Article Text

Abstract
Background Viral respiratory infection (VRI) is a common cause of pulmonary exacerbations in children with cystic fibrosis (CF). The importance of VRI in adult CF populations is unclear.
Objective To determine the incidence and clinical impact of VRI among adults with CF.
Methods One hundred adults with CF were followed up prospectively for 12 months. Sputum, nose swabs and throat swabs were collected every 2 months and at onset of pulmonary exacerbation. PCR assays for adenovirus, influenza A&B, human metapneumovirus, parainfluenza 1–3, respiratory syncytial virus and human rhinovirus were performed on each sample. Symptom scores, spirometry and inflammatory markers were measured at each visit.
Results One or more respiratory viruses were detected in 191/626 (30.5%) visits. Human rhinovirus accounted for 72.5% of viruses. Overall incidence of VRI was 1.66 (95% CI 1.39 to 1.92) cases/patient-year. VRI was associated with increased risk of pulmonary exacerbation (OR=2.19; 95% CI 1.56 to 3.08; p<0.001) and prescription of antibiotics (OR=2.26; 95% CI 1.63 to 3.13; p<0.001). Virus-positive visits were associated with higher respiratory symptom scores and greater C-reactive protein levels. Virus-positive exacerbations had a lower acute fall in FEV1 than virus-negative exacerbations (12.7% vs 15.6%; p=0.040). The incidence of exacerbations, but not VRI, was associated with greater lung function decline over 12 months (−1.79% per pulmonary exacerbation/year; 95% CI −3.4 to −0.23; p=0.025).
Conclusion VRI is common in adults with CF and is associated with substantial morbidity. Respiratory viruses are a potential therapeutic target in CF lung disease.
- Cystic Fibrosis
- Viral Infection
Statistics from Altmetric.com
Key messages
What is the key question?
-
How common are viral respiratory infections (VRIs) among adults with cystic fibrosis (CF) and what clinical impact do such infections have?
What is the bottom line?
-
Adults with CF have an average of 1–2 viral infections per year; these infections are strongly associated with pulmonary exacerbations, increased respiratory symptoms, raised inflammatory markers and a greater requirement for antibiotic therapy.
Why read on?
-
This study describes detailed epidemiological, clinical and microbiological characteristics of VRIs in adults with CF. Respiratory viruses represent an underexploited therapeutic target in CF lung disease.
Introduction
Viral respiratory infections (VRIs) such as the common cold are associated with substantial morbidity among the general population.1 ,2 Respiratory viruses are of even greater significance for people with chronic airways diseases and are implicated in exacerbations of both asthma and chronic obstructive pulmonary disease.3–8
Studies in children with cystic fibrosis (CF) suggest an incidence of up to five cases of VRI per patient-year. Viral infections in this population are associated with increased respiratory symptoms and disease progression.9–13 Up to 64% of pulmonary exacerbations in paediatric CF populations are associated with respiratory viruses,11 yet the literature on VRI in adults with CF is sparse. Small studies in adults have identified a respiratory virus in up to 68% of pulmonary exacerbations, while case reports show that viruses such as influenza have the potential to cause severe respiratory infection in this patient group.14–17 There is also increasing in vitro evidence to demonstrate interactions between respiratory viruses, bacteria and host immune defences, which may have direct relevance to the pathogenesis of CF lung disease.18 19
To date, however, no large-scale, longitudinal study has been carried out to examine respiratory viruses in adult patients with CF. We performed a single-centre, prospective study to determine the incidence and clinical impact of VRI in a cohort of adults with CF. Preliminary data from this study have previously been presented in abstract form.20
Methods
Participants and study design
Patients aged ≥18 years attending the Manchester Adult Cystic Fibrosis Centre were invited to participate. The first 100 respondents were recruited. The only exclusion criterion was previous lung transplantation. Recruitment was completed between December 2010 and March 2011 and all patients gave written informed consent. The study was approved by the Greater Manchester West research ethics committee (reference 10/H1014/71).
Participants were followed up for 12 months or until death or lung transplantation. During follow-up, patients were seen routinely every 2 months. Between scheduled visits, patients were asked to contact the investigators when they developed symptoms of a pulmonary exacerbation (PEx) or upper respiratory tract infection (URTI). An additional study visit was then conducted within 48 h. Clinicians were blinded to the results of virological tests when making treatment decisions at each study visit.
Detection of respiratory viruses
Sputum, nose swabs and throat swabs were collected at each visit for virological analysis. Sputum was expectorated spontaneously by the patient into sterile containers. Flocked swabs were collected from the nose and posterior pharynx and conveyed in viral transport medium at room temperature. Sputum or viral transport medium was mixed in a 1 : 1 ratio with AL lysis buffer (Qiagen, Hilden, Germany) before being inactivated at 80°C for 20 min. Total nucleic acids were extracted using the QIAamp Virus Biorobot MDx instrument (Qiagen, Hilden, Germany), in accordance with the manufacturer's instructions. In-house PCR assays were performed to identify the presence of adenovirus, influenza A&B, human metapneumovirus, parainfluenza 1–3, respiratory syncytial virus and human rhinovirus. Details of the PCR assays, primers and probes are given in the online supplementary table S1. PCR cycle threshold (CT) values of <45 were considered positive. Lower CT values indicate that fewer cycles of PCR amplification were needed to detect viral nucleic acids and, therefore, reflect a stronger degree of PCR positivity.
Genetic sequencing of rhinoviruses
Genetic sequencing was performed on a subset of rhinoviruses identified during the study. All rhinovirus-positive sputum samples with a CT value <40 were selected for sequencing as well as upper airway swabs from patients with two or more consecutive rhinovirus-positive visits. Total nucleic acids were extracted as described above. Sequencing of the rhinovirus 5′ untranslated region was performed using the Applied Biosystems 3130xl Genetic Analyzer (Life Technologies Ltd, Paisley, UK) following a modification of the method reported by Lee et al,21 which is described in detail in the online supplementary appendix. Rhinovirus sequences were identified through phylogenetic analysis and comparison with the GenBank database using BLASTn. Sequences have been deposited with GenBank under accession numbers KF112083–KF112142.
Clinical parameters
PEx was defined according to a modification of the criteria described by Fuchs et al22: four or more symptoms and a requirement for intravenous or oral antibiotics was considered an exacerbation. URTI symptoms were quantified using the score described by Johnston et al.3 Spirometry was performed at each visit using the Vitalograph 2150 volumetric spirometer (Vitalograph Ltd, Buckingham, UK) in line with accepted standards.23 Baseline forced expiratory volume in 1 s (FEV1) was taken as the best value in the 3 months before the study and compared with the best value in the 3 months after study completion. Full blood count and serum C-reactive protein levels were measured at each visit.
Statistical analysis
The sample size was determined using McNemar's test, assuming significance at the 5% level. Ninety-four patients gave 80% power to detect a 20% difference in the proportion of virus-positive events among exacerbation visits compared with stable visits. The power calculation assumed that a third or more visits were positive for a virus overall. A recruitment target of 100 patients was set to allow for patient drop-out. The incidence of VRI is reported as the mean number of virus-positive visits per person-year and was calculated using a univariable Poisson regression model offset by the natural log of follow-up duration. Patients followed up for <6 months were excluded from incidence calculations. A multivariable Poisson regression model was used to evaluate the effect of demographic variables on the incidence of VRI. The variables included in this model were selected a priori based on factors known to increase the risk of VRI in the general population or to be of prognostic importance in CF.
Analysis of longitudinal outcomes used methods which take account of repeated observations from individual participants. Assessment of the association between VRI and other clinical outcomes used generalised estimating equation models employing an exchangeable correlation structure. Generalised estimating equation models with a logistic regression structure were selected for binary outcomes while a linear regression structure was used for continuous variables. Multiple linear regression was used to assess the impact of PEx and VRI on the rate of decline in FEV1. Univariable analyses were conducted in addition to a multivariable model adjusted for age and sex. Data are presented as mean (SD) or median (IQR), as appropriate. Variables which were not normally distributed were subject to log-transformation before inclusion in statistical models and this is highlighted in the manuscript where it has been used. A significance level of 0.05 was assumed unless stated otherwise. Statistical analysis was performed using SPSS V.20.0 (IBM, New York, USA).
Results
Patient demographics
One hundred patients were recruited. Baseline demographics of the participants are detailed in table 1. One participant was lost to follow-up and one withdrew from the study after the baseline visit. The remaining 98 patients completed a mean of 6.6 (SD 1.7) study visits over 11.5 (SD 2.0) months. Four patients were followed up for <6 months leaving 94 patients in the VRI incidence calculations. Three patients died during the study and one underwent bilateral lung transplantation. Uptake of the seasonal influenza vaccination in the autumn before the study was 89%.
Baseline demographics of study participants
Identification of respiratory viruses
Virology results were available for 626/649 completed study visits. Of these, 191 (30.5%) were positive for a respiratory virus, including nine episodes of dual viral infection. Rhinovirus accounted for 72.5% of viruses identified. The distribution of viruses detected is shown in figure 1. Details of the dual viral infections are given in online supplementary table S2.

Breakdown of viruses identified during the study. RSV, respiratory syncytial virus.
The overall incidence of VRI was 1.66 (95% CI 1.39 to 1.92) cases/patient-year. Rhinovirus had the highest incidence at 1.17 (95% CI 0.95 to 1.39) cases/patient-year. Equivalent values for other viruses were: metapneumovirus 0.28 (0.17 to 0.39), influenza A 0.08 (0.02 to 0.13), adenovirus 0.08 (0.02 to 0.13), influenza B 0.05 (0.01 to 0.10), parainfluenza virus 1–3 0.05 (0.01 to 0.10) and respiratory syncytial virus 0.04 (0.001 to 0.09) cases/patient-year. Eighty of 94 patients (85%) had at least one episode of laboratory-confirmed VRI during the study. Demographic variables did not have a significant effect on the incidence of VRI (see table 2).
Demographic risk factors for viral respiratory infection
Genetic sequencing of rhinovirus strains
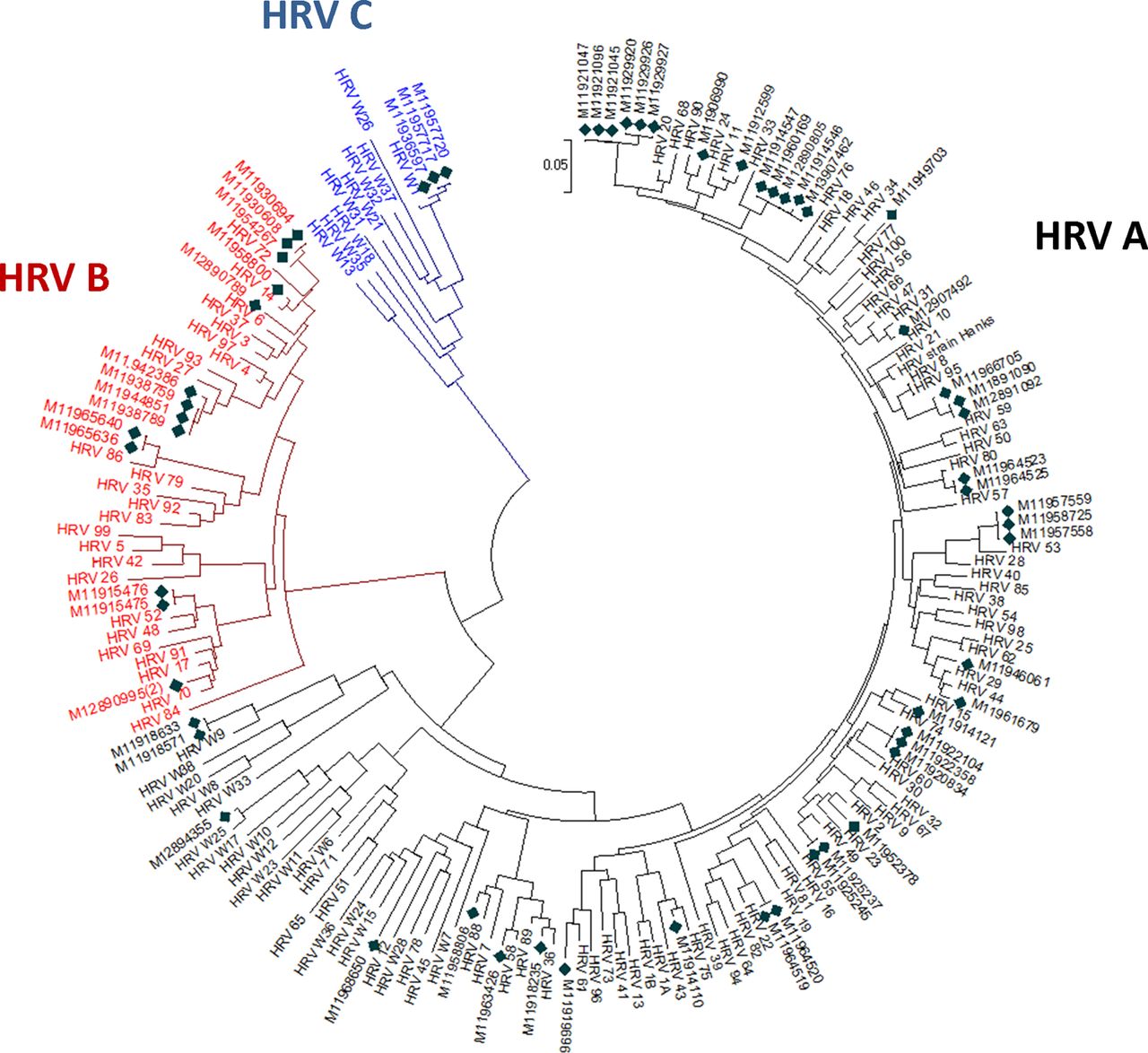
The rhinovirus 5′ untranslated region was sequenced successfully from 61 respiratory tract specimens known to be PCR positive for rhinovirus. These samples were collected at 42 study visits from 27 separate patients and comprised 29 sputum specimens, 21 nose swabs and 11 throat swabs. Thirty-five different rhinovirus subtypes were identified in total. Human rhinovirus A was detected at 29/42 visits (69.0%) with 11/42 visits (26.2%) positive for human rhinovirus B. Human rhinovirus C was detected in only 2/42 (4.8%) visits. There were no cases of simultaneous infection with different rhinovirus subtypes. One patient appeared to harbour the same strain of rhinovirus A at three separate study visits over a period of 10 months. No other cases of persistent rhinovirus infection were identified in the cohort. Figure 2 shows a phylogenetic tree to illustrate the diversity of rhinoviruses sequenced in this study.

Phylogenetic tree showing rhinoviruses detected in clinical samples from this study and reference rhinovirus strains reported by Lee et al.22 The phylogenetic tree was constructed in MEGA 5.1 using the neighbour joining method with bootstrap values of 500. ♦ indicates study samples. HRV, human rhinovirus.
Rhinovirus A infection seemed to have more severe clinical outcomes than rhinovirus B (see online supplementary table S3). Rhinovirus A-positive visits had greater URTI scores (12.5 (SD 7.1) vs 6.5 (SD 5.6); p=0.014) and higher C-reactive protein levels (geometric mean 15.9 (range 0–140) vs 6.0 (2–24); p=0.008) than rhinovirus B-positive episodes.
Association between VRI and pulmonary exacerbation (PEx)
Data were available for both exacerbation and virology status in 609 visits. Of these, 229 (37.6%) episodes met the predefined criteria for PEx. Patients had a mean of 2.6 (SD 1.8) exacerbations/patient-year. Forty per cent of exacerbations were positive for a virus compared with 24% of non-exacerbation visits. Identification of a virus was associated with increased risk of PEx (OR=2.19; 95% CI 1.56 to 3.08; p<0.001). Overall, 306/649 (47%) visits resulted in a prescription for antibiotics, of which 49% were for intravenous antibiotics. Virus-positive episodes were associated with a greater likelihood of any antibiotic prescription (OR=2.26; 95% CI 1.63 to 3.13; p<0.001) but there was no significant increase in the prescription of intravenous antibiotics (OR=1.30; 95% CI 0.94 to 1.81; p=0.114).
The mean PCR CT value for virus-positive specimens was 37.1 (SD 5.8) cycles, with lower CT values indicating a stronger degree of PCR positivity. Lower CT values were a significant predictor of meeting the criteria for PEx (OR=0.92; 95% CI 0.88 to 0.97; p<0.001) and for prescription of antibiotics (OR=0.89; 95% CI 0.83 to 0.95; p<0.001).
Impact of VRI on acute and long-term changes in FEV1
The mean difference between the FEV1 at baseline and a given study visit was similar at virus-positive and virus-negative episodes (8.7 vs 9.4%; p=0.412). When exacerbations were considered separately, virus-positive PEx were associated with a smaller fall in FEV1 than virus-negative PEx (12.7% (SD 1.3) vs 15.6% (SD 1.4); p=0.040).
In comparison with baseline values, the end of study FEV1 fell by a mean of 1.5% (SD 12.4). There was no evidence of a significant association between the number of virus-positive visits per year and an increased rate of decline in FEV1 over the study period (−0.88% per VRI/year; 95% CI −2.7 to +0.95; p=0.268). The number of PEx per year did have a significant association with decline in FEV1, which persisted after adjustment for baseline demographics and number of viral infections (see table 3).
Effect of incidence of pulmonary exacerbations and viral respiratory infections on rate of decline in FEV1 over 12 months using a multiple linear regression model
Effect of VRI on symptoms and inflammatory markers
Virus-positive visits were associated with a mean URTI score of 7.6 (SD 6.3) out of 27 compared with 5.3 (SD 4.6) for virus-negative visits (p<0.001). Mean Fuchs PEx scores, from a maximum value of 12, were 3.6 (SD 2.3) and 2.9 (SD 2.4) in the virus-positive and negative groups, respectively (p<0.001). The odds of virus-positive visits being associated with individual symptoms are shown in supplementary table S4. Increased cough, change in sputum, increased dyspnoea, sinus discharge, sore throat and hoarse voice were all significantly more likely at virus-positive visits. Among virus-positive visits, 22.8% were minimally symptomatic as defined by a total of <4 in both the URTI and PEx scores. VRI was associated with higher C-reactive protein levels (geometric mean 10.3 (range 0–244) vs 8.4 (0–165); p=0.004) and lower lymphocyte counts (1.83 vs 1.94×109; p=0.011) than virus-negative visits.
In comparison with visits positive for other viruses, rhinovirus infection was associated with a similar rate of PEx (47.8% vs 48.6%, respectively). Non-rhinovirus VRI was associated with an increased rate of prescription of intravenous antibiotics (41.3% vs 21.0%; p=0.011) but rhinovirus infection was otherwise comparable in severity to that of other viruses (see table 4).
Clinical outcomes for rhinovirus-positive visits in comparison with visits positive for other viruses
Diagnosis of VRI
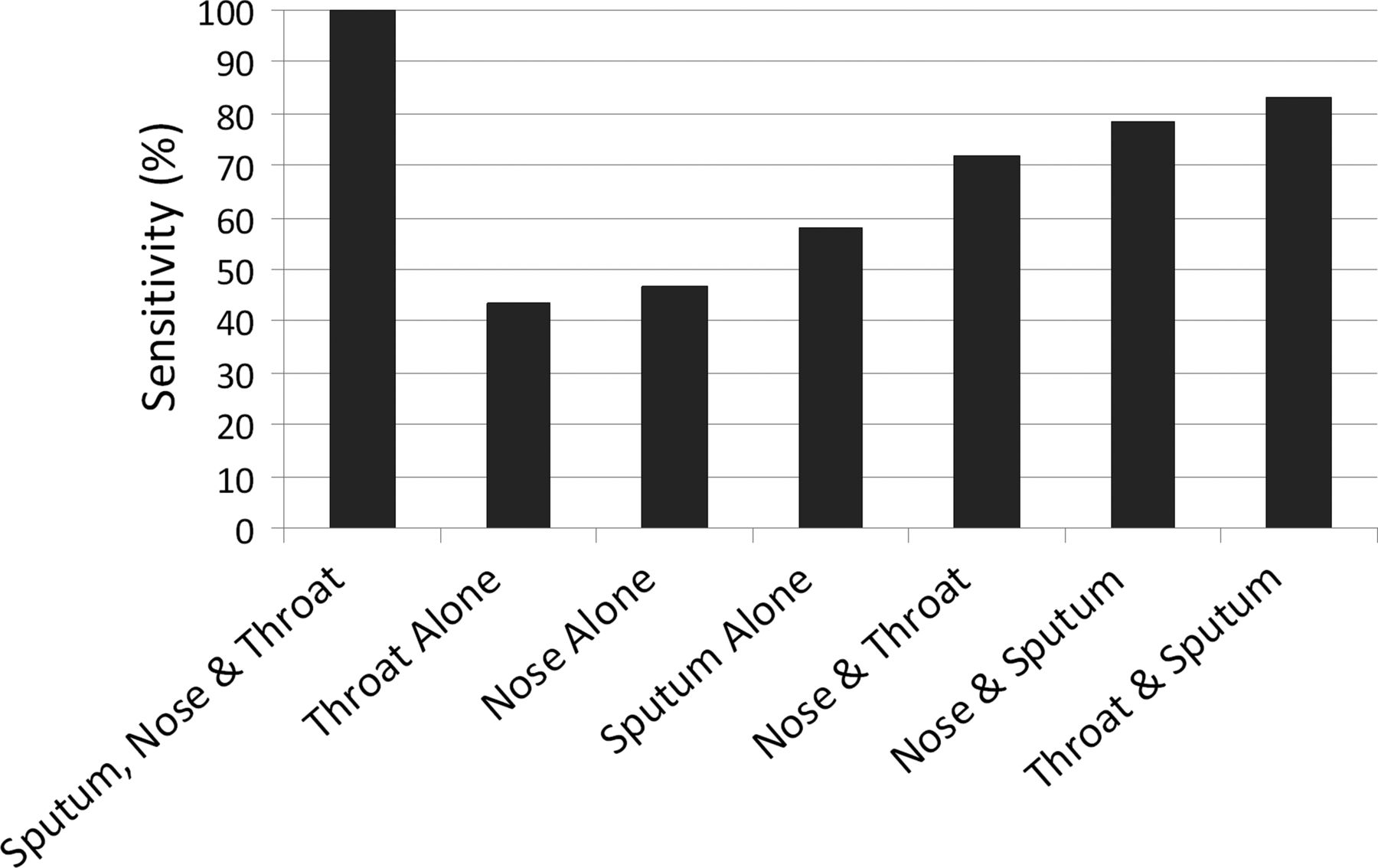
Complete sets of virology samples (ie, sputum, nose swabs and throat swabs) were collected at 469 visits. Samples were missing most commonly because the patient was unable to expectorate sputum. One or more viruses were detected at 151/469 (32.2%) visits. Of these, 100 (66.2%) were positive in only one of the three specimen types, 30 (19.9%) in two and 21 (13.9%) in all three specimen types. Sputum samples identified 58.0% of viruses compared with 46.7% for nose swabs and 43.3% for throat swabs. The sensitivity of different specimen combinations is shown in figure 3. Sputum samples identified a wider diversity of viral pathogens than upper airway swabs (see online supplementary figure S1).

{kind=link}
{kind=link}
{kind=link}
Sensitivity of different combinations of sputum, nose swabs and throat swabs for the diagnosis of viral respiratory infection in adults with cystic fibrosis.
Receiver operating characteristic analysis suggests that the URTI score has limited usefulness for the prediction of laboratory-confirmed VRI in adults with CF (see online supplementary figure S2). The original diagnostic threshold of ≥4/27 gave a sensitivity of 0.68 (95% CI 0.45 to 0.86) and specificity of 0.51 (0.40 to 0.63). Positive and negative predictive values were 0.28 and 0.85, respectively, with an area under the receiver operating characteristic curve of 0.68 (95% CI 0.54 to 0.81).
Discussion
This paper presents the results of the first large-scale, prospective study to document the incidence of VRI in adults with CF. Our experience shows that respiratory viruses are common in this population and are strongly associated with pulmonary exacerbations and increased morbidity. The overall incidence of VRI in our study is consistent with previous paediatric CF studies and it is now clear that respiratory viruses have an important role in CF lung disease in adults as well as children.9–13 ,24
We identified human rhinovirus as overwhelmingly the most common viral pathogen in adults with CF. Rhinovirus belongs to the Picornaviridae family of viruses and is the principal cause of the common cold.25 For patients with airway diseases, rhinovirus is a greater problem and is associated with most acute asthma attacks.3 ,7 The predominance of rhinovirus in our study mirrors data from children with CF and confirms that rhinovirus is an important CF pathogen.10–13 Our data also show that rhinovirus A is the predominant rhinovirus species to affect adults with CF. We have not detected a prominent role for the recently identified rhinovirus C species, which contrasts sharply with the findings of de Almeida and colleagues in their paediatric cohort.11 Our study has shown in CF for the first time that rhinovirus A has more severe clinical outcomes than rhinovirus B, which may have implications for the development of future antirhinoviral treatments.
The relationship between pulmonary exacerbations, respiratory viruses and decline in lung function warrants close analysis. Most paediatric CF studies have found accelerated lung function decline in patients with more frequent viral infections.12 ,13 ,26 We found that respiratory viruses double the risk of PEx and, separately, that the incidence of PEx is linked to an increased rate of FEV1 deterioration. Despite this, our data do not show a statistically significant link between incidence of VRI and lung function decline.
Explanations might include the fact that our study was not powered to detect changes in lung function and a larger study might have unveiled an effect of viral infections on FEV1 decline. In addition, respiratory viruses were associated with a wide spectrum of clinical severity in our study. The “noise” from asymptomatic viral infections might have masked the impact of more harmful viruses. Finally, the unusually low incidence of influenza over the winter of 2011–2012 and our high vaccine coverage rate might have had an impact on our results;27 only one case of influenza was seen over the entire second winter of the study.
An important finding of this study is the detection at 24% of study visits of a respiratory virus which did not meet the prespecified criteria for PEx. The prevalence of VRI during clinical stability has not been reported before among adults with CF but the rate in paediatric patients has varied from 13 to 53%.10 ,11 ,24 ,28 Our data are therefore broadly consistent with the paediatric CF literature. It is important to note that PEx is not a binary phenomenon. Acute deteriorations in CF lung disease represent a spectrum of events and the visits not meeting the criteria for PEx are likely to have included ‘mild’ exacerbations and pure upper respiratory viral infections.
Before this study, little was known about the symptom burden associated with respiratory viruses in adults with CF. We have shown that VRI is associated with characteristic symptoms, including sore throat, sinus discharge and hoarse voice. Other symptoms associated with VRI included increased cough, change in sputum and dyspnea, which are extremely common in patients with CF. In general, many of the symptoms associated with VRI are non-specific and this probably explains the poor diagnostic accuracy of the URTI symptom score in our population. It should be noted that the Johnston URTI score was originally used in a paediatric asthma study and has not been validated for use in CF.3 The score did have a high negative predictive value but our findings suggest that URTI symptoms should not be used as a surrogate for laboratory-confirmed VRI in clinical practice or future research in CF. Olesen et al24 reached similar conclusions among paediatric patients with CF.
Our study has also presented new data on the optimal means of diagnosing VRI in CF. We have previously shown that CF sputum is suitable for the diagnosis of VRI using PCR.15 In contrast to a recent paediatric study,28 we found that sputum had higher viral identification rates than upper airway swabs and detected a greater variety of viruses. This presumably reflects the greater ease with which most adult patients expectorate sputum. Our study suggests that a combination of sputum and upper airway samples is required to maximise diagnostic sensitivity in adults with CF.
A number of limitations of this study need to be recognised and it is likely that our results underestimate the true incidence of VRI. First, our PCR panel of nine respiratory viruses is not exhaustive and did not include bocavirus, coronavirus or parainfluenza 4. In addition, the study design required patients to contact the CF centre at onset of new respiratory symptoms so mild illnesses might have gone unreported. The planned strategy of testing sputum, nose swabs and throat swabs was achieved in only 72% of study episodes. This reflects ‘real-life’ practice where patients often vary in their ability to produce sputum. Finally, we used the aggregate number of symptoms making up the Fuchs criteria as both a diagnostic tool and a surrogate marker for the severity of lower respiratory tract symptoms. The Fuchs criteria were not designed for use in this way but we took the pragmatic approach of assuming a correlation between the number of PEx symptoms and exacerbation severity.
Allowing for these limitations, our study has shown a clear link between respiratory viruses and exacerbations in adults with CF. PEx are extremely important events in CF and are linked to impaired quality of life,29 declining lung function30 and increased mortality.31 PEx remain common despite the availability of established prophylactic treatments such as maintenance antibiotics and mucolytic agents. The need for additional treatments to prevent such exacerbations, therefore, is clear. Our findings suggest that respiratory viruses, especially rhinovirus, represent a potential therapeutic target in CF lung disease.
In summary, we have demonstrated that respiratory viruses are common pathogens in adults with CF and are strongly linked to pulmonary exacerbations. Further research needs to be directed towards understanding the pathophysiology of these infections and virus–bacteria interactions within the CF lung. Such studies may ultimately lead to effective new treatments to prevent virus-induced exacerbations in patients with CF.
Acknowledgments
We are very grateful to Alan Lord, Chris Parker, Helen Flight and the MACFC nursing staff for assistance with the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors WGF was involved in study design, data collection, data analysis and wrote the first draft. All other authors contributed to study design, data collection or analysis and all authors helped to revise the manuscript.
-
Funding The study was funded by the Manchester Adult Cystic Fibrosis Centre's charitable fund.
-
Competing interests None.
-
Ethics approval Greater Manchester West NHS research ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.