and Shriners Hospital of North America Grants SHC85500 (PE) & 84050 (DLT). Clinical grade, cryopreserved human allogeneic MSCs were obtained from an NIH-supported Production Assistance for Cellular Therapies group (Molecular and Cellular Therapeutics, UMN), Contract # HHSN268201000008C. We want to acknowledge the major contributions of both Dr Traber and his wife, Lillian Traber, both of whom have passed away since these experiments were completed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figure
Footnotes
-
SA and HI contributed equally.
-
Contributors SA: collection and/or assembly of data, data analysis and manuscript writing; HI: surgical procedures, collection and/or assembly of data and data analysis; DLT: study conception and design, financial support, data analysis and interpretation; JWL: design of the experiments, preparation of the mesenchymal stem cells, interpretation of the results and manuscript writing; RAC and HKH: design, data analysis and manuscript editing; DFM: design of the experiments, data interpretation and manuscript writing; DHM: preparation of the mesenchymal stem cells, interpretation of the results and manuscript writing; LDT: surgical procedures and experimental design; HZ: data entry, statistical analyses of all the data, manuscript and figure preparation; JW: manuscript writing and editing, and composition of the tables; DNH: concept development and study design; DSP: concept development, study design and data interpretation; KDL: experimental design, data interpretation and manuscript editing; MAM: experimental design, data analysis, data and table organisation, and manuscript writing; PE: experimental design, surgical procedures, data analysis and interpretation, financial support, concept development, manuscript writing and responsible for overall content as guarantor.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.