Article Text

Abstract
Background Patients with fibrotic interstitial lung disease have symptom control and quality of life (QoL) needs. This review aims to evaluate the evidence for the use of interventions in improving dyspnoea, other symptoms and QoL.
Methods Eleven databases, relevant websites and key journals were hand-searched. Studies were assessed and data extracted independently by two researchers using standardised proformas. Meta-analyses were performed where possible with 95% CI.
Results 34 papers with 19 interventions in 3635 patients were included. Meta-analyses showed no significant effect of interferon γ-1b or sildenafil on 6-minute walking distance (6MWD) or dyspnoea. Pulmonary rehabilitation and pirfenidone had a positive effect on 6MWD (mean difference (95% CI) 27.4 (4.1 to 50.7)) and 24.0 (4.3 to 43.7), respectively), and pulmonary rehabilitation had a mixed effect on dyspnoea. Both pulmonary rehabilitation and sildenafil showed a trend towards significance in improving QoL. There was weak evidence for the improvement of 6MWD using oxygen; dyspnoea using prednisolone, diamorphine, D-pencillamine and colchicine; cough using interferon α and thalidomide; anxiety using diamorphine; fatigue using pulmonary rehabilitation; and QoL using thalidomide and doxycycline. A wide range of outcome scales was used and there were no studies with economic evaluation.
Conclusions There is strong evidence for the use of pulmonary rehabilitation and pirfenidone to improve 6MWD and moderate evidence for the use of sildenafil and pulmonary rehabilitation to improve QoL. Future recommendations for research would include careful consideration of the dichotomy of radical and palliative treatments when deciding on how symptom and QoL outcome measures are used and data presented.
- Interstitial Fibrosis
- Palliative Care
- Pulmonary Rehabilitation
Statistics from Altmetric.com
Key messages
What is the key question?
-
What is the overall outcome of trials assessing the use of pharmacological and non-pharmacological methods to improve symptom control and QoL in patients with progressive idiopathic fibrotic interstitial lung diseases?
What is the key point?
-
There is strong evidence for the use of pulmonary rehabilitation and some evidence for sildenafil and pirfenidone. There is weak evidence for a number of other interventions which warrants further investigation.
Why read on?
-
All patients with progressive idiopathic fibrotic interstitial lung diseases should receive best supportive care to improve symptom control and QoL and, where possible, this should be evidence-based.
Introduction
Patients with interstitial lung disease have a wide range of diagnoses and prognoses. Many patients can live many years with their diagnosis and some are responsive to treatments. However, a subset of patients with progressive idiopathic fibrotic interstitial lung diseases (PIF-ILD), such as idiopathic pulmonary fibrosis (IPF), have a short disease trajectory and a similar prognosis to patients with lung cancer.1
Only a small number of patients are suitable for lung transplantation and no other treatments have been shown to influence mortality. Evidenced-based palliation is seldom applied, despite the high symptom burden2 and poor quality of life (QoL).3
In this systematic review of PIF-ILD, we evaluate (1) the evidence for the use of interventions to improve symptoms and QoL; (2) the evidence for the use of symptom scales for dyspnoea and other symptoms; and (3) the cost-effectiveness of interventions to improve symptoms and QoL. In addition, we aim to make a crucial distinction between radical (potentially disease-modifying) and palliative (non-disease-modifying) treatments, and consider this in appraising the evidence as interpretation of secondary outcome measures should differ between these contexts.
Methods
Search strategy
We performed comprehensive searches of 11 electronic databases including MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials (CENTRAL) from 1966 to December 2010 using a combination of MESH headings and keywords (for full search strategy see online appendix 1). In addition, three key respiratory journals (Thorax, American Journal of Respiratory and Critical Care Medicine and Chest) were hand-searched for the last 3 years, with reference lists of all included papers. The search was updated to September 2011. Study authors were contacted to obtain full reports where abstracts only were available or further information was required (authors contacted twice in 1 month period). No language restrictions were imposed and translation was performed where needed.
Selection
Study populations
Published data for patients diagnosed with IPF, non-specific interstitial pneumonia (NSIP), cryptogenic fibrosing alveolitis (CFA) and idiopathic interstitial pneumonia (IIP) were evaluated. All stages of disease were included. Studies including subjects with other forms of ILD were acceptable if outcomes for PIF-ILD were reported separately. Where necessary, authors were contacted and, if no separate data was obtainable, the study was excluded but listed as potentially relevant.
Types of interventions
Any single or combined interventions for the treatment of PIF-ILD were reviewed including pharmacological and non-pharmacological treatments, with the exception of lung transplantation.
Types of comparison
Because of the paucity of evidence, all intervention comparisons were assessed but meta-analysis was only conducted for randomised controlled trials (RCTs) of placebo-controlled interventions.
Types of outcome measures
The outcomes included were effects on dyspnoea (at rest), QoL, all other symptoms, 6-minute walking distance (6MWD) and economic data.
Types of study included
A scoping search identified a paucity of controlled trials so all trials, including prospective and retrospective studies, were evaluated. Studies published only in abstract form were included if sufficient information was available to satisfy inclusion criteria. Higher weighting was given to randomised placebo-controlled studies. The quality of RCTs was assessed as described by Jadad et al.4 Studies with qualitative enquiry or mixed method designs were also included. Studies with fewer than five patients were excluded. Paediatric studies were excluded due to radical differences in the PIF-ILD syndromes between childhood and adulthood.5
Data extraction
Details of data extraction can be found in online appendix 1.
Data analysis
Where data quantity and quality allowed, data were combined using fixed or random effects meta-analysis. The choice of model was determined by the degree of heterogeneity, as judged by the I2 statistic and p value for the χ2 test (a random effects model was used if p<0.10 and/or I2>50%). Results are presented as pooled mean differences between intervention and placebo groups with 95% CI. Forest plots are used to display the results from the individual studies and the pooled estimate. For single studies, the effect size and 95% CI were calculated using standard formulae when not reported in the original paper. A descriptive summary of other studies has been given.
Results
Overview of included studies
Joint data extraction was conducted for 75 papers with interventional data (figure 1). Thirty-four papers were included (see online appendix 2) and 41 were excluded or listed as potentially relevant (see online appendix 3). Of the 34 papers included, these reported 35 studies (two papers each contained two studies6 ,7 and one study was reported in two papers8 ,9). No health economic papers were identified.

Flow of studies through review.
Seventeen pharmacological interventions and two non-drug interventions were evaluated. In total, 3635 patients were used in the analysis (IPF, n=3419; CFA, n=153; IIP, n=54; usual interstitial pneumonia (UIP), n=9) with a range of 6–826. Interferon γ-1b (IFNγ-1b) was the intervention most tested, with the greatest number of patients analysed, the greatest number of RCTs and the largest individual RCT. Pulmonary rehabilitation had the largest number of studies (n=6).10–15
The 17 RCTs had an average Jadad score of 4 (range 2–5). There was a preponderance of placebo-controlled RCTs with few comparisons across classes (notably between pharmacological and non-pharmacological interventions). Twenty-six studies used American Thoracic Society/European Respiratory Society (ATS/ERS) diagnostic criteria.16 Only two papers were not published in English.13 ,17
Studies were funded by industry (20%), industry and other sources (6%), government (6%), investigators (3%) and other sources such as charities (31%), with the funding source unclear in (34%).
Outcome measures
There were a wide range of outcome measures for dyspnoea and QoL (table 1, see appendix 4).
Outcome measures used in studies analysed
Interventions
Interventions are presented in order of weighted evidence by study design and subdivided into 6MWD, dyspnoea and other symptoms and QoL. Evidence supported by meta-analysis is listed as ‘strong’, if supported by single RCTs the evidence is listed as ‘moderate’. All other evidence which is supported by non-RCT study designs has been listed as ‘weak’. A summary of the results are presented in table 2 and effect sizes are shown in table 3 with full results in appendix 2.
Summary of studies included and results (presented as radical or palliative treatments and in order of weighted evidence)
Effect sizes and pooled estimates where applicable
Interventions trialled in RCTs
Interferon γ-1b (IFNγ-1b)
6MWD, dyspnoea and cough: Three RCTs23 ,25 ,32 studied IFNγ-1b in 908 patients. There were no significant effects of IFNγ-1b on 6MWD (figure 2), dyspnoea (figure 3) or cough.
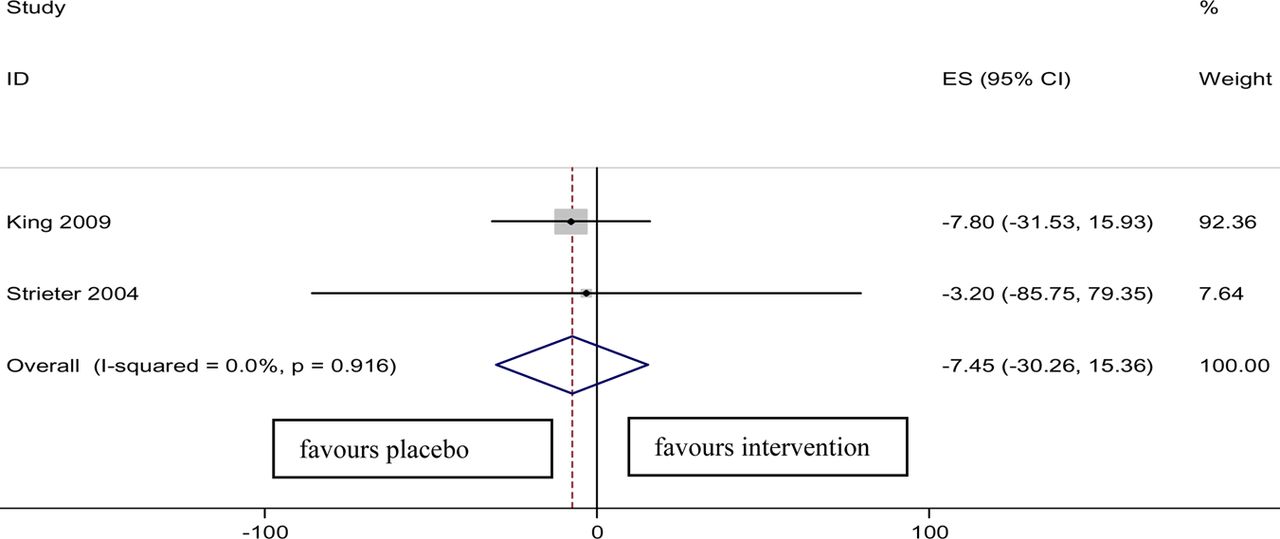
Forest plot showing comparison of effect of interferon γ-1b (IFNγ-1b) versus control on change in 6-minute walking distance (6MWD): effect size −7.45 (95% CI −30.26 to 15.36), p=0.52. Access the article online to view this figure in colour.

Forest plot showing comparison of effect of interferon γ-1b (IFNγ-1b) versus control on change in San Diego breathlessness scale: effect size 0.08 (95% CI −4.18 to 4.34), p=0.97. Access the article online to view this figure in colour.

Forest plot showing comparison of effect of sildenafil versus control on change in 6-minute walking distance (6MWD): effect size 5.25 (95% CI −8.90 to 19.40), p=0.467. Access the article online to view this figure in colour.
QoL: There was a significant difference in St George's Respiratory Questionnaire (SGRQ) symptom domain favouring IFN in one study (change in mean score from baseline: IFN −13.2 (95% CI −21.4 to 5.0) vs colchicine 7.5 (95% CI −4.5 to 19.5), p=0.01).23 However, no other improvements in QoL were seen.
Sildenafil
Sildenafil was trialled in four studies, two RCTs6 ,21 (one of which6 which was followed by an open-label study) and an uncontrolled quasi-experimental study.20 A total of 378 patients were used in the analysis.
6MWD: Collard et al20 conducted an open-label uncontrolled quasi-experimental study which found a significant mean improvement in 6MWD of 49.0 m (95% CI 17.5 to 84.0). Eleven patients were used in the analysis. However, a meta-analysis of data from the two larger RCTs6 ,21 did not support this finding (figure 4).
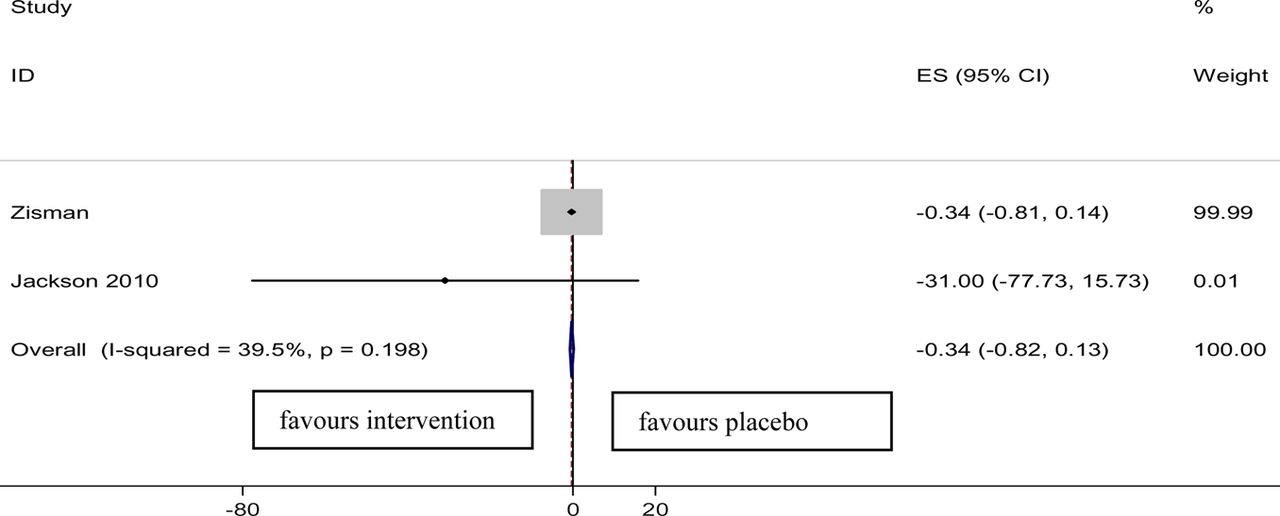
Forest plot showing comparison of effect of sildenafil versus control on change in Borg score at rest: effect size -0.34 (95% CI −0.82 to 0.13), p=0.157. Access the article online to view this figure in colour
Dyspnoea: One RCT6 showed less deterioration in dyspnoea but overall benefit was not supported by meta-analysis (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing comparison of effect of pulmonary rehabilitation versus control on change in 6-minute walking distance (6MWD): effect size 27.4 (95% CI 4.1 to 50.7), p=0.021. Access the article online to view this figure in colour.
QoL: Zisman et al6 found that the SGRQ total score remained stable in the sildenafil group but worsened in the placebo group (mean difference −4.08 (95% CI −7.3 to −0.86)). The Short Form Health Survey (SF-36) general health subscore was better preserved in the sildenafil group than in the placebo group (mean difference 2.86 (95% CI 0.76 to 4.95)). This was not seen during the open-label phase.
Pulmonary rehabilitation
Six studies used pulmonary rehabilitation as the intervention. These included two RCTs10 ,11 and four quasi-experimental open-label studies,12 14 15 of which two had controls. A total of 194 patients were used in the analysis.
6MWD: Meta-analysis showed an overall significant benefit of pulmonary rehabilitation on 6MWD (figure 6). This was also supported by other non-randomised studies.12 ,14 ,15
Dyspnoea and other symptoms: Nishiyama et al10 found no significant effects on dyspnoea. However, in a subset of patients in the paper by Holland et al,11 even though improvements were not seen in the MRC scale, a positive effect was seen for the Chronic Respiratory Disease Questionnaire (CRDQ) dyspnoea score. Kozu et al14 also found a significant improvement in dyspnoea in the IPF subgroup (p<0.01). Ozalevli et al12 found a significant decrease in baseline MRC score after pulmonary rehabilitation (p=0.003) and Rammaert et al13 found non-significant changes in the Borg and MRC scales. Swigris et al15 found that there was a significant improvement in fatigue. There were no significant improvements in anxiety, depression or sleep quality.
QoL: Two RCTs10 ,11 found positive effects on QoL in a number of domains of the SF-36, CRDQ and SGRQ, of which the SGRQ total score was also significant (p<0.05). This was supported by Ozalevli et al12 and Rammaert et al13 who found that, among other positive QoL results, SF-36 physical limitation scores decreased significantly post-intervention (p=0.05).13 Other non-randomised studies did not find any positive effects on QoL.14 ,15
Bosentan
Two RCTs were reported in three papers trialling bosentan,8 ,9 ,26 with 769 patients included in the analysis.
6MWD: BUILD-1 showed no benefit of bosentan compared with placebo for 6MWD.8 ,9
Dyspnoea: In BUILD-1 there was no significant effect of bosentan on dyspnoea in the total population or in the diagnostic biopsy subset at the primary endpoint of 12 months.8 ,9 These findings were supported by a second larger RCT (BUILD-3).26
QoL: BUILD-1 found no difference for any domain of the SGRQ at 12 months.8 Forty-two percent of bosentan-treated patients had an improved SF-36 health transition score compared with 28% of the placebo group (p=0.084). However, a subanalysis of patients who had undergone diagnostic biopsy favoured bosentan, showing a significant beneficial effect on QoL with mean total SGRQ scores favouring bosentan.8 Significant treatment effects were observed at 12 months in the impact domain of the SGRQ (median treatment effect (MTE) −7.0, p=0.03) and the physical functioning (MTE 9.3, p=0.04), general health (MTE=9.4, p=0.01) and role emotional domains of the SF-36 (MTE 0.0, p=0.04).9 However, none of these findings were supported in the larger BUILD-3 study.26
Pirfenidone
Two RCTs (CAPACITY) testing pirfenidone were presented in one paper.7 A total of 692 patients were included in the analysis. Significant improvement was seen in 6MWD of pooled data for the intervention group compared with placebo (absolute difference 24.0 m (95% CI 4.3 to 43.7)). No significant change in dyspnoea score was seen (table 3) and there were no QoL data.
N-acetylcysteine (NAC)
Two RCTs39 ,31 with 177 patients included in the analysis did not show any significant differences for aerosolised or oral NAC compared with control for 6MWD, dyspnoea or QoL.
Co-trimoxazole
A pilot RCT of 20 patients compared oral co-trimoxazole alone with a combination with oral prednisolone.24
Dyspnoea and other symptoms: The MRC dyspnoea score showed improvement with a median score of 3 (95% CI 2 to 4) before treatment compared with 2 (95% CI 1 to 3) 3 months after treatment for the active group (p=0.05) which was maintained at 12 months. The Borg breathlessness score and visual analogue scale (VAS) score were significantly improved (data not presented in paper). Cough improved within 4 weeks of treatment (p=0.002) (data not presented in paper).
QoL: The SGRQ showed a significant reduction in symptom scores in the co-trimaxole group (p=0.05) but an improvement was also seen in the placebo group (p=0.02). Non-significant effect sizes were seen for other components of the SGRQ.
Etanercept
A RCT of etanercept in 87 patients with IPF showed no significant improvement in 6MWD (table 3), dyspnoea or QoL compared with placebo (data not presented in paper).35
Iloprost
A RCT of 51 patients treated with inhaled iloprost showed no significant differences between inhaled iloprost and placebo for change in 6MWD or Borg dyspnoea score (data not presented in paper).18
Disease management programme
Lindell et al33 conducted a RCT of 21 patients which compared a disease management programme delivered using a format of support group for both patients with IPF and carers with a control group of best usual care. There was mixed evidence of benefit.
Quantitative work suggested a negative impact of this intervention on perceptions of physical QoL and a tendency for greater anxiety. The mean end Beck Anxiety Index scores approached statistical significance (intervention 15.13 (6.92) vs control 8.56 (6.95), p=0.077), reflecting increased anxiety in the intervention group. The mean (SD) end score for the SF-36 physical component showed a statistically significant difference (intervention 31.06 (4.61) vs control 36.04 (4.63), p=0.038), reflecting a negative impact on perceptions of physical health-related QoL. However, qualitative work in which 19 participants in the experimental group were interviewed found that patients did not feel isolated and felt that the intervention had enabled them to put the disease into perspective, gave comfort and provided an improved mental picture.
Interventions trialled more than once in non-randomised controlled studies
Prednisolone
Two quasi-experimental studies30 ,36 and one retrospective review28 were included. A total of 163 patients were used in the analysis.
Dyspnoea and other symptoms: Fiorucci et al30 conducted a three-arm study of 30 patients using prednisolone alone (group 1), prednisolone and cyclophosphamide (group 2) and prednisolone and colchicine (group 3). There were significant improvements in dyspnoea in the prednisolone and colchicine group compared with the two other groups (mean (SD) baseline dyspnoea score 8.4 (2.5) vs 6.3 (2.2) at 18 months (p=0.001)). Two patients in group 1 (18%), one patient in group 2 (11%) and eight patients in group 3 (80%) showed a significant decrease in dyspnoea (p=0.001). However, the numbers were small and the study was conducted in a single centre. Turner Warwick et al28 conducted a retrospective review which included 127 patients in the analysis. After 4–6 weeks of treatment, 55 (43%) were classified as non-responders and 72 (57%) as responders with improvement in dyspnoea on a 4-point scale. However, patients were classed as CFA using the criteria of Turner Warwick et al41 without diagnostic biopsies.
Hope-Gill et al36 conducted an open-label study of prednisolone on capsaicin-induced cough and found a significant reduction in cough reflex sensitivity to capsaicin with a reduction in the mean (SE) VAS score from 7.2 (0.8) to 2.2 (2.5) at 4 weeks (p<0.05). However, the numbers were small (n=6) and only five of the six patients reported VAS data.
No 6MWD or QoL data were available for prednisolone.
Oxygen
6MWD: Hicks et al19 conducted a retrospective review of 70 patients with IPF to assess the benefits of ambulatory oxygen. Patients not requiring regular oxygen before the study managed to walk further on optimal oxygen therapy (mean 81.2 m, p<0.01). Patients already on regular oxygen showed less benefit on optimal oxygen therapy, walking an extra 16.9 m (p=0.02). A second retrospective review22 of 34 patients with IPF/NSIP showed that ambulatory oxygen (additional or increased) significantly improved 6MWD from baseline (mean (SE) 272.3 (19.8) m vs 304.7 (17.8) m, p=0.0001).
Dyspnoea: Visca et al22 found that dyspnoea measured by the Borg scale improved with oxygen (median 4.25 (95% CI 3 to 5) at baseline vs 3.25 (95% CI 2.5 to 4) on oxygen, p<0.00001). Borg scores at the end of the study were not significantly different using optimal oxygen than baseline tests in the study by Hicks et al.19
There were no QoL studies for oxygen.
Interventions trialled only once in non-randomised open-label uncontrolled studies
Diamorphine
An uncontrolled quasi-experimental open-label study27 of 11 patients on subcutaneous diamorphine showed no adverse effects on vital signs and oxygen saturation but a substantial fall in the dyspnoea analogue score from a mean (SD) of 83 (13) at baseline to 36 (11) at 15 min and 36 (12) at 30 min (p<0.001). The authors also reported decreased observed anxiety (no details given). However, strict diagnostic criteria were not used.
D-pencillamine
An uncontrolled quasi-experimental open-label study of D-pencillamine in 10 patients with IPF showed improvement by one full grade on the New York Heart Association (NYHA) dyspnoea scale in 50% of patients.34 No diagnostic criteria were given.
Interferon α
A quasi-experimental open-label study using interferon α lozenges showed improvements in frequency, duration, intensity of daytime cough and improvements in night-time cough.37 Five of six subjects with chronic cough who completed the Leicester Cough Questionnaire improved with a mean change in total score from baseline of 3.16 (95% CI 1.58 to 4.74), where 1.3 is considered to exceed the minimal important difference.
Ribavarin
An uncontrolled quasi-experimental open-label study of 10 patients with ribavirin showed no significant change in dyspnoea.29
Thalidomide
Cough: A phase II trial of the effect of thalidomide on cough in 11 patients with IPF showed marked improvement/resolution of symptoms.38 Three patients who stopped taking thalidomide all experienced return of cough within 2 weeks but, with reinstitution, all three patients again had resolution of the cough.
QoL: SGRQ data showed a significant decrease on question 2 (cough question) between baseline and 3 months (4.9 (0.3) vs 2.2 (1.6), p=0.03).
Colchicine
A quasi-experimental open-label uncontrolled study of 17 patients with IPF showed improvement in dyspnoea of 1.7 units (as part of a composite clinical score) in 10 patients (significance not stated).17 The diagnostic criteria used were those of Turner Warwick et al41 and therefore patients are likely to include a mixed group. Of note, improvement in dyspnoea was also noted in the study by Fiorucci et al30 which compared colchicine with prednisolone and cyclophosphamide.
Doxycycline
6MWD: A quasi-experimental open-label uncontrolled trial of six patients with IPF showed no improvement in 6MWD.40
QoL: There was a significant improvement in QoL on the SGRQ total score after treatment with doxycycline (p<0.0001). However, other SGRQ scores were not presented or commented on in the paper.
Discussion
Patients with PIF-ILD suffer a high symptom burden2 and impaired QoL3 in the terminal stages of their disease. This systematic review aimed to present the evidence for the use of interventions to improve dyspnoea, other symptoms and QoL in PIF-ILD. We reviewed the symptom scales used in these interventions and sought to perform an economic evaluation of them.
While a recent review examining the treatment of dyspnoea in IPF recommends that sildenafil should be considered,42 we do not believe that there is sufficient evidence to support its use in improving dyspnoea. A Cochrane review of physical training for ILD43 that involved meta-analyses of RCT evidence for 6MWD, dyspnoea and QoL (and included some unpublished data) supported the use of pulmonary rehabilitation. However, our data, which include all types of studies, can only support the use of pulmonary rehabilitation in improving 6MWD and, to a lesser extent, QoL.
The minimum clinically important difference in 6MWD in patients with IPF has been reported as 24–45 m.44–46 Our analysis show that pooled data for both pulmonary rehabilitation and pirfenidone are within that range. Even though pulmonary rehabilitation improved 6MWD, the effect on dyspnoea was mixed. In addition, pirfenidone improved 6MWD but not dyspnoea.7 Interplay between functional capacity and dyspnoea at rest is complex and a clear correlation was not found. This may be because dyspnoea is a complex multifaceted problem47 which is not necessarily linked to functional capacity, or it may be that appropriate dyspnoea outcome measures were not used.
Although there is weak evidence for ambulatory oxygen, it is worth taking into account that a feature of pulmonary rehabilitation itself is to optimise the use of oxygen prior to proceeding with the programme. Therefore, oxygen may have been an important element of the intervention which adds to its positive effects.
Despite their widespread use, we could find only weak evidence for the benefit of steroids in improving dyspnoea and cough and no extractable or appropriate data on QoL. However, a number of studies were excluded (see appendix 3 online), largely due to mixed patient groups and a paucity of extractable symptom control or QoL data. Individually, it is possible that patients may experience a subjective improvement from a short course of low-dose steroids due to the mood and appetite-enhancing effects. In deciding whether to continue treatment, the subjective symptomatic benefit should be balanced with recent data48 and any potential side effect burden.
Our aim in this systematic review was to present the evidence for interventions which improved symptom control and QoL. However, the crucial distinction and essential dichotomy in considering these interventions is to classify them as radical or palliative. In using palliative interventions (eg, diamorphine), the only goal is to improve symptoms and QoL while, in using radical interventions (eg, pirfenidone), the primary goal is to slow disease progression with no adverse effect on symptoms or QoL. When considering the effect of radical treatments, the more important and currently realistic goal may be a stabilisation or slowing in the deterioration of symptoms and QoL. This in itself is important as stabilisation of disease may result in physiological and psychological adaptations which could result in improvement in symptom control and QoL over time.
For patients where radical treatments are being applied, a change in score within a patient group may not be a sensitive measure since the underlying efficacy of the treatment to slow or alter the rate of disease progression may be effective but mirrored by no change in symptom score which would otherwise have declined. For purely palliative interventions, an improvement in symptom experience is often the more meaningful outcome. For example, Zisman et al6 reported a non-significant change in dyspnoea with sildenafil treatment but presented data showing that there was less deterioration in the intervention group than in the placebo group. Conversely, many other radical interventions do not present these data and a non-significant change cannot be interpreted further. We would encourage authors to present this information clearly to facilitate a true interpretation of the impact of radical interventions on symptoms and QoL.
Our review has highlighted a number of important issues which limit comparison across studies. There was a paucity of RCTs (all were published in the last 10 years), very few studies were powered for QoL or symptoms as the primary outcome, there was poor reporting of data and mixed group studies did not report outcome measures separately. Despite some work at developing outcome scales specifically related to this disease group,49–51 we found poor use of validated outcome measures and a heterogeneity of measures used. Interestingly, in one study33 the quantitative results were contradictory to the qualitative results. We would recommend international consensus regarding patient-reported outcome measures and study methodology to ensure that future trials capture accurate symptom control and QoL data. In addition, future trials looking at symptoms and QoL outcomes should include a priori subgroup analysis of patients with severe symptoms and longitudinal analysis of subgroups in which radical interventions result in stable disease.
Patients with IPF experience increased healthcare resource utilisation and direct medical costs.52 As the population gets older, we can expect that the burden on healthcare will increase.52 We believe that timely and adequate symptom control may prevent unnecessary hospital admissions and therefore contain some expenditure. Interestingly, government funding provided only 6% of support for trials and over a quarter of studies had some source of industry funding. Studies which are funded by industry are unlikely to have symptoms and QoL as primary outcome measures, so the design of these studies may not be best to assess these outcome measures. In the absence of economic analysis of interventions, recommendations about future directions of government spending and conclusions about the resultant potential savings cannot be made.
Study limitations
Only one reviewer retrieved and chose papers. However, a number of sources including a multidisciplinary panel of experts in the ILD and palliative care fields were consulted to ensure that no known studies were missing. We included all study types and all studies regardless of whether PIF-ILD was diagnosed using ATS/ERS criteria.16 There were only a few studies for each outcome. However, we have only used high-quality studies in the meta-analyses and presented studies clearly to allow readers to draw their own conclusions.
This review presents respiratory physicians with the evidence for interventions in improving 6MWD, dyspnoea, other symptoms and QoL in patients with PIF-ILD.
Conclusions
There is strong evidence for the use of pulmonary rehabilitation and pirfenidone to improve 6MWD and moderate evidence for the use of sildenafil and pulmonary rehabilitation to improve QoL. The evidence for pulmonary rehabilitation in improving dyspnoea is mixed. There is weak evidence for oxygen, prednisolone, diamorphine, D-pencillamine, colchicine, interferon α, thalidomide and doxycycline which warrants further investigation. Future recommendations for research include consensus on the use of validated outcome scales, primary endpoints related to symptom control and QoL and economic evaluation of interventions. In addition, careful consideration should be given to how symptom control and QoL outcome measures are used and the presentation of data in radical versus palliative treatment contexts.
Acknowledgments
The authors thank Abdelhamid Benalia and Natalia Calanzani for translation work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online appendix
- Data supplement 3 - Online appendix
- Data supplement 4 - Online appendix
Footnotes
-
Contributors All authors were involved in conceiving the review. SB conducted the review. SB and JRR jointly extracted data. SB and JLP conducted analysis. SB, JRR, JLP and AUW drafted the paper. All authors reviewed a copy of the paper and had intellectual input into the final version.
-
Funding Funding was received from the Royal Marsden and Royal Brompton Palliative Care research fund which is funded from charitable sources. JLP is supported by the NIHR Biomedical Research Centre based at Guy's and St Thomas’ NHS Foundation Trust and King's College London.
-
Competing interests AUW is a member of the UK Intermune advisory board.
-
Provenance and peer review Not commissioned; externally peer reviewed.