Article Text

Statistics from Altmetric.com
- Sarcoidosis
- hepatopulmonary syndrome
- transjugular intrahepatic portosystemic shunt
- pneumonia
- respiratory infection
Resident: I would like to present the case of one of my new patients. She is a 63-year-old Caucasian woman with long-term sarcoidosis of the lungs and multiorgan involvement including liver and spleen. Despite pneumological surveillance and prednisolone treatment, her respiratory situation worsened, and was started on home oxygen treatment 5 years ago when fibrosis of the lungs was diagnosed. She also has severe osteoporosis due to long-term steroid use and immobility. She is now presenting with worsening dyspnoea of a duration of 4 months despite using 8 litres of oxygen.
I admitted a prematurely aged woman in a poor general condition. She presented with dyspnoea, right upper quadrant abdominal pain and back pain. A physical examination revealed stigmata of hypoxaemia, light crackles on both lungs, clinical signs for steroid use and an enlarged liver painful on palpation. She is a non-smoker and she has no history of cardiac diseases or cardiac involvement by sarcoidosis. An echocardiogram was normal and right heart catheterisation 2 months ago showed no pulmonary hypertension. There was no fever or relevant inflammation parameters. Laboratory tests revealed a mild hyperbilirubinaemia of 1.8 mg/dl, slightly reduced albumin of 32 g/litre, normal transaminases and an elevated γ-glutamyl transpeptidase (GGT) (981 U/litre) and alkaline phosphatase (AP) (559 U/litre). Her International Normalised Ratio (INR) was within the normal range. An ultrasound scan showed an enlarged liver and spleen and some ascites.
Consultant: Concerning her respiratory situation, we have to think of a worsening of lung fibrosis due to sarcoidosis, since there is no trace of cardiac or infectious conditions so far. You should perform spirometry, blood gas analysis and a high-resolution CT scan of her chest. Besides, she seems to have a problem of the liver, which we know is affected by sarcoidosis in her case as well. Please complete history and examinations on liver disease. If she shows any signs for portal hypertension, we will perform a liver biopsy and measure her portosystemic gradient.
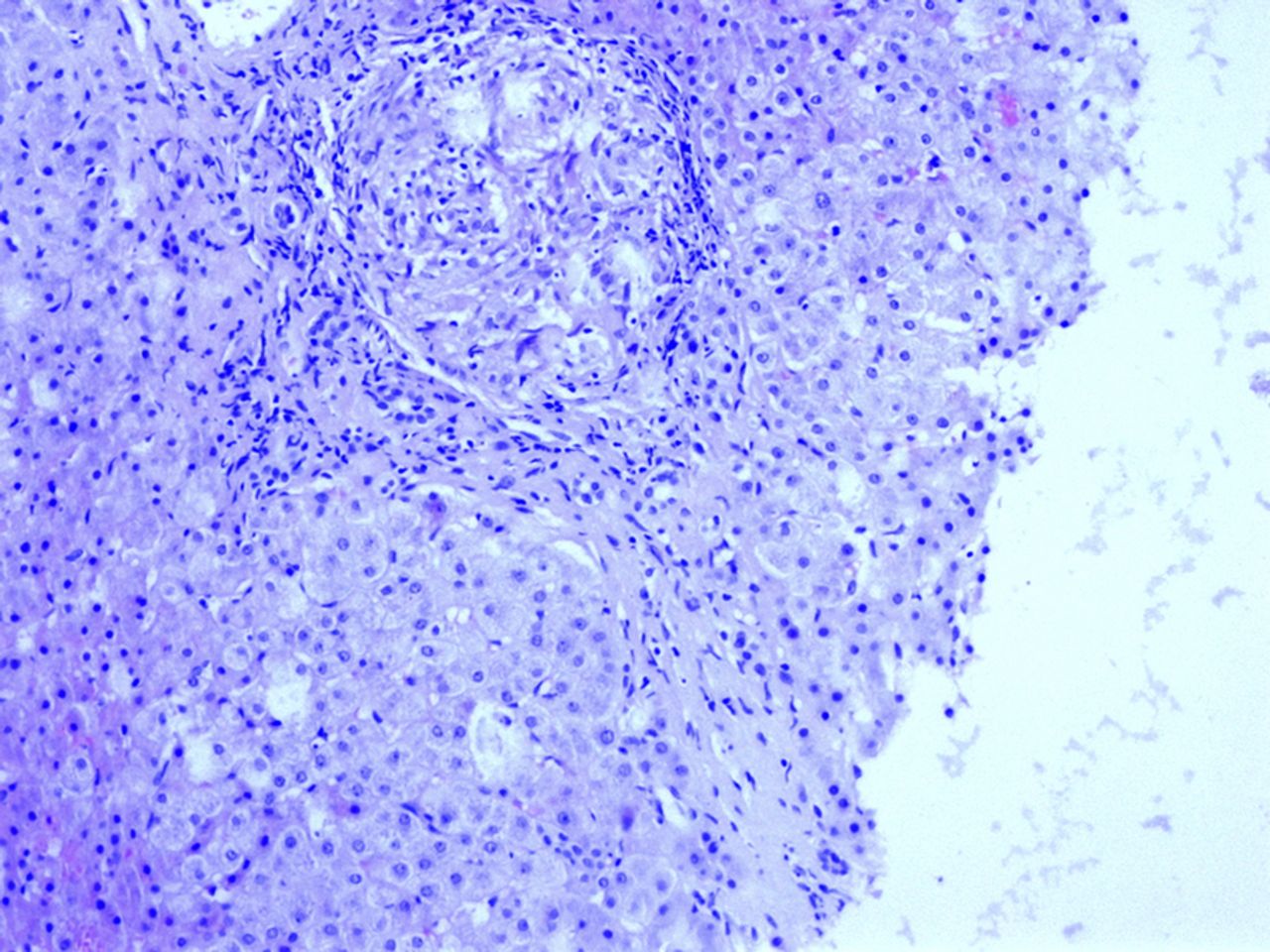
R: Her pulmonary function tests revealed severe hypoxaemia (PaO2 of 49 mm Hg with 8 litres of oxygen/min). Her vital capacity was 68% of the expected value. The CT scan showed second degree sarcoidosis without ground glass capacity, similar to the last examination in her reports. Ultrasound, gastroscopy and angiography revealed severe portal hypertension, including gastro-oesophageal varices with red spots and a portosystemic gradient of 19 mm Hg (normal range: 1–4 mm Hg). The liver biopsy showed granulomas consistent with sarcoidosis in a cirrhotic liver (figure 1). Her Child–Pugh–Score is 7 points (class B).

{kind=link}
Granulomatous lesions from the patient's liver biopsy.
Thinking of other causes for liver disease, there was no clinical or laboratory evidence for alcohol abuse or metabolic conditions including non-alcoholic fatty liver disease. Chronic viral hepatitis could be ruled out, and her autoimmune serology was unremarkable. The biopsy showed no other features of liver diseases or other causes of hepatic granuloma such as tuberculosis or primary biliary cirrhosis. Other infectious causes for hepatic granuloma are very unlikely since the patient has no history of travelling. The orthopaedic surgery department was consulted for her severe back pain. They have found destructing inflammation in her lower spine and pelvis.
C: That is an interesting development, since though sarcoidosis involves the liver in up to 80% by biopsy, only very few patients develop cirrhosis and portal hypertension.1 As we have a discrepancy between the pulmonary status and the degree of hypoxaemia, the reason for worsening dyspnoea may not be lung fibrosis. Apart from hepatic hydrothorax, portopulmonary hypertension, cirrhotic cardiomyopathy or respiratory infections, hypoxaemia in patients with chronic liver disease can be caused by hepatopulmonary syndrome (HPS),2 so we have to check on this.
R: Indeed, by using shaken saline for contrast-enhanced echocardiography we detected microbubbles in the left atrium as a sign of pulmonary vascular dilatations. Taken together with the other findings, severe HPS due to sarcoid liver disease is the most likely diagnosis. I have found only three reported cases with sarcoidosis of the liver causing HPS.3 All patients were initially diagnosed as having extrahepatic sarcoidosis and developed serious affection of the liver with granulomas and cirrhosis. In these cases only oxygen treatment was administered. In our severe case of hypoxaemia oxygen supplementation is not sufficient any more. Orthotopic liver transplantation (OLT) is the only potential cure for HPS,2 for which our patient might be a candidate.
C: In the interdisciplinary transplantation board the patient was considered to be not a candidate for OLT due to her respiratory impairment, disseminated sarcoidosis and immobilising instability of her pelvis, which cannot be surgically treated according to the consulted orthopaedic surgeon. As a palliative treatment we may consider a transjugular intrahepatic portosystemic shunting (TIPS), which is a possible treatment for complications of liver disease. There are a number of case reports that have demonstrated improvement of HPS after TIPS, although there is not enough evidence for routine treatment and no TIPS has been performed in patients with hepatic sarcoidosis with HPS.4
R: Our patient consented to a TIPS procedure after thorough explanation of risk and expected benefits. TIPS implantation was technically successful and the stent was patent in several follow-up Duplex mode ultrasound examinations. At 6 weeks after TIPS the patient had a PaO2 of 102 mm Hg with 8 litres of oxygen. However, she felt no subjective relief and would keep on using large amounts of supplemental oxygen. Almost 9 months after TIPS implantation she was admitted with Clostridium difficile-associated diarrhoea after antibiotic treatment for a urinary tract infection. Attempts in the meantime to withdraw her from oxygen have failed. Blood gas analysis under 8 litres oxygen/min showed hypoxaemia and orthodeoxia (55 mm Hg in upright, 64 mm Hg in supine position).
C: The final clinical outcome is quite disappointing. However, we have to take into account that the TIPS was implanted as a last attempt to improve hypoxaemia. Our evaluation 9 months after TIPS might be confounded by a progress of lung fibrosis suggested by reduced vital capacity compared to the year before (38% vs 68% of the expected value). The repeat CT scan, however, revealed no significant changes. If we take a look at the seven existing case reports, only three patients were successfully bridged to OLT. The other reports describe patients improving clinically within a few weeks although the reported follow-up periods were short, with 4 months and 6 months being used, as well as 8 months in a paediatric case. The longest follow-up described a stable status 3 years after TIPS. However, there is a small case series reporting seven patients, of which only one temporally improved after TIPS.5
Our case may teach us that sarcoidosis of the liver does not just cause severe liver disease but can also be responsible for severe portal hypertension leading to HPS in rare cases. This has to be considered if hypoxaemia and lung affection from sarcoidosis do not match. A benefit after TIPS implantation in HPS has been described only in case reports. Although patient numbers are low, controlled trials including a longer follow-up are required to provide evidence for efficacy of TIPS on hypoxaemia. To avoid confounding by coexisting causes of hypoxaemia semiquantitative measurement of shunting can be performed by using technetium-labelled macroaggregated albumin scanning before and after TIPS. Until there is more evidence, treatment of HPS with TIPS remains an experimental attempt to bridge highly selected patients until OLT.
Acknowledgments
We thank Dr Alexander Quaas for contributing the photo of the pathology slide.
Footnotes
-
Contributors Planning and drafting the manuscript: M Nistal, A Pace; critical reviewing of the manuscript: H Klose, D Benten; critical reviewing of the manuscript and conducting: A Lohse.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves