Article Text

Statistics from Altmetric.com
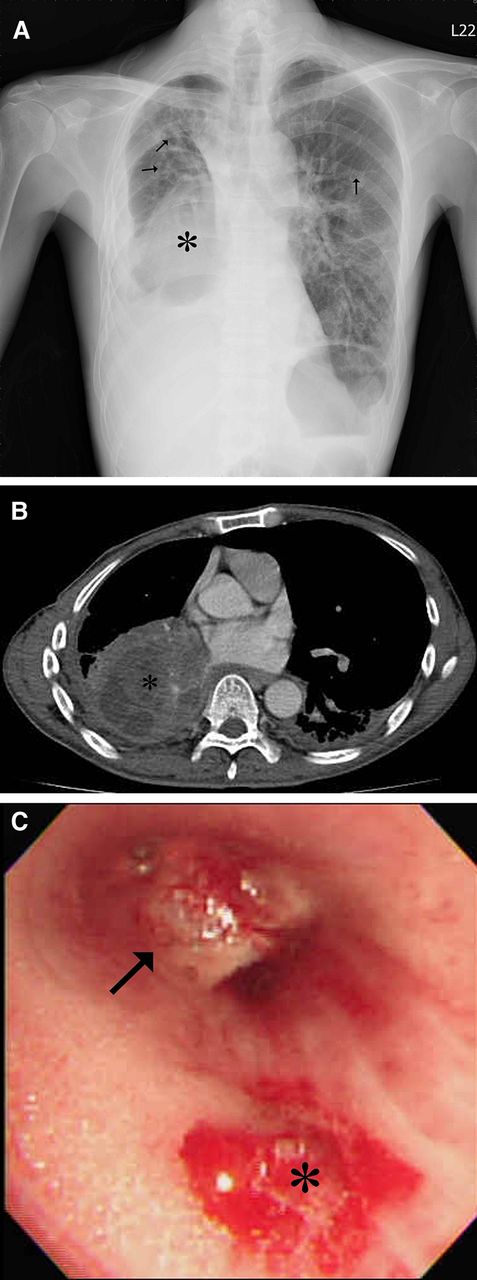
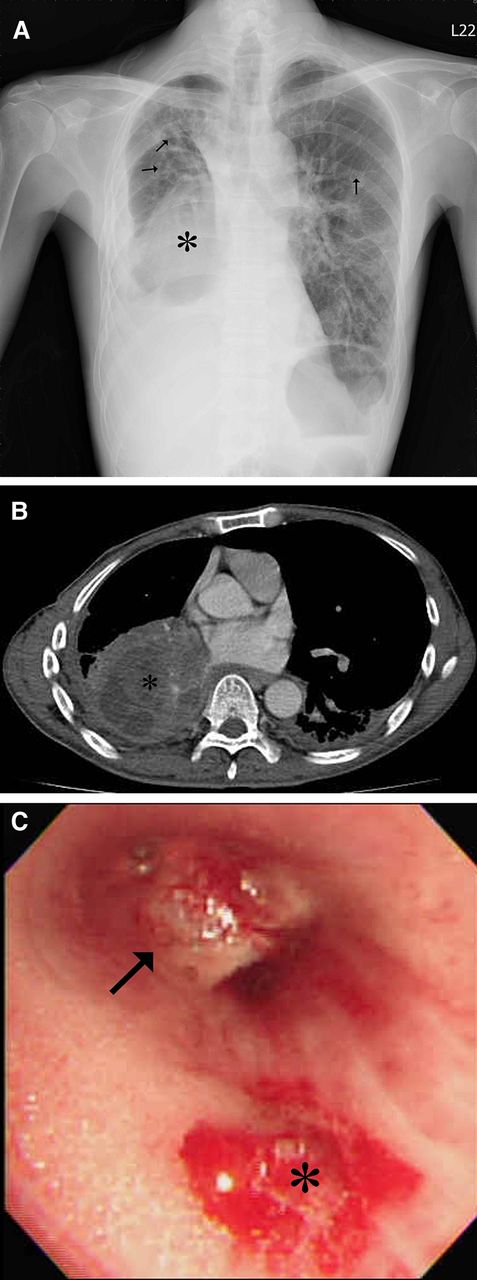
A 49-year-old male had history of recurrent laryngeal papillomatosis spreading to the bronchus and lung parenchyma since childhood. He had been treated with repeated endoscopic CO2 laser excision (figure 1). He had no smoking history. He was admitted with a 3-day history of worsening fever, cough and dyspnoea. Chest radiography showed a right lower lung mass, bronchiectasis, many cystic lesions and right pleural effusion (figure 2A). The right lower lobe mass measured 8.8×7.0 cm and had central hypodense areas consistent with necrosis (figure 2B, taken 8 years after figure 1) and there was mediastinal lymphadenopathy. Fiberoptic bronchoscopy showed numerous papillomas in the respiratory tract consistent with respiratory papillomatosis and an endobronchial tumour obliterating the right lower lobe bronchus, which bled on contact (figure 2C). Histopathology proved it a squamous cell carcinoma with papillomas identified in the tumour. Recurrent respiratory papillomatosis with malignant transformation was diagnosed. The patient received target therapy with erlotinib (Tarceva) and radiotherapy.

Coronal reconstructed CT image demonstrates multiple nodules (arrows) in the respiratory tract and multiple thin-walled cystic lesions (asterisks) in the lung parenchyma, indicating laryngeal papillomatosis with downward spreading to the airway and lung.
{kind=link}
{kind=link}
(A) Chest radiography disclosed a right lower lung mass opacity (asterisk), bronchiectasis, many cystic lesions (arrows) and right pleural effusion (B) Contrast-enhanced CT scan demonstrates a growing mass lesion in the right lower lobe (asterisk) with central hypodense areas indicating necrosis. (C) Fiberoptic bronchoscopy discloses an endobronchial tumour (arrow) obliterating the right lower lobe bronchus, which easily bled on contact (asterisk).
Recurrent respiratory papillomatosis, caused by infection with human papillomavirus, is usually localised to the laryngeal and subglottic region. Tracheal involvement has been reported to occur in 5% of cases, and fewer than 1% of cases show lung involvement.1 The image features of respiratory papillomatosis are solid or cystic nodules predominantly in the lower lobes, tracheal wall irregularity due to scars and papillomas, and bronchiectasis from obstruction and secondary infection. Malignant transformation into squamous cell carcinoma occurs in 2–3%, usually within 10 years of the diagnosis of pulmonary recurrent respiratory papillomatosis.2 Clinicians should suspect malignant transformation when growth of a pulmonary nodule or mass is detected by serial imaging.
Key messages
-
Extra laryngeal spread in patients with recurrent respiratory papillomatosis is rare.
-
The radiographic features of respiratory papillomatosis are solid or cystic nodules predominantly in the lower lobes, tracheal wall irregularity due to scars and papillomas and bronchiectasis from obstruction and secondary infection.
-
Clinicians should suspect malignant transformation when growth of a pulmonary nodule or mass is detected by serial x-ray or CT.
Footnotes
-
Contributors ELS, MFL, JHH: concept, drafting, and revision of article. MTW: interpretation of imaging study. All authors gave final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.