Article Text

Statistics from Altmetric.com
Case description
A 33-year-old Caucasian male smoker presented to our rapid access lung cancer clinic with a single episode of moderate haemoptysis and no other respiratory or systemic symptoms. There was no relevant past medical history. As an adopted child he was unaware of any significant family history. The only finding on clinical examination was decreased air entry on the right side. Laboratory tests were all normal. Chest x-ray demonstrated a small right hemithorax with marked mediastinal displacement to the right, increased soft tissue opacity adjacent to the right side of the mediastinum causing widening of the right paratracheal stripe and loss of silhouette of the right heart border, and increased interstitial opacity throughout the right lung (figure 1A). A CT scan of the thorax confirmed the presence of a large amount of abnormal low attenuation soft tissue around the right side of the mediastinum, which also involved the azygo-oesophageal space causing considerable thickening of the oesophageal wall (figure 1B), a small right hemithorax, bronchial and non-bronchial systemic artery hypertrophy and widespread interlobular septal thickening (figure 1C). No endobronchial lesion was noted on bronchoscopy but multiple superficial vessels were present in the trachea and entrance to the right main bronchus (figure 1D). Bronchoalveolar lavage microbiology and cytology were negative. Spirometry was within the normal range. Ultrasound of the abnormal mediastinal soft tissue suggested the presence of numerous blood vessels within which slow flow could be demonstrated on Doppler. Attempted pneumonectomy was abandoned due to severe blood loss. Future embolisation is planned to reduce the bleeding risk.

(A) Chest x-ray showing a small right hemithorax with right paramediastinal soft tissue and interstitial shadowing in the right lung. (B) Axial CT image at the level of the right hemidiaphragm showing abnormal right paracardiac and paraoesophageal soft tissue. Note also the enlarged right inferior phrenic artery coursing over the top of the liver. (C) Axial CT image through the lung bases showing widespread right-sided interlobular septal thickening which was present throughout the right lung. (D) Bronchoscopy shows multiple superficial vessels in the trachea and origin of the right main bronchus. Access the article online to view this figure in colour.
ANSWER See page 99
Answer
From the question on page 93.
Discussion
The combination of a small right hemithorax, abnormal right paramediastinal soft tissue, bronchial and non-bronchial systemic artery hypertrophy and interlobular septal thickening is consistent with a diagnosis of isolated congenital unilateral pulmonary vein atresia.
This condition, without associated cardiac malformation, is very rare with fewer than 50 reported cases worldwide.1–5 Diagnosis is usually made in infancy. To our knowledge, only five adult cases have been described (table 1).1–4 Recurrent pulmonary infections (affected side), exertional dyspnoea and haemoptysis are the predominant presenting complaints.2 ,3
Reported cases of isolated unilateral pulmonary vein atresia in adults
Imaging features include:
-
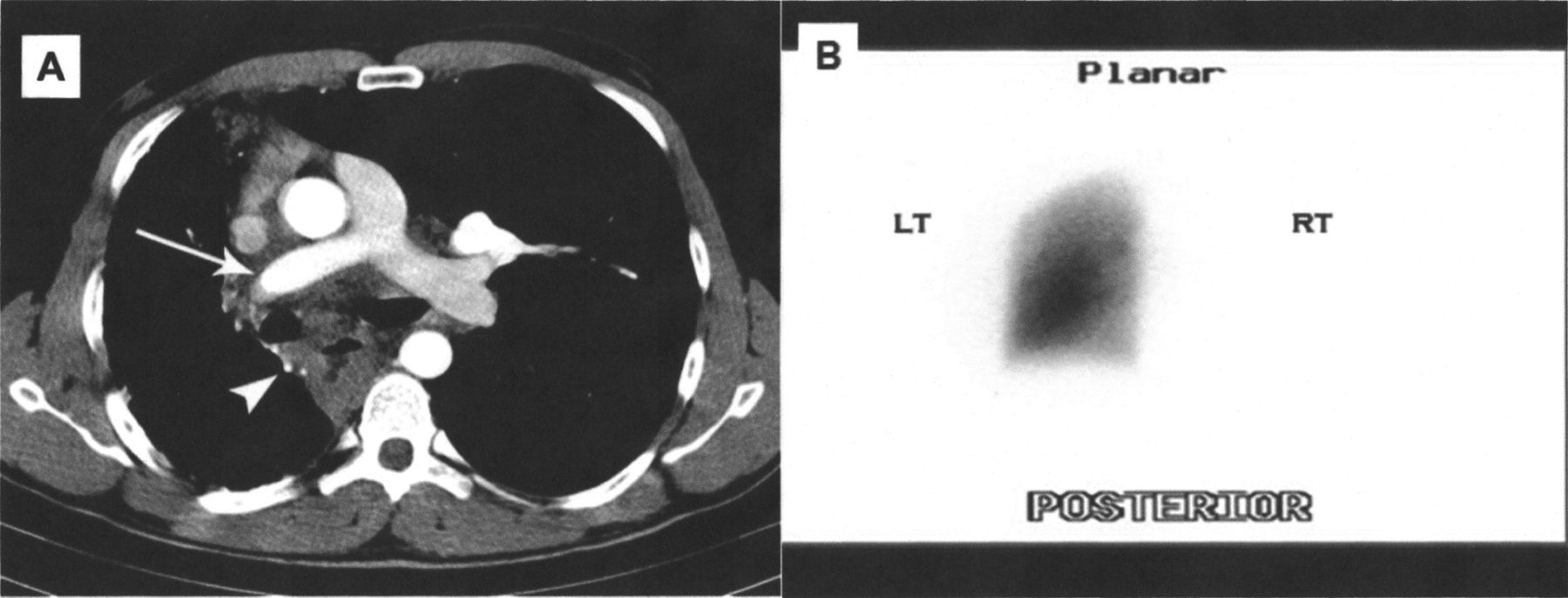
Bronchial and non-bronchial systemic artery hypertrophy which, through normal systemic artery to pulmonary artery (PA) anastomoses, causes reversal of blood flow within the ipsilateral PA. Figure 2A shows a hypertrophied right bronchial artery (arrowhead) and increased enhancement of the right PA (arrow) compared with the left. The reversal of flow is further confirmed by the complete absence of activity in the right lung on a technetium-99 m macroaggregate albumin perfusion lung scan (figure 2B).
-
Complete absence of ipsilateral central pulmonary veins with a smooth contour to the right side of the left atrium (figure 3).
-
Ipsilateral interlobular septal thickening due to severe pulmonary venous outflow obstruction (figure 1C).
-
Abnormal paramediastinal soft tissue which is largely made up of venous collaterals.2
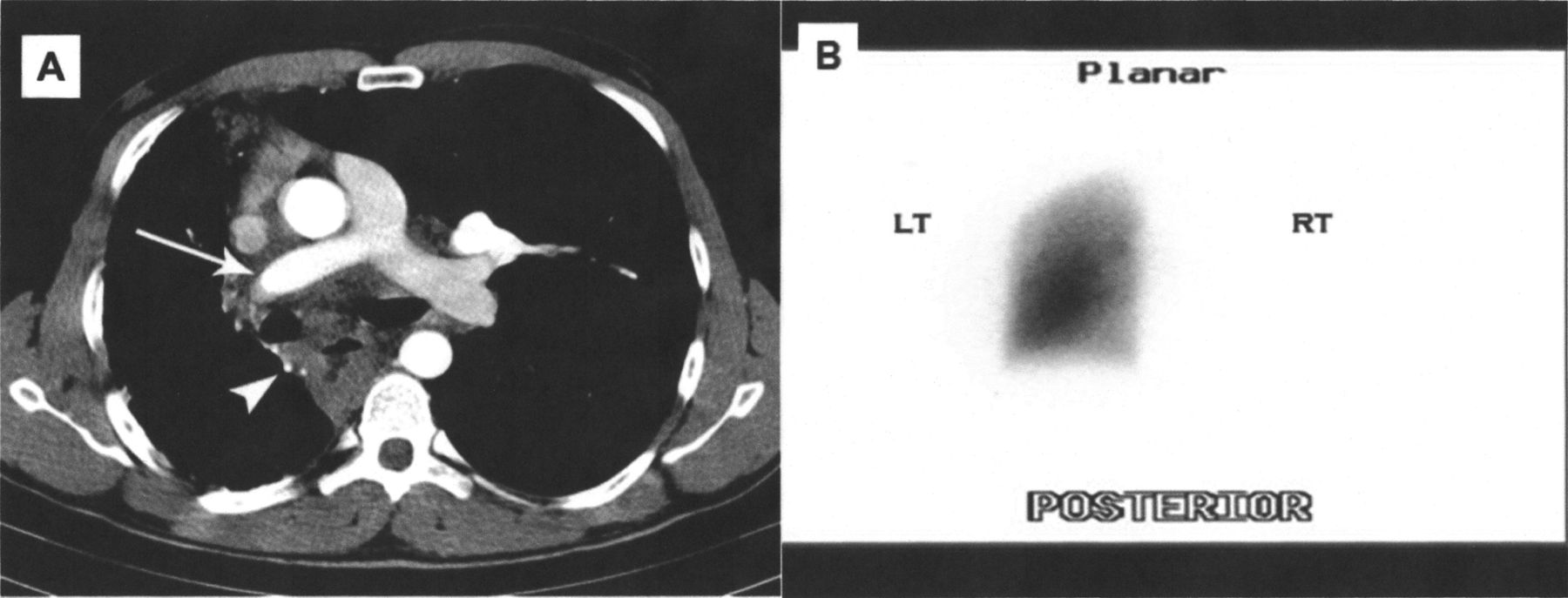
(A) Axial contrast-enhanced CT image at the level of the pulmonary artery bifurcation showing increased enhancement of the right pulmonary artery (arrow) compared with the left side and a hypertrophied bronchial artery (arrowhead). (B) Posterior lung perfusion scan (performed to confirm absence of antegrade flow in the right pulmonary artery) demonstrating absence of perfusion to the right lung. Ventilation to the right lung was normal (not shown).

{kind=link}
{kind=link}
{kind=link}
CT image through the left atrium showing a smooth contour to the right side of this chamber due to complete absence of the right-sided pulmonary veins.
Pulmonary vein atresia is caused by late failure of incorporation of the common pulmonary vein into the left atrium.4 Mortality approaches 50% if untreated.1 ,3 Management may be conservative. Outcome data from attempted restorative surgery are poor.3 ,4 Pneumonectomy, if possible, is the preferred treatment choice to avoid life-threatening haemoptysis.1–3
Footnotes
-
Contributors All authors have made substantial contributions to the conception and design of the study or acquisition and interpretation of imaging data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be submitted. RMR is responsible for the overall content as guarantor.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves