Article Text

Abstract
Objectives Hydrogen sulfide (H2S) is a gas produced by respiratory cells including smooth muscle cells and may play a role as a cellular gasotransmitter. We evaluated whether H2S levels in serum or sputum could represent a new biomarker of COPD in a cross-sectional study.
Methods H2S levels in sputum and serum samples were measured using a sulfide-sensitive electrode in 64 patients with stable COPD (S-COPD), 29 COPD subjects during acute exacerbation (AE-COPD), 14 healthy smokers and 21 healthy non-smokers.
Results Sputum H2S levels in AE-COPD subjects were higher than those in S-COPD, healthy smoking and non-smoking subjects (p<0.001), but serum H2S levels in AE-COPD were lower than those in S-COPD (p<0.001). Thus, the sputum-to-serum ratio of H2S (H2S ratio) in AE-COPD subjects were higher than those in stable COPD, healthy smoking and non-smoking subjects (p<0.001). In 14 COPD subjects whose H2S ratios were measured during and after an exacerbation, the mean ratio was increased during exacerbation (p<0.05). H2S ratio was positively correlated with St. George's Respiratory Questionnaire score, sputum neutrophils and IL-6 and IL-8 levels in sputum and serum (p<0.01) but inversely correlated with sputum macrophages (%), FEV1%predicted and FEV1/FVC (p<0.01). The cut-off level of H2S ratio to indicate an exacerbation was ≥0.44 (sensitivity of 93.1% and specificity of 84.5%).
Conclusions The ratio of sputum-to-serum levels of H2S may provide a useful marker of COPD indicative of obstructive neutrophilic inflammation and of potential ongoing exacerbation.
- COPD Exacerbations
Statistics from Altmetric.com
Key messages
What is the key question?
-
We evaluated whether H2S levels in serum or sputum could represent a new biomarker of COPD.
What is the bottom line?
-
We found that the ratio of sputum-to-serum levels of H2S may provide a useful marker of COPD indicative of obstructive neutrophilic inflammation and of potential future risk of exacerbation.
Why read on?
-
Concomitant measurement of H2S in sputum and in serum represents a novel promising biomarker of COPD.
Introduction
COPD is one of the major causes of morbidity and mortality, likely to become the third global cause by 2020.1 COPD is characterised by persistent progressive airflow limitation and chronic pulmonary inflammation.2 Exacerbations of COPD characterised by worsening of respiratory symptoms are commonly observed in more severe disease and have been linked to lung function decline, cardiovascular events and death,3 ,4 and with increased pulmonary and extrapulmonary inflammation.5–8 Systemic inflammation may be a key link between COPD and comorbidities, possibly resulting from a spillover from the lung into the systemic circulation.9 ,10
Hydrogen sulfide (H2S), a gas with a typical malodorous smell, is produced by many cell types in the lungs including pulmonary arterial and airway smooth muscle cells, primary fibroblasts and endothelial cells11–13 through the action of three enzymes, namely, cystathionine-γ-lyase (CSE), cystathionine-β-synthase (CBS) and 3-mercaptopyruvate sulfur transferase.14 H2S is the third gasotransmitter along with nitric oxide (NO) and carbon monoxide (CO), with vasodilator and neurotransmitter properties.15 H2S may also be involved in anti-inflammatory processes and has been reported to reduce cigarette smoke-induced lung inflammation in mice.16 It also has reducing properties and can scavenge various oxidising and nitrative species such as superoxide and peroxynitrite.17 In vivo, H2S prevented endothelial disruption and lung vascular leakage induced by particulate air pollution through scavenging reactive oxygen species.18
H2S levels in the lung as well as in serum have been assayed in asthma and COPD. In COPD, higher levels of serum H2S have been reported compared with healthy non-smokers (HNS), with lower levels during an acute exacerbation.19 In asthma, H2S levels in both sputum and serum were strongly correlated with obstructive neutrophilic airway inflammation.20 Therefore, H2S could be considered as a potential biomarker of chronic airway diseases.21 The aims of our study were (i) to measure sputum and serum H2S levels in patients with COPD during a stable period and during an exacerbation, and (ii) to examine their relationships to key markers of disease activity and neutrophilic inflammation. In addition, we evaluated whether sputum and serum levels of H2S could indicate an ongoing exacerbation.
Methods
Subjects
In total, 64 subjects with stable COPD (S-COPD) and 29 subjects with acute exacerbation of COPD (AE-COPD) were recruited from the clinics of the Royal Brompton and Royal Free Hospitals in London. Fourteen healthy smokers (HS) and 21 HNS were recruited from advertisement (table 1). The diagnosis of COPD was made according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines.22 Briefly, COPD subjects had a history of chronic respiratory symptoms (ie, dyspnoea, coughing, sputum or both), a smoking history of >10 pack-years and a postbronchodilator FEV1/FVC ratio <70%. COPD subjects were categorised as severe (stages III and IV) or non-severe (stages I and II). Subjects with concomitant respiratory diseases other than COPD were excluded. HS (≥10 pack-years) and HNS (≤5 pack-years) had normal lung function, no bronchial hyperresponsiveness and no history of pulmonary disease. All participants gave informed consent to a protocol approved by the Ethics Committee.
Characteristics, lung function and treatment of cohorts
COPD exacerbation
An acute exacerbation was defined as new or increased respiratory symptoms for two or more consecutive days, with at least one major symptom (dyspnoea and sputum production) with either another major or minor symptom (wheeze, cold, sore throat and cough). All exacerbation visits occurred within 7 days after its onset. A stable state was defined as having no symptoms related to exacerbation for the preceding 6 weeks.23
Study design
This was a cross-sectional observational study. Health status was assessed with the Medical Research Council (MRC) dyspnoea scale24 and the St. George's Respiratory Questionnaire (SGRQ).25 Lung function tests, 6 minute walk test (6MWT) and sputum and peripheral blood samplings were performed. In 14 COPD subjects, H2S levels in sputum and serum were obtained during an exacerbation and during the stable state.
Sputum induction and processing
Sputum induction was performed with inhaled nebulised 4.5% NaCl solution.26 Sputum plugs were harvested and processed with 0.1% dithiothreitol (DTT) and sulfide antioxidant buffer added to sputum supernatant and stored at −80 °C. Cytospins were prepared for differential cell counts.
Measurement of H2S
H2S concentrations in serum and sputum were measured using a sulfide-sensitive electrode (Model 9616; Orion Research; Beverly, Massachusetts, USA). Briefly, standard solutions were made using 0.1% DTT plus phosphate-buffered saline or distilled water for sputum and serum H2S measurement respectively in order to minimise any effect of DTT. The electrode was placed into the standard solutions for measurement of H2S levels and the calibration standard curve constructed. Validation of H2S measurements including accuracy, reproducibility and storage effects of samples has been reported.20
Measurement of IL-6 and IL-8
IL-6 and IL-8 in serum and sputum supernatants were measured using a commercially available sandwich ELISA kit (R&D Systems, Minneapolis, Minnesota, USA).
Statistical analysis
The main outcome predictor was H2S levels in sputum and serum, or the ratio of sputum to serum H2S levels. At least 14 subjects were needed per group for a 70% power to detect a 20% difference in H2S levels between each group with a two-sided α of 0.05.
Data are shown as mean and SD for normally distributed variables, and median and IQR for non-normally distributed variables. Comparisons of continuous variables between groups were made using Kruskall–Wallis and Mann–Whitney U test with Bonferroni correction. χ2 or Fisher's exact test was used for the comparison of categorical data. Differences of paired samples in the same subjects were analysed by Wilcoxon matched-pairs signed rank test. Linear regression modelling was used to evaluate the simple and joint associations of H2S levels in sputum and serum with parameters that were relevant to COPD, adjusting for age, sex, height, weight and smoking status. Then, multiple linear regression analysis, using a forward stepwise selection, was conducted to determine the independent association of H2S levels with parameters with p value <0.05 obtained from regression modelling. Finally, receiver operating characteristic (ROC) curve was constructed to determine the predictive value of the sputum-to-serum H2S ratio for an exacerbation. A two-tailed p value <0.05 was considered significant.
Results
Characteristics of participants
Forty-one (64.0%) in S-COPD group and 16 (55.2%) in AE-COPD group had mild-to-moderate COPD. SpO2 at rest, FEV1, FVC, FEV1/FVC ratio and sputum macrophages in COPD subjects were lower than in healthy subjects (p<0.05). The 6MWT distance in S-COPD subjects was also shorter (p<0.05). Total SGRQ score and neutrophils in blood and sputum in S-COPD and AE-COPD subjects were higher than those of HNS (p<0.05).
H2S levels in sputum and serum
H2S levels in induced sputum from S-COPD (31.9±15.0 μM) were higher than those from HNS (12.1±6.64 μM; p<0.001). In addition, sputum H2S levels in AE-COPD subjects (50.4±24.4 μM) were much higher than those from S-COPD, HS and HNS subjects (31.9±15.0, 12.1±6.64, 19.7±7.98 μM, respectively; p<0.001) (figure 1A). The concomitant serum H2S levels in S-COPD (148.9±77.6 μM) were also higher than those from HNS and HS (91.0±62.2, 90.6±52.7 μM, respectively; p<0.05). However, unlike the sputum H2S levels, the concomitant serum H2S levels in AE-COPD (48.9±25.5 μM) were much lower compared with those in S-COPD (figure 1B). There was no difference in H2S levels between non-severe and severe COPD subjects during both stable and exacerbated states (see online supplementary figure E1).

H2S levels in sputum (A) and serum (B) from stable COPD subjects (S-COPD:Δ), COPD subjects with acute exacerbation (AE-COPD:▾), healthy smoking (HS:□), and non-smoking subjects (HNS:◯). Horizontal bars indicate mean. ***p≤0.001.
Relationships between H2S levels and COPD parameters
Table 2 shows the correlations between sputum H2S, serum H2S levels and clinically relevant parameters in S-COPD. Both sputum and serum H2S levels positively correlated with MRC scores, total SGRQ scores, sputum neutrophils and serum IL-8 levels (p<0.01). Sputum H2S levels, but not serum H2S levels, showed positive correlations with sputum IL-8 and sputum IL-6 levels (p<0.01). In addition, there were negative correlations between sputum as well as serum H2S levels and SpO2 at rest, 6MWT distance, FEV1%predicted, FEV1/FVC, and sputum macrophages (p<0.01). Sputum H2S levels, but not serum H2S, were negatively correlated to transfer factor of the lung for carbon monoxide (TLCO) and carbon monoxide diffusing capacity adjusted for alveolar volume (KCO) (p<0.01). When adjusted for the potential confounding factors (age, sex, height, weight and smoking status), sputum H2S levels were still correlated with 6MWT distance, FEV1%predicted, FEV1/FVC ratio, TLCO, sputum macrophages (%), sputum neutrophils (%) and sputum IL-8 levels. Similarly, serum H2S levels were significantly correlated with FEV1%predicted and FEV1/FVC ratio. For AE-COPD subjects, there was no significant correlation between sputum H2S, serum H2S levels and other COPD-related parameters (data not shown).
Correlation analysis between H2S in sputum and serum and other parameters related to COPD
Using multiple linear regression analysis to determine the independent association with sputum and serum H2S (table 3), sputum H2S was associated with increased sputum neutrophil (%) and sputum IL-8 levels, and decreased FEV1 (% predicted) (p≤0.05), and serum H2S was associated with decreased FEV1 (% predicted) (p=0.03). Sputum and serum H2S were not influenced by age, sex, height, weight and smoking status.
Independent parameters associated with H2S in sputum and serum using multiple linear regression analysis*
Sputum-to-serum H2S ratio
We examined the ratio of sputum-to-serum levels, the ‘H2S ratio’. H2S ratio in AE-COPD (mean 1.42; 95% CI 0.89 to 1.96) was higher than that in S-COPD subjects (mean 0.27; 95% CI 0.22 to 0.32), HNS (mean 0.20; 95% CI 0.11 to 0.28) and HS (mean 0.24; 95% CI 0.17 to 0.31) (p<0.001) subjects (figure 2A). For further confirmation of this difference, paired samples of sputum and serum during exacerbation as well as stable state from 14 COPD subjects were obtained. H2S ratio during exacerbation (mean 1.54; 95% CI 0.58 to 2.49) was increased compared with that during stable state in all 14 participants (mean 0.28, 95% CI 0.19 to 0.36) (figure 2B) (p<0.01).

(A) H2S sputum-to-serum ratio in stable COPD subjects (S-COPD:Δ), COPD subjects with acute exacerbation (AE-COPD:▾), healthy smoking (HS:□) and non-smoking subjects (HNS:◯). Horizontal bars indicate mean. ***p≤0.001. (B) Difference in H2S sputum-to-serum ratio between stable and exacerbation state. At acute exacerbation, H2S ratio increased in comparison with that in stable state. **p≤0.01.
Sputum-to-serum IL-8 and IL-6 ratios
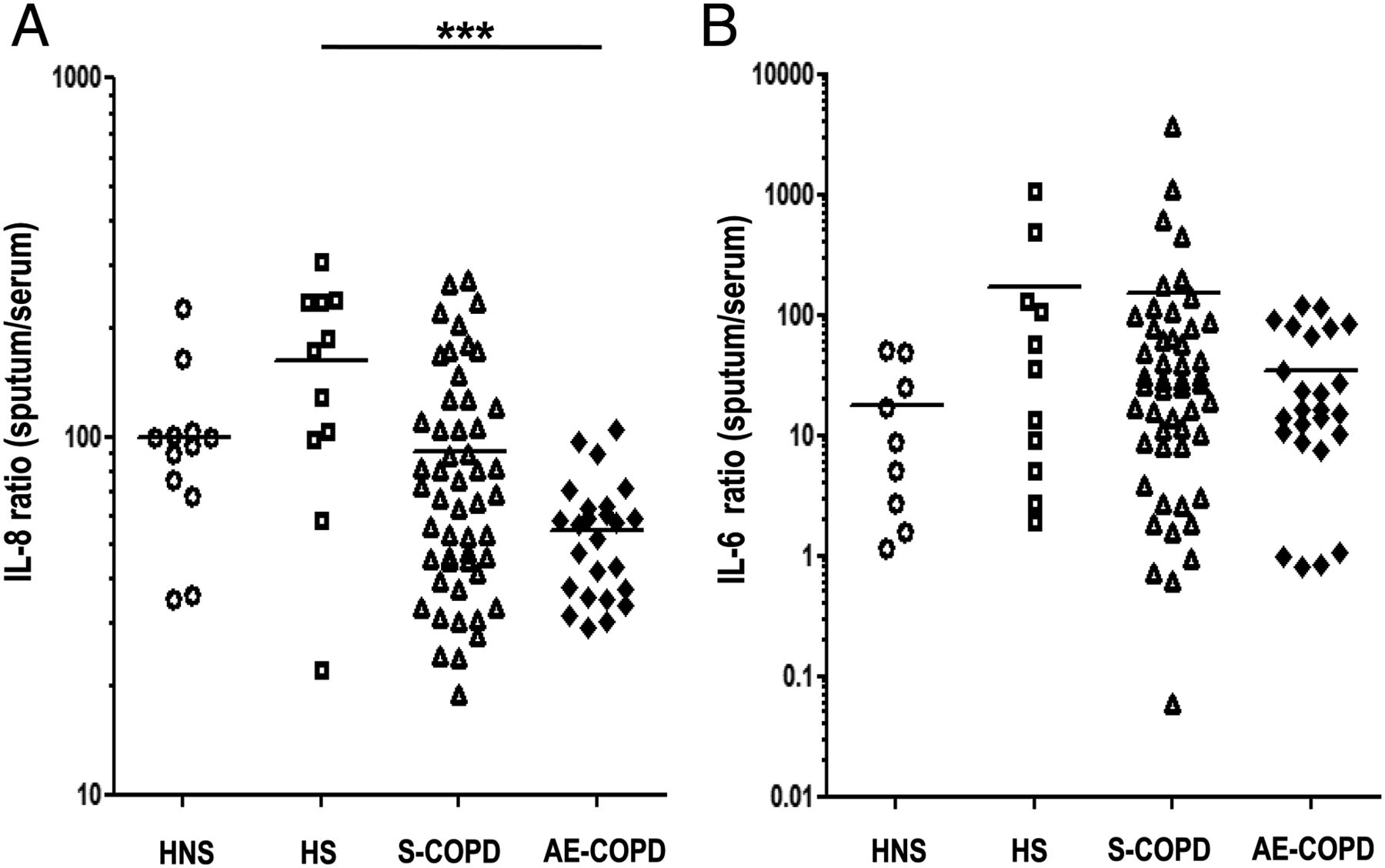
We determined whether the sputum-to-serum ratios of the levels of IL-6 and IL-8 could also be altered during exacerbations. IL-8 ratio in AE-COPD (mean 54.8; 95% CI 46.3 to 63.4) was lower than that in HS (p<0.01), but was not different from S-COPD and HNS (figure 3A). There was no significant difference in IL-6 ratio between the groups (figure 3B). Both serum and sputum IL-6 levels were increased in AE-COPD compared with S-COPD, while only serum IL-8 was increased (see online supplementary figure E2).
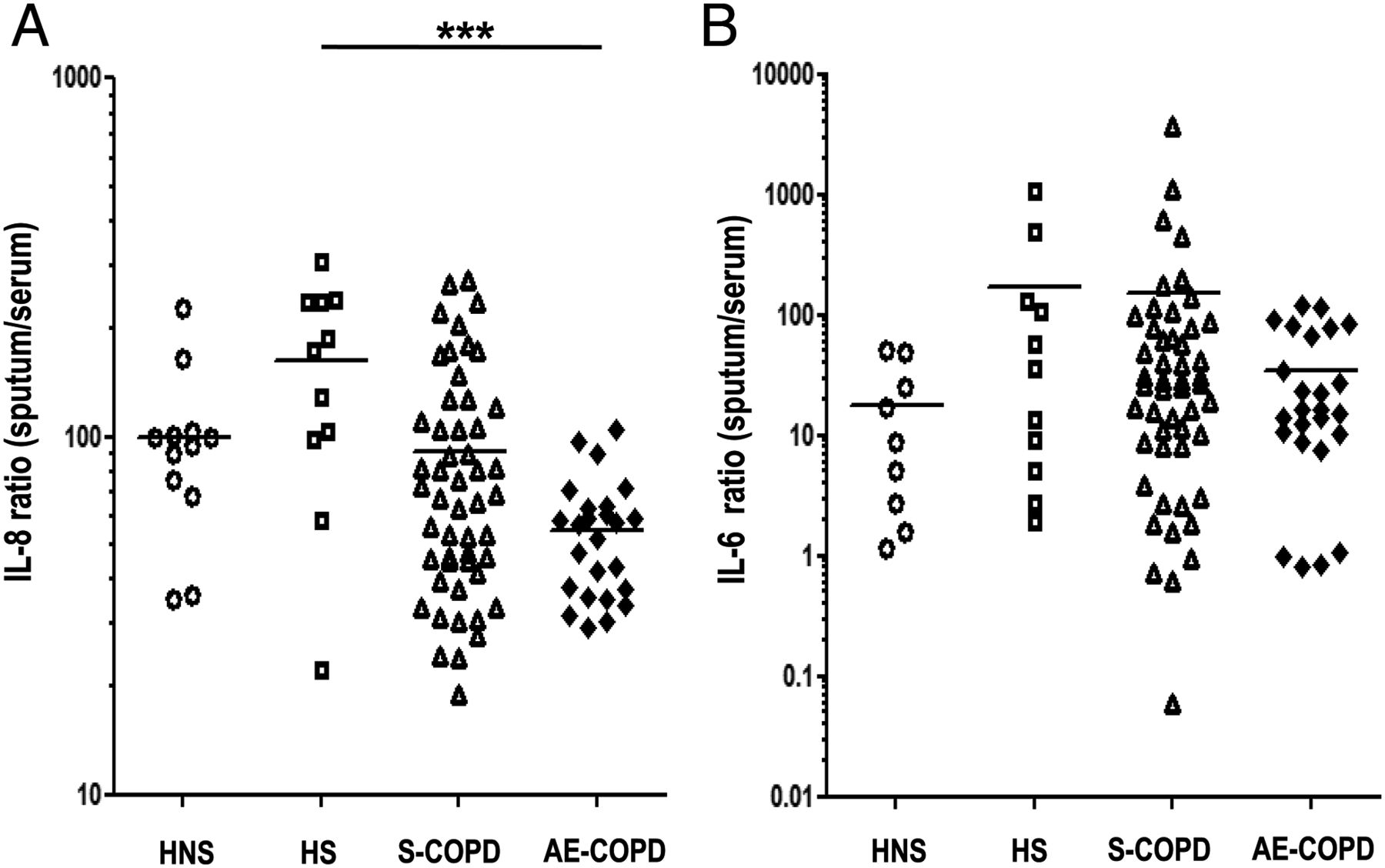
IL-8 sputum-to-serum ratio (A) and IL-6 sputum-to-serum ratio (B) from stable COPD subjects (S-COPD:Δ), COPD subjects with acute exacerbation (AE-COPD:▾), healthy smoking (HS:□) and non-smoking subjects (HNS:◯). Horizontal bars indicate mean. ***p≤0.001.
H2S ratio, bacterial sputum cultures and onset of exacerbations
H2S ratio in AE-COPD with negative bacterial sputum cultures (mean 2.33; 95% CI 0.65 to 4.01) was higher than that in AE-COPD with positive sputum cultures (mean 1.03; 95% CI 0.52 to 1.54) (p<0.05), S-COPD with negative (mean 0.28; 95% CI 0.21 to 0.36) and S-COPD with positive bacteria (mean 0.25; 95% CI 0.14 to 0.36) (p<0.001). There was no difference in H2S ratio between S-COPD with and without bacteria (figure 4A).
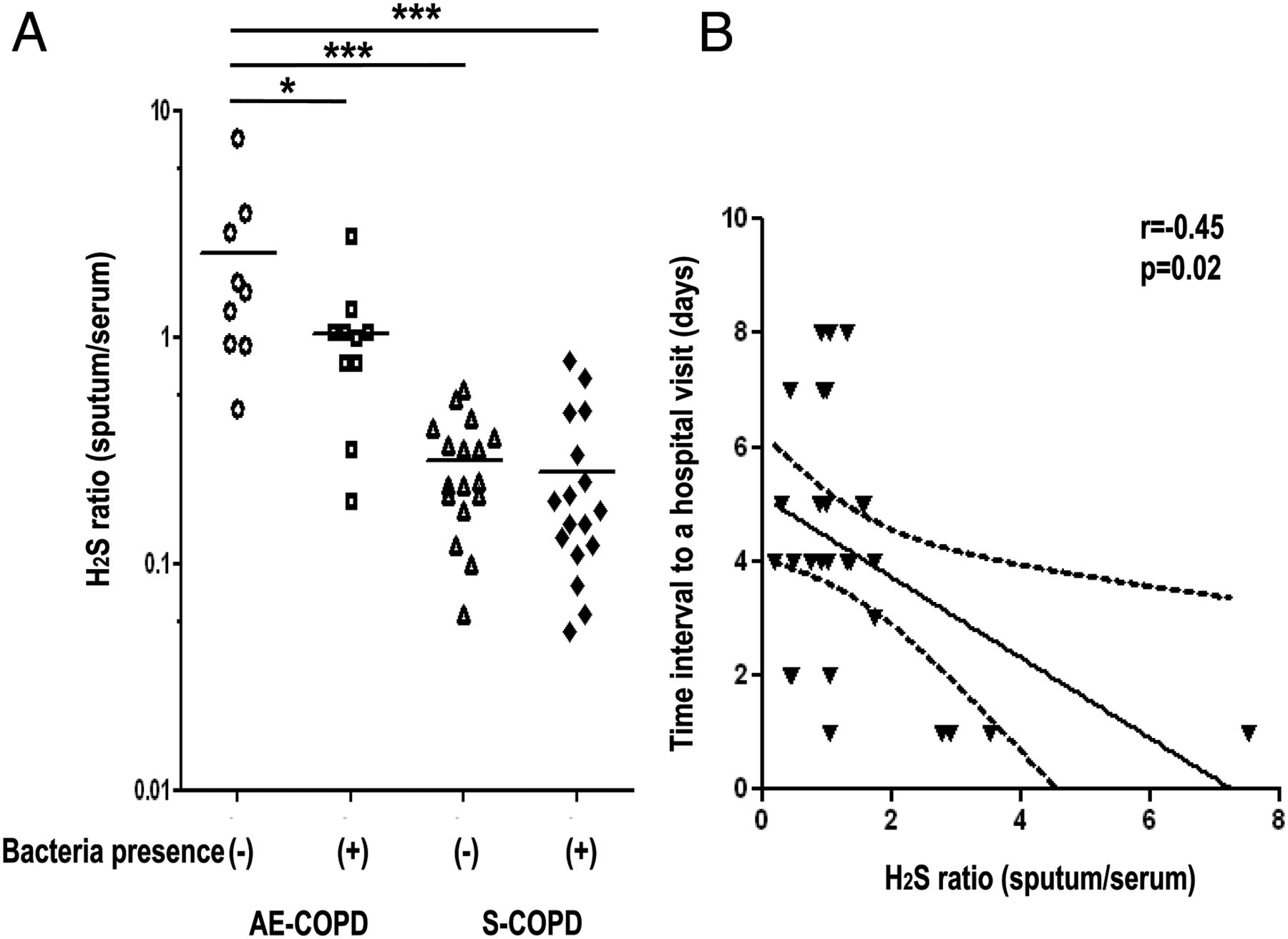
(A) H2S sputum-to-serum ratio in AE-COPD and S-COPD with and without bacterial presence; AE-COPD without bacteria (◯), AE-COPD with bacteria (□), S-COPD without bacteria (Δ) and S-COPD with bacteria (◆). Horizontal bars indicate mean. (B) Relationship between H2S ratio and the time interval from exacerbation onset to a hospital visit.
There was a negative correlation between H2S ratio and the time interval from exacerbation onset to a hospital visit, that is, the greater the H2S ratio, the shorter the time of presentation to hospital (r=−0.45; p=0.02) (figure 4B).
H2S ratio as indicative of an exacerbation
ROC curves were constructed to determine the cut-off level of H2S ratio for indicating an acute exacerbation from stable COPD (figure 5). The optimal cut-off level of H2S ratio for indicating an exacerbation was ≥0.44 (area under the curve; 0.946, sensitivity of 93.1% and specificity of 84.5%, p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operator characteristics curve for H2S sputum-to-serum ratio to predict the future risks of acute exacerbation.
Discussion
In patients with COPD, sputum H2S levels were elevated in S-COPD and AE-COPD compared with healthy smoking and non-smoking subjects; however, serum levels were higher in stable COPD but not during an acute exacerbation when compared with serum levels in healthy subjects. Chronic cigarette smoking itself did not influence serum or sputum levels. Sputum H2S levels increased and serum H2S levels dropped during acute exacerbations of COPD, as confirmed in patients where concomitant sputum and serum levels were measured at baseline and during an exacerbation. Both sputum and serum H2S levels correlated inversely with the degree of airflow obstruction, suggesting that H2S levels are closely related to physiological characteristics of COPD. There were positive relationships between sputum neutrophils (%), serum IL-8 and H2S levels in sputum and serum, indicating that H2S levels may reflect neutrophilic airway inflammation. Furthermore, H2S levels in sputum and serum were associated with SpO2 at rest, 6MWT distance, MRC score and SGRQ scores, indicating that H2S may also be a marker of the degree of physical and quality-of-life impairment.
This is the first study to examine the levels of H2S in sputum and serum during the stable and acute exacerbation phases of COPD. Previous studies have reported serum H2S levels in COPD and during chest infections19 ,27 and in agreement with our results, serum H2S levels in patients with S-COPD were found to be higher than those in HNS, with lower levels in AE-COPD.19 Interestingly, the changes in sputum and serum H2S levels between stable and exacerbation were entirely opposite with an increase in sputum H2S levels and concomitant decrease in serum H2S levels during acute exacerbation. Thus, the sputum-to-serum H2S ratio increased sixfold during an exacerbation and a ratio >0.44 was indicative of an exacerbation. By comparison, the sputum-to-serum IL-6 and IL-8 ratios did not differentiate stable COPD and COPD during an exacerbation from non-smoking and smoking healthy subjects. This lack of differentiation is explained by the fact that serum IL-6 and IL-8 levels increased during an exacerbation in contrast to the reduction in serum H2S levels; in addition, the increase in sputum cytokines during exacerbation was either negligible or small.
The role of H2S in the lungs is currently unclear. H2S possesses anti-inflammatory and antioxidant effects in the lungs. In vitro, H2S can suppress airway smooth muscle proliferation and IL-8 release,12 and induce vascular smooth muscle relaxation.28 In in vivo studies, aggravated airway hyperresponsiveness and increased airway inflammation occurred not only in mouse models of asthma with deficiency of H2S-producing enzymes29 but also in rat models of cigarette-induced inflammation when CSE was blocked.16 Therefore, H2S may have a protective role in COPD. However, other studies have revealed that H2S has a proinflammatory role in regulating the severity of LPS-induced sepsis,30 acute pancreatitis31 and burn injury.32 Inhibition of H2S in animal models was protective of organ injury in endotoxaemia30 and so systemic production of H2S might be downregulated during an exacerbation.
Endogenous H2S synthesis occurs through the action of several enzymes including CSE and CBS.14 In airway smooth muscle cells, CBS is the more important enzyme in generating H2S.12 We have preliminary data indicating that in airway smooth muscle cells from patients with COPD, there is an increase in expression of CBS. An increase in CBS may underlie the increase in H2S found in sputum and serum of COPD subjects. The increase in serum H2S we found in COPD subjects is in agreement with a previous study,19 as is our finding of a reduction in serum H2S during exacerbation. The mechanisms by which H2S levels are decreased in serum and increased in sputum are unclear. In addition to increased expression of H2S-generating enzymes such as CBS, there could be an increase in inflammatory cells in the lungs during an exacerbation together with an increased bacterial load that could add to the increased production of H2S. However, in serum, the reduction in H2S levels may be a reflection of increased sequestration of H2S from the circulation into the lungs.
In our study, the higher the levels of sputum and serum H2S, the greater were the degree of airflow obstruction and of neutrophilic inflammation. These results are similar to those found in patients with asthma where the levels of sputum and serum H2S correlated with the degree of airflow limitation and the level of sputum neutrophilia.20 In addition, in COPD, the 6MWT distance, which could be influenced by physical activity, and quality-of-life scores among many other determinants33 ,34 also correlated with sputum and serum levels of H2S indicating the potential value of measuring this diffusible marker.
Importantly, these levels may also indicate the risk of an exacerbation. A most significant observation is the decrease in the systemic levels of H2S and an increase in the lung levels of H2S during exacerbations that make this ratio a unique biomarker of a warning system for exacerbations.
We have used a sulfide-ion selective electrode to assay H2S that usually provides levels in the µM range, while other techniques have detected lower levels.27 ,35 We have added a sulfide-antioxidant buffer to our samples prior to storage and subsequent assay in order to prevent the oxidation of sulfur compounds and avoid the volatilisation of H2S.20 Thus, these levels represent the total sulfide pool (rather than solely as H2S) derived by hydroxyl replacement on cysteine residues in the blood and sputum protein pool. We performed a spiking experiment with different concentrations of H2S added to serum samples and found a tight correlation between the measured and predicted H2S levels.20 In terms of short-term reproducibility, serum H2S levels from nine healthy volunteers taken twice over a week period had a mean coefficient of variation of 6.34%.20 However, the short-term and long-term reproducibility of sputum H2S measurements in healthy or COPD subjects is not known.
Other than the inflammatory milieu, other factors may influence the levels of H2S. First, the effect of COPD medications, particularly anticholinergic, β-adrenergic agonists and inhaled or oral corticosteroids on the production of H2S, is not known. Corticosteroids may inhibit H2S production in macrophages partly through the inhibition of the H2S-producing enzyme, CSE.36 ,37 However, there was no difference in H2S levels between subjects taking and not taking inhaled corticosteroids (data not shown). Fluticasone propionate inhalation had no effect on the levels of sputum H2S in patients with COPD.38 Second, bacteria in the upper and lower airways may contribute to H2S production, particularly that the lower airways contain bacteria with an altered bacteriome in COPD.39 In addition, H2S produced by bacteria may sustain bacterial growth and suppress their sensitivity to antibiotics.40 In our exacerbating patients where conventional sputum cultures were positive for bacteria, the sputum-to-serum ratios were significantly lower than those with negative bacterial cultures, thus indicating the contribution of lower airway bacterial infections to H2S levels.
In summary, concomitant measurements of H2S in sputum and in serum may provide a novel biomarker of COPD. H2S levels may be valuable as a marker of neutrophilic inflammation, chronic airflow obstruction, physical activity and of an acute exacerbation. The clinical utility and validity of measuring the sputum-to-serum ratios of H2S will need to be tested in larger COPD cohorts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors Conception and design: KFC and JS; analysis and interpretation: KFC and JS; execution and recruitment: JS, DG, PM, CR, RS, AJM and PKB; drafting the manuscript for important intellectual content: KFC, JS and AJM.
-
Funding NIHR Biomedical Research Unit.
-
Competing interests This project was supported by NIHR Respiratory Biomedical Research Unit at the Royal Brompton NHS Foundation Trust and Imperial College London. JS was supported by a grant from the Fukushima Medical University, Fukushima, Japan. KFC is a senior investigator of NIHR.
-
Patient consent Obtained.
-
Ethics approval Ethics Committee of Royal Brompton & Harefield NHS Trust/National Heart & Lung Institute and the Ethics Committee of Royal Free Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.