Article Text

Abstract
Background This study aimed to assess associations of outdoor air pollution on prevalence of chronic bronchitis symptoms in adults in five cohort studies (Asthma-E3N, ECRHS, NSHD, SALIA, SAPALDIA) participating in the European Study of Cohorts for Air Pollution Effects (ESCAPE) project.
Methods Annual average particulate matter (PM10, PM2.5, PMabsorbance, PMcoarse), NO2, nitrogen oxides (NOx) and road traffic measures modelled from ESCAPE measurement campaigns 2008–2011 were assigned to home address at most recent assessments (1998–2011). Symptoms examined were chronic bronchitis (cough and phlegm for ≥3 months of the year for ≥2 years), chronic cough (with/without phlegm) and chronic phlegm (with/without cough). Cohort-specific cross-sectional multivariable logistic regression analyses were conducted using common confounder sets (age, sex, smoking, interview season, education), followed by meta-analysis.
Results 15 279 and 10 537 participants respectively were included in the main NO2 and PM analyses at assessments in 1998–2011. Overall, there were no statistically significant associations with any air pollutant or traffic exposure. Sensitivity analyses including in asthmatics only, females only or using back-extrapolated NO2 and PM10 for assessments in 1985–2002 (ECRHS, NSHD, SALIA, SAPALDIA) did not alter conclusions. In never-smokers, all associations were positive, but reached statistical significance only for chronic phlegm with PMcoarse OR 1.31 (1.05 to 1.64) per 5 µg/m3 increase and PM10 with similar effect size. Sensitivity analyses of older cohorts showed increased risk of chronic cough with PM2.5abs (black carbon) exposures.
Conclusions Results do not show consistent associations between chronic bronchitis symptoms and current traffic-related air pollution in adult European populations.
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is long-term exposure to traffic or ambient air pollution associated with prevalence of cough and phlegm in adult European populations?
What is the bottom line?
-
Current long-term average air pollution levels were not associated with symptoms of chronic bronchitis, cough or phlegm in European adults of all ages living in nine European countries, but there were small increases in reported phlegm in never-smokers associated with coarse particulate matter.
Why read on?
-
This is one of the largest such studies in adults involving >10 000 individuals in five European cohorts using harmonised exposure and outcome measurements; while most results were null, there was some heterogeneity across findings for cohort assessments at different time points, particularly for black carbon and NO2.
Introduction
Chronic cough and phlegm production are common respiratory symptoms. In the past, these were often considered together as the clinical phenotype of chronic bronchitis,1 but more recently phlegm2 and cough3 have been considered separately and may have differing mechanisms—for example, cough may result from central reflex sensitivity4 as well as irritation and inflammation. A previous study of young adults found wide geographic variability in chronic bronchitis prevalence (0.7–9.7%) across Europe, but only 30% of the variability could be explained by differences in smoking habits.5 This suggests other potentially modifiable factors—such as air pollution—may be important.
There is good evidence that air pollution triggers exacerbations in patients with COPD, and suggestive evidence of chronic effects of air pollution on the prevalence and incidence of COPD in adults.6 Concurrent asthma may give rise to cough and phlegm. Traffic-related air pollution has also been related to onset of childhood asthma, but findings in adults are less clear.7 Pathophysiological studies have found associations between long-term exposure to ambient particulate matter (PM) and chronic mucosal inflammation in the lung,8 resulting in excessive mucus secretion, coughing and phlegm production.9 Previous epidemiological studies examining associations between objectively measured air pollution and chronic bronchitis symptoms in adults10–27 are difficult to compare. For example, some studies have used surrogate measures for air pollution (eg, distance from the main road,13 ,20 ,21 ,27 traffic intensity17), others used air pollution data from local monitoring networks10–13 ,16 ,22 ,23 ,25 ,26 or model-derived exposures estimated at home address.15 ,17 ,19 ,24 Some13 ,15 ,17 but not all14 ,18 ,19 ,23 studies reported increased risks in the general population, whereas studies in specific populations reported associations only in never-smokers10–12 ,16 ,26 or females.20 ,21 ,25
The present study investigates cross-sectional associations between ambient air pollution estimated at home address and prevalence of chronic bronchitis symptoms in five European cohort studies participating in European Study of Cohorts for Air Pollution Effects (ESCAPE) project. Taking advantage of individual information and repeated assessments, we gave special attention to the time period of exposure (contemporary, historic 2000s and historic 1990s exposures) in repeated cross-sectional analyses and conducted extensive sensitivity analyses.
Methods
Study populations
Analyses were based on subpopulations from the European Community Respiratory Health Survey (ECRHS); National Survey of Health and Development (NSHD) from the UK; the Study on the influence of Air pollution on Lung function, Inflammation and Aging (SALIA) from Ruhr area in Germany; the Swiss cohort study on Air Pollution And Lung and heart Diseases in Adults (SAPALDIA); and the French Asthma-E3N study, an asthma case–control study nested in the ‘Etude Épidémiologique de Femmes de la Mutuelle Générale de l’Education Nationale (E3N)’ cohort who were living in geographic areas covered by ESCAPE exposure models (‘ESCAPE areas’). A brief description of each cohort is available in online supplements-1. Those included in the analyses had valid chronic bronchitis data and information on sex, age, smoking status, season of questionnaire interview, education. The NSHD, SALIA and SAPALDIA contributed information from two assessment rounds. Ethical approvals for analyses were obtained for all cohorts.
Outcome definition
Chronic bronchitis symptoms were assessed by questionnaire in all cohorts using standard questions based on those defined by the British Medical Research Council (MRC) in 1965,1 as reported cough and phlegm production first thing in the morning and/or during the day or at night for 3 months of the year for ≥2 years. Other outcomes investigated were chronic cough (reported cough for 3 months for ≥2 years regardless of reported phlegm or not) and chronic phlegm (reported phlegm for 3 months for ≥2 years regardless of reported cough or not), except for SALIA, where questions regarding phlegm production were not asked separately from cough, therefore it was not possible to derive the outcome of ‘chronic phlegm’ (online supplements-2).
Exposure measurements
ESCAPE-period exposures
The ESCAPE exposure assessments have been described elsewhere.28 ,29 Briefly, a standardised protocol was applied in all geographic sites within the ESCAPE areas during October 2008 to April 2011. Nitrogen dioxide (NO2) and nitrogen oxides (NOx) measurements were conducted in 36 ESCAPE study areas while PM (PM10, PM with aerodynamic diameter ≤10 µm and PM2.5, PM with aerodynamic diameter ≤2.5 µm) were measured in 20 ESCAPE study areas, both in a 14-day period of each of three seasons (cold, warm and intermediate). Annual average concentrations for each monitoring site were calculated by combining the three 14-day periods with measurement data from a centrally located reference site, in operation during the whole study period, to adjust for temporal variability. The land-use regression (LUR) model developed used geographic information system (GIS)-derived predictor variables to describe spatial variation of annual average concentrations for each study area at measurement locations. An annual average estimate was then assigned from the LUR models to each geocoded address (place of residence) based on the date of questionnaire assessment for study participants. In addition, two indicators of local exposures to traffic were derived for each participant's address: traffic intensity on the nearest road (traffic intensity, vehicles/day) and total traffic load on major roads in a 100 m buffer (traffic load, vehicles*m/day).
Each participant was assigned an annual average concentration at home outdoor of NO2, NOx and the background levels of NO2. For participants residing within ESCAPE areas with PM measurements, they were also assigned exposures to PM2.5, PM10, the coarse fraction of PM (PMcoarse as PM10 minus PM2.5) and PM2.5abs, the light absorbance of PM2.5 (similar to ‘black carbon’).
Back-extrapolation
Questionnaire assessments in some cohorts occurred prior to the ESCAPE monitoring campaign in 2008–2011, with some up to 25 years earlier. Due to changes (usually decreases) in air pollution over time, ESCAPE-period exposure values were back-extrapolated to the years of collection of health data assuming proportional changes in within-city spatial patterns. Here, individually assigned estimates of ambient concentrations were adjusted (calibrated) for the long-term trends using a predefined back-extrapolation algorithm (see http://www.escapeproject.eu/manuals/Procedure_for_extrapolation_back_in_time.pdf; accessed 10 May 2014).
Back-extrapolation for NO2 and PM10 was conducted by ratio methods to the most recent follow-up years in ECRHS and SAPALDIA (assessments in 1998–2002 and 2002, respectively) and also to earlier assessment in SALIA in 1985–1994, NSHD in 1999 and SAPALDIA in 1991.
Statistical analyses
Each cohort was first analysed separately using centrally written analytic codes, and harmonised outcome and confounder variables. Descriptive analyses were conducted including Spearman correlation coefficients. The analytic strategy, including all models, sensitivity and subgroup analyses, was specified a priori, based on current knowledge. Cross-sectional analyses using logistic regression models were undertaken to obtain cohort-specific ORs. Results were then combined using both fixed effects and random effects meta-analyses; pooled estimates from the latter were only shown when heterogeneity (p<0.05) existed across cohorts.
The main analyses used ‘ESCAPE-period exposure’ for 2008–2011 applied to the most recent assessment within 10 years of exposure models in all five cohorts (earliest ECRHS and SAPALDIA with assessments in 2002).
A sequence of nested models were run for each outcome: model 1—unadjusted crude model; model 2—adjustments of age and sex; model 3 (main model)—further adjusted for smoking, education level and interview season, all uniformly defined in all cohorts. Model 4 was further adjusted for environmental tobacco smoking (ETS) exposures at home and/or at work and occupational exposures to any of vapours/gases/dusts/fumes (VGDF); availability and definition of these differed across cohorts. Model 5 was a study-specific model further adjusted for smoking pack years and locally defined neighbourhood-level socioeconomic status. All traffic indicator models were adjusted for the background NO2 (NO2 not directly influenced by traffic) to better estimate near traffic effects.
In main analyses, based on model 3 using ESCAPE-period exposures, cohort-specific sensitivity analyses were conducted (i) on the following potentially sensitive subgroups: females, asthmatics, those aged ≥50 years and never-smokers; (ii) excluding those with COPD and/or asthma.
All cohort-specific results from model 3 (or where appropriate, related subgroup and/or sensitivity analyses), were then combined using both fixed effects and random effect meta-analyses by the Stata metan command; pooled estimates from the latter were only shown when heterogeneity (p<0.05) existed across cohorts. Results presented/used in the meta-analyses for multicountry study ECRHS were from random effect models with city modelled as a random effect while the other four were from fixed effect models with country/area modelled as a fixed effect.
Further sensitivity analyses were conducted to address issues relating to cohort heterogeneity and exposure estimation. In main analyses, based on model 3 using ESCAPE-period exposures, cohort heterogeneity was investigated in leave-one-out meta-analyses, where each cohort was dropped in turn. To investigate exposure issues, we (i) conducted meta-analyses excluding centres with poorer exposure model validation statistics (R2<0.6); (ii) restricted analyses to non-movers (those who did not move between the most recent and previous assessment, which were at least 8 years apart); (iii) conducted analyses using ‘contemporary exposure estimates’; these used ESCAPE 2008–2011 estimates for Asthma-E3N (2011), NSHD (2008) and SALIA (2006/2010), that is, excluding SAPALDIA and ECHRHS where questionnaire assessments were >6 years prior to exposure estimation; (iv) conducted analyses using ‘historic exposure estimates’ back-extrapolated to year of assessment for assessments in 1999–2002 (ECRHS 2002, NSHD 1999, SAPALDIA 2002) and in the early 1990s (SAPALDIA 1991, SALIA 1985–1994), that is, when exposures were higher.
Statistical analyses were performed using Stata V.12.0, Texas, USA. Statistical significance was set at p value <0.05.
Results
For main analyses using ESCAPE-period estimates for the most recent assessment, there were 15 279 participants successfully assigned at least NO2 estimates (table 1) and 10 537 participants assigned at least PM10 estimates (see online supplements-3) with information on variables of main model 3. At the most recent assessment, mean age of the study population ranged from 42.9 years (ECRHS) to 71.5 years (SALIA). Asthma-E3N and SALIA were cohorts of older females only. Current smokers ranged from 5.3% (SALIA) to 32% in the younger general population of ECRHS. Asthma-E3N participants were mainly teachers, and 91.3% were highly educated compared with 11.5% in NSHD. VGDF exposure was 30–40% in the mixed sex general population cohorts (ECRHS, NSHD, SAPALDIA) but lower in the female cohorts. Prevalence of chronic bronchitis ranged from 1.5% (Asthma-E3N) to 6.8% (SALIA) (see online supplements-4).
Description of study population (subpopulations of the original study with individually assigned NO2 measures) of all five cohorts as used at each assessment
Summary statistics of ESCAPE-period air pollutants and traffic indicators are presented in online supplements-5. Mean NO2 ranged from 22 µg/m3 (NSHD) to 31 µg/m3 (Asthma-E3N), whereas mean PM10 ranged from 16 µg/m3 (NSHD) to 27 µg/m3 (SALIA). Within-study contrasts assessed by IQR varied from 8 µg/m3 in SAPALDIA to 20 µg/m3 in ECRHS for NO2 and 2 µg/m3 (NSHD) to 9.2 µg/m3 (ECRHS) for PM10. Exposures back-extrapolated to the 1990s were higher than for estimates at later assessments.
Spearman correlation coefficients between PM and NOx/NO2 metrics were high (r∼0.7–0.8), therefore precluding two pollutant analyses, while correlations between pollutants and traffic measures were low to moderate (r∼0.3–0.5) (see online supplements-6).
ESCAPE-period exposure estimates 2008–2011 were highly correlated (r>0.9) with exposures back-extrapolated to the assessments in 2002 ECRHS and SAPALDIA, justifying the use of ESCAPE-period exposures in main analyses.
Results from analyses using ESCAPE-period exposure estimates
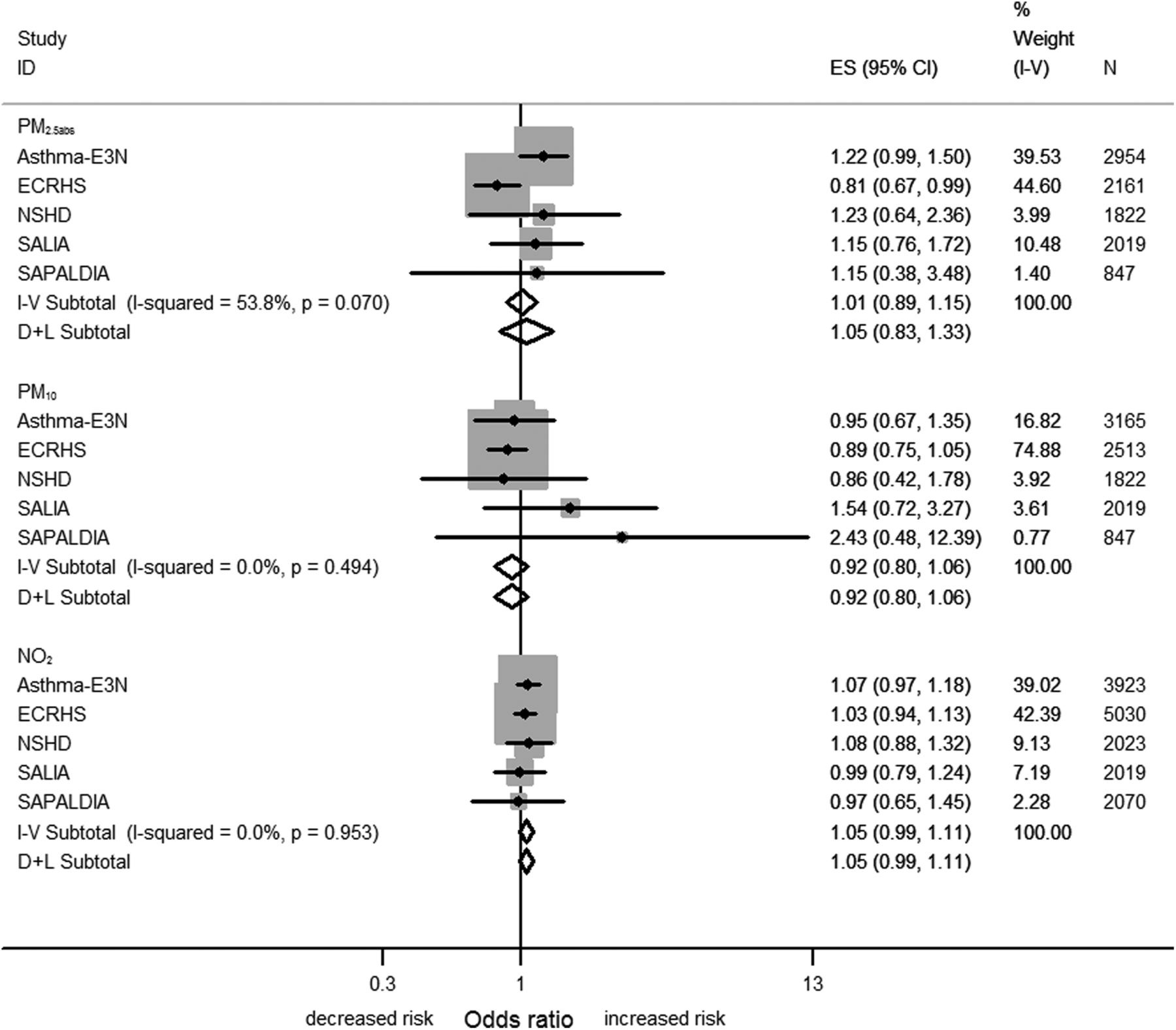
Combined estimates from the meta-analyses using model 3 are displayed in table 2 (see also figure 1 and Forest plots, online supplements-7). No statistically significant overall associations were found between any air pollutant or traffic indicator and any outcome using ESCAPE-period estimates.
Overall populations at the most recent assessment *: fixed-effect meta-analysis results on model 3 (adjusted for age, sex, smoking, education and season of interview) for all air pollutants and traffic indicators for each outcome, using ESCAPE-period (2008–2011) exposures from all five cohorts.

Meta-analysis results on model 3 (adjusted for age, sex, smoking, education, season of questionnaire interview) for NO2 (per 10 µg/m3), PM10 (per 10 µg/m3) and PM2.5abs (per 10−5 m−1) for chronic cough at the most recent assessment using the European Study of Cohorts for Air Pollution Effects (ESCAPE)-period exposures in the overall populations from all five cohorts. I-squared, variation in estimated effect attributable to heterogeneity; I-V, inverse–variance weighted fixed effects method; D-L, DerSimonian-Laird random effects method; ES, effect estimate; PM, particulate matter.
Associations in meta-analyses using main model 3 leaving out one cohort in turn (online supplements-8) or restricted to cohorts with ‘contemporary exposure estimates’: Asthma-E3N (2011), NSHD (2008) and SALIA (2006–2010) (online supplements-9) were all null except for associations between chronic cough and PM2.5abs in analyses not including ECRHS, with OR, 95% CI 1.20 (1.01 to 1.44) per 10−5/m.
Further adjustments in models 4 and 5 did not change the results substantially, although effect estimates were slightly smaller and the 95% CIs became wider (data not shown), which may in part relate to fewer participants.
Sensitive subgroups
In never-smokers, higher and uniformly positive effect estimates for all air pollutants and traffic indicators for all three outcomes were observed (table 3). A statistically significant association was found between chronic phlegm and both PM10 (OR, 95% CI 1.32 (1.02 to 1.71), per 10 µg/m3 increase) and PMcoarse (OR, 95% CI 1.31 (1.05 to 1.64), per 5 µg/m3 increase) (figure 2). In analyses of never-smokers in cohorts with ‘contemporary exposure estimates’ (online supplements-9), associations with chronic phlegm were no longer statistically significant but associations between chronic cough and PM2.5 and PM2.5abs became larger and statistically significant: PM2.5 OR, 95% CI 1.47 (1.02 to 2.12) per 5 µg/m3 increase, PM2.5abs OR, 95% CI 1.30 (1.04 to 1.63) per 10−5/m, although with evidence of heterogeneity for the latter (Phet=0.024). In the random-effects analysis, the PM2.5abs result was not statistically significant: OR, 95% CI 1.58 (0.90 to 2.76) per 10−5/m.
Never-smokers at the most recent assessment*: fixed-effect meta-analysis results on model 3 (adjusted for age, sex, smoking, education and season of interview) for all air pollutants and traffic indicators for each outcome, using ESCAPE-period (2008–2011) exposures from all five cohorts

{kind=link}
{kind=link}
Meta-analysis results on model 3 (adjusted for age, sex, smoking, education, season of questionnaire interview) for PM10 (per 10 µg/m3) and PMcoarse (per 5 µg/m3) for chronic phlegm at the most recent assessment using the European Study of Cohorts for Air Pollution Effects (ESCAPE)-period exposures in the never-smokers populations from four cohorts. I-squared, variation in estimated effect attributable to heterogeneity; I-V, inverse-variance weighted fixed effects method; D-L, DerSimonian-Laird random effects method; PM, particulate matter. The Study on the influence of Air pollution on Lung function, Inflammation and Aging (SALIA) was excluded from the above analysis because questions regarding phlegm production were not asked separately from cough. ES, effect estimate.
There were no statistically significant effect estimates observed in meta-analyses for asthmatics, females, participants aged 50+ years, participants without COPD and/or asthma or non-movers (results not shown).
Exposure-related sensitivity analyses
Sensitivity analyses for NO2 and NOx excluding centres with LUR model validation R2 statistics <0.6 gave similar null results for the main ESCAPE-period analyses (online supplements-10). The R2 statistics were all >0.6 for PM estimates in our study areas.
Using back-extrapolated ‘historic exposure estimates’ to 1999–2002 (table 4), there were consistent but statistically non-significant elevated risks in all populations but not in never-smokers for all three outcomes with NO2 and PM10. Using historic exposure estimates to the early 1990s in only two cohorts (table 5), statistically significant associations were found between NO2 and both chronic bronchitis (OR: 1.10, 95% CI 1.00 to 1.22) and chronic cough (OR: 1.10, 95% CI 1.01 to 1.20).
Back-extrapolated from ESCAPE-period exposures (2008–2011) to early 2000s ‘historic exposure estimates’: fixed-effect meta-analysis on cross-sectional results from ECRHS (2002), NSHD (1999), SAPALDIA (2002): all participants (upper section) and never-smokers (lower section), main model 3.
Back-extrapolated from ESCAPE-period exposures (2008–11) to early 1990s ‘historic exposure estimates’: fixed-effect meta-analysis on cross-sectional results from SALIA (1985–1994), SAPALDIA (1991): all participants (upper section) and never-smokers (lower section), main model 3.
Discussion
This is one of the largest studies to investigate the link between bronchitis symptoms and current air pollution exposures using five cohorts in nine European countries. Main analyses defined a priori did not show significant associations between the period prevalence of chronic bronchitis, cough or phlegm and any of six air pollutant metrics and two traffic indicators. Associations between the particulate measure of black carbon PM2.5abs and chronic cough were statistically significant if leaving out a younger cohort (ECRHS) in analyses of all individuals and of never-smokers. In never-smokers, associations were in general larger and consistently positive, reaching statistical significance between phlegm and PMcoarse (but not PM2.5). The higher NO2 exposures in the early 1990s were associated with chronic bronchitis and cough, but this analysis was only possible for two cohorts.
Findings in comparisons with previous studies
To our knowledge, this is one of the first epidemiological studies to report on long-term associations between the coarse fraction of ambient particles and cough and phlegm in adults. PMcoarse has previously been found to be associated with respiratory hospital admissions30 and to be more potent than fine PM in inducing inflammatory responses in in vitro and in vivo (mouse) studies.31 ,32
We also observed significant associations between PM10 and phlegm in never-smokers but not overall. As in this analysis, cross-sectional associations with chronic bronchitis and with phlegm were seen in never-smokers (but not in former and current smokers) in the SAPALDIA study,26 but no statistically significant associations were seen in SALIA (mainly non-smokers)23 while continuous measures of PM10 were not associated with cough in older adults in France.15 However, longitudinal analyses in both SALIA22 and SAPALDIA24 studies suggested declines in PM10 are associated with declines in cough and chronic bronchitis symptoms; additionally, an analysis of Seventh Day Adventist non-smokers found associations between chronic cough and 15-year cumulative PM10 exposures.10
We saw no significant associations overall with PM2.5. This is consistent with previous cross-sectional epidemiological studies in adults in the USA19 and a 2006 analysis of the ECRHS25 cohort and with a longitudinal analysis in Melbourne14 but not an analysis in non-smoking Seventh Day Adventists, which found associations between 20-year cumulative exposure to PM2.5 and chronic bronchitis.11 We did observe associations between chronic cough and PM2.5abs, a measure of black carbon or soot, in some sensitivity analyses, but these were not consistent and may represent chance findings.
Lack of findings of significant associations with NO2, except for chronic cough and chronic bronchitis in SALIA and SAPALDIA in the 1990s when exposures were higher are partially consistent with previous studies. Significant associations were seen with cough, but not chronic bronchitis in a previous analysis of SALIA23; with chronic bronchitis and with phlegm in women but not men in the ECRHS (cough was not considered)25; with phlegm (but not cough) in women but not men in an older French cohort15; and with chronic bronchitis and chronic phlegm in never-smokers in SAPALDIA.26 Chronic bronchitis symptoms were not associated with low levels of cumulative NO2 exposure in non-smoking Californians.16
We are aware of only one adult study that has considered NOx and contrary to our null findings, exposures >19 vs 0–8 µg/m3 in southern Sweden were associated with higher prevalences of chronic bronchitis.17
We found no significant associations of traffic intensity with any chronic bronchitis symptoms, contrary to six previous studies using differing traffic intensity metrics based on traffic counts17 ,23 and distance from road.13 ,20 ,21 ,27
ORs using ESCAPE exposure estimates in individual cohorts were comparable with those from previously published analyses using cohort-specific air pollution estimates, allowing for differences in study design (see online supplements-11 for details).
Most10–13 15–17 19–21 ,23 ,25–27 but not all14 ,18 ,22 ,24 previous studies examining associations between air pollutant metrics and chronic bronchitis in adults have conducted cross-sectional analyses. We did not do a longitudinal analysis because symptoms come and go over time and they do not represent a stable chronic condition. Also, questionnaire-based reporting is most likely to capture symptoms experienced in the last few months, therefore reflecting cumulative prevalence of acute and subacute effects.
Strengths and weaknesses of the study
Strengths of this study are the use of five large existing cohorts in different parts of Europe, centrally defined harmonised variables for each cohort, standard assessment of exposures to eight traffic-related exposures individually assigned to home address and an identical prespecified statistical protocol. However, there were also several limitations. First, uncertainty in exposure estimates might have introduced non-systematic errors, reducing the power of the study to detect effects. However, analyses excluding models with spatial variation R2 <0.6 did not substantially change the results (online supplements-10 and supplements-12) Second, exposure assessments for ESCAPE occurred years after questionnaire assessments in some cohorts. This was investigated using back-extrapolated exposure assessments aligned with questionnaire. Back-extrapolation assumes within-city spatial contrasts of air pollutants remain similar over long periods of time, for which there is some support from previous studies.33 ,34 Third, harmonised information on confounders was limited. Fourth, there might be reporting bias, particularly reluctance to report phlegm in females.35 Fifth, we conducted many statistical analyses and it is possible that observed associations were due to chance. Sixth, the cohorts were heterogeneous in both design and populations, which may have resulted in systematic differences between studies. To address this, we used harmonised variables, explored potential effect modifiers, used meta-analyses not pooled analyses and conducted leave-one-out sensitivity meta-analyses. Finally, we note that detecting effects in potentially susceptible subgroups, of relevance to environmental policy, may require much larger sample sizes than possible here.
In conclusion, although deleterious effects of ambient air pollution on a range of health outcomes including mortality are well documented, we did not find evidence for significant associations between current long-term average air pollution levels and symptoms of chronic bronchitis, cough or phlegm in >10 000 European adults. Our study findings, based on very large-scale harmonised population-based cohort studies using a priori specified analyses, contribute to strengthening the evidence-based studies for policy formulation.
Acknowledgments
We thank all study members and staff involved in data collections in each cohort.
E3N We wish to thank all the women from the E3N study. We also thank Lyan Hoang, Maryvonne Niravong and Marie Fangon for invaluable assistance with the implementation of the study.
ECRHS The ECRHS data incorporated in this analysis would not have been available without the collaboration of the following individuals and their research teams.
ECRHS Co-ordinating centre: P Burney, D Jarvis, S Chinn, J Knox (ECRHS II), C Luczynska+, J Potts.
Steering Committee for ECRHS II: P Burney, D Jarvis, S Chinn, J. M. Anto, I. Cerveri, R. deMarco , T. Gislason, J. Heinrich, C. Janson, N. Kunzli, B. Leynaert, F. Neukirch, T. Rochat, J. Schouten, J. Sunyer; C. Svanes, P. Vermeire+, M. Wjst.
Principal Investigators and Senior Scientific Teams for ECRHS II: Australia: Melbourne (M Abramson, R Woods, EH Walters, F Thien), Belgium: South Antwerp & Antwerp City (P Vermeire+, J Weyler, M Van Sprundel, V Nelen), Denmark: Aarhus (EJ Jensen), Estonia: Tartu (R Jogi, A Soon), France: Paris (F Neukirch, B Leynaert, R Liard, M Zureik), Grenoble (I Pin, J Ferran-Quentin), Bordeaux (A Taytard, C Raherison), Montpellier (J Bousquet, P Demoly) Germany: Erfurt (J Heinrich, M Wjst, C Frye, I Meyer) Hamburg (K Richter), Iceland: Reykjavik (T Gislason, E Bjornsson, D Gislason, T Blondal, A Karlsdottir), Italy: Turin (M Bugiani, P Picci oni, E Caria, A Carosso, E Migliore, G Castiglioni), Verona (R de Marco, G Ver lato, E Zanolin, S Accordini, A Poli, V Lo Cascio, M Ferrari), Pavia (A Marinoni, S Villani, M Ponzio, F Frigerio, M Comelli, M Grassi, I Cerveri, A Corsico), Netherlands: Groningen & Geleen (J Schouten, M Kerkhof), Norway: Bergen (A Gulsvik, E Omenaas, C Svanes, B Laerum), Spain: Barcelona (JM Anto, J Sunyer, M Kogevinas, JP Zock, X Basagana, A Jaen, F Burgos), Huelva (J Maldonado, A Pereira, JL Sanchez), Albacete (J Martinez-Moratalla Rovira, E Almar), Galdakao (N Muniozguren, I Urritia), Oviedo (F Payo), Sweden: Uppsala (C Janson, G Boman, D Norback, M Gunnbjornsdottir), Goteborg (K Toren, L Lillienberg, AC Olin, B Balder, A Pfeifer-Nilsson, R Sundberg), Umea (E Norrman, M Soderberg, K Franklin, B Lundback, B Forsberg, L Nystrom), Switzerland: Basel (N Kunzli, B Dibbert, M Hazenkamp, M Brutsche, U Ackermann-Liebrich); UK: Norwich (D Jarvis, B Harrison), Ipswich (D Jarvis, R Hall, D Seaton), USA: Portland (M Osborne, S Buist, W Vollmer, L Johnson).
†Deceased
NHSD We acknowledge the NSHD participants and the NSHD scientific and data collection teams.
SALIA During the last decades, a lot of scientists, study nurses and laboratories were involved in conducting the study. As representatives for all these people, we would like to thank especially Reinhard Dolgner (MD) for organizing the baseline study and Barbara Schulten as study nurse for her help in organizing the follow-up study. We are most grateful for all the women from the Ruhr area and from Borken who participated in the study during decades.
SAPALDIA Study directorate: T Rochat (p), NM Probst Hensch (e/g), JM Gaspoz (c), N Künzli (e/exp), C Schindler(s).
Scientific team: JC Barthélémy (c), W Berger (g), R Bettschart (p), A Bircher (a), G Bolognini (p), O Brändli (p), C Brombach (n), M Brutsche (p), L Burdet (p), M Frey (p), U Frey (pd), MW Gerbase (p), D Gold (e/c/p), E de Groot (c), W Karrer (p), R Keller (p), B Knöpfli (p), B Martin (pa), D Miedinger (o), U Neu (exp), L Nicod (p), M Pons (p), F Roche (c), T Rothe (p), E Russi (p), P Schmid-Grendelmeyer (a), A Schmidt-Trucksäss (pa), A Turk (p), J Schwartz (e), D. Stolz (p), P Straehl (exp), JM Tschopp (p), A von Eckardstein (cc), E Zemp Stutz (e).
Scientific team at coordinating centres: M Adam (e/g), E Boes (g), PO Bridevaux (p), D Carballo (c), E Corradi (e), I Curjuric (e), J Dratva (e), A Di Pasquale (s), L Grize (s), D Keidel (s), S Kriemler (pa), A Kumar (g), M Imboden (g), N Maire (s), A Mehta (e), F Meier (e), H Phuleria (exp), E Schaffner (s), GA Thun (g) A Ineichen (exp), M Ragettli (e), M Ritter (exp), T Schikowski (e), G Stern (pd), M Tarantino (s), M Tsai (e), M Wanner (pa)
(a) allergology, (c) cardiology, (cc) clinical chemistry, (e) epidemiology, (exp) exposure, (g) genetic and molecular biology, (m) meteorology, (n) nutrition, (o) occupational health, (p) pneumology, (pa) physical activity, (pd) paediatrics, (s) statistics
The study could not have been done without the help of the study participants, technical and administrative support and the medical teams and field workers at the local study sites.
Local fieldworkers: Aarau: S Brun, G Giger, M Sperisen, M Stahel, Basel: C Bürli, C Dahler, N Oertli, I Harreh, F Karrer, G Novicic, N Wyttenbacher, Davos: A Saner, P Senn, R Winzeler, Geneva: F Bonfils, B Blicharz, C Landolt, J Rochat, Lugano: S Boccia, E Gehrig, MT Mandia, G Solari, B Viscardi, Montana: AP Bieri, C Darioly, M Maire, Payerne: F Ding, P Danieli A Vonnez, Wald: D Bodmer, E Hochstrasser, R Kunz, C Meier, J Rakic, U Schafroth, A Walder.
Administrative staff: C Gabriel, R Gutknecht.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
YC, TS and MA contributed equally to this work.
TS, FK UK, JS, NK, NP-H and ALH: Steering Committee ESCAPE Work Package 4 Respiratory Health in Adults.
↵†Deceased.
-
Contributors Conceptualised the study: ALH, YC, ZA-K, MA and the Steering Committee of ESCAPE WP4: NP-H, FK, UK, TS, JS, NK (Chair). Drafted and edited the paper: YC, ALH, TS, NK. Discussed and interpreted the findings: ESCAPE WP4 working group: MA, AB, A-EC, YC, ALH, NP-H, BJ, FK, NK, UK, AM, JS, MS, TS, AV. Cohort data collections: MB, FC-C, BF, MWG, JH, NP-H, RH, DJ, FK, DKuh, NK, UK, TR, CS, JS, ST, AV, RV. Air pollution assessments: RB, BB, MC, AdN, CD, KdH, REDS, VVF, GH, MJN, AR, MSR, DS, MT. Statistical analysis: ZAK, MA, AB, A-EC, YC, BJ, DKei, AM, CS, MS, TS, AV. All authors have revised the paper and approved the final version.
-
Funding The research leading to these results has received funding from the European Community's Seventh Framework Program (FP7/2007-2011) under grant agreement number: 211250.
-
E3N cohort is being studied with the financial support of the Mutuelle générale de l’éducation nationale, the European Community, the Ligue nationale contre le cancer, the Institut Gustave–Roussy, INSERM, and a grant from the World Cancer Research Fund (grant no. 2007/14). The Asthma-E3N study was supported by the Fonds de dotation 'Recherche en Santé Respiratoire'.
-
ECRHS was supported by the European Commission, as part of their Quality of Life programme.
-
The coordination of ECRHS II was supported by the European Commission, as part of their Quality of Life programme. The following bodies funded the local studies in ECRHS II in this article.
-
Albacete—Fondo de Investigaciones Santarias (grant code: 97/0035-01, 13 99/0034-01, and 99/0034-02), Hospital Universitario de Albacete, Consejeria de Sanidad. Antwerp—FWO (Fund for Scientific Research)—Flanders Belgium (grant code: G.0402.00), University of Antwerp, Flemish Health Ministry.
-
Barcelona—Fondo de Investigaciones Sanitarias (grant code: 99/0034-01, and 99/0034-02), Red Respira (RTIC 03/11 ISC IIF). Ciber of Epidemiology and Public Health has been established and founded by Instituto de Salud Carlos III.
-
Erfurt—GSF–National Research Centre for Environment & Health, Deutsche Forschungsgemeinschaft (DFG) (grant code FR 1526/1-1), funded by Helmholtz Zentrum Munich and grants from the German Research Foundation (HE3294/10-1).
-
Galdakao—Basque Health Department.
-
Grenoble—Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no.
-
2610, Ministry of Health, Direction de la Recherche Clinique, Ministere de l'Emploi et de la Solidarite, Direction Generale de la Sante, CHU de Grenoble, Comite des Maladies Respiratoires de l'Isere.
-
Ipswich and Norwich—National Asthma Campaign (UK).
-
Huelva—Fondo de Investigaciones Sanitarias (FIS) (grant code: 97/0035-01, 99/0034-01, and 99/0034-02).
-
Oviedo—Fondo de Investigaciones Santarias (FIS) (grant code: 97/0035-01, 99/0034-01, and 99/0034-02).
-
Paris—Ministere de l'Emploi et de la Solidarite, Direction Generale de la Sante, UCBPharma (France), Aventis (France), Glaxo France, Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, CHU de Grenoble.
-
Pavia—Glaxo, Smith & Kline Italy, Italian Ministry of University and Scientific and Technological Research (MURST), Local University Funding for Research 1998 & 1999 (Pavia, Italy).
-
Turin—ASL 4 Regione Piemonte (Italy), AO CTO/ICORMA Regione Piemonte (Italy), Ministero dell'Università e della Ricerca Scientifica (Italy), Glaxo Wellcome spa (Verona, Italy).
-
Umeå—Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Västerbotten County Council (ALF).
-
Verona—University of Verona; Italian Ministry of University and Scientific and Technological Research (MURST); Glaxo, Smith & Kline Italy.
-
NSHD, the National Survey of Health and Development was funded by the UK Medical Research Council (MRC). The NSHD and Professors Hardy and Kuh are supported by core funding and grant funding (MC_UU_12019/1, MC_UU_12019/2, MC_UU_12019/4) from the UK Medical Research Council.
-
SALIA received funds from the German state (NRW) and federal Ministries of the Environment. The follow-up investigation was funded by the DGUV (German statutory accident assurance) VT 266.1.
-
SAPALDIA received funds from the Swiss National Science Foundation (grants no 33CSCO-134276/1, 33CSCO-108796, 3247BO-104283, 3247BO-104288, 3247BO-104284, 3247-065896, 3100-059302, 3200-052720, 3200-042532, 4026-028099), the Federal Office for Forest, Environment and Landscape and several Federal and Cantonal authorities; The Swiss National Science Foundation and German research Foundation D-A-CH grant no 32473BM-133148.
-
Measurements and models for PM in Grenoble (ECRHS) were funded by Region Rhônes-Alpes.
-
Ethics approval Ethical approval was obtained for each of five participating cohorts in this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The ESCAPE air pollution data are available for use in future research projects on application to the ESCAPE steering committee (PI Burt Brunekreef).