Article Text

Statistics from Altmetric.com
Learning point
-
Cryptogenic OP may rarely present as a small airway-predominant disease causing severe airflow limitation and a ‘tree in bud’ pattern on HR-CT.
A 19-year-old man presented with dyspnoea, a non-productive cough and subfebrile temperature. Chest radiography showed a diffuse nodular pattern and a pneumomediastinum. HR-CT revealed a diffuse ‘tree in bud’ pattern (figure 1). An infectious bronchiolitis was suspected. Despite treatment with moxifloxacin he developed hypercapnic respiratory failure requiring mechanical ventilation. Extensive microbiological investigations did not reveal a pathogenic microorganism. Continued treatment with antibiotics, low-dose steroids and neomacrolides was not effective, and an open lung biopsy was performed. Histology showed an organising pneumonia (OP) with extensive endobronchiolar granulation tissue (figure 2). The treatment was converted to high-dose steroids upon which the patient improved rapidly. Spirometry performed shortly after intensive care discharge revealed a severe airflow limitation (FEV1 40% predicted). The patient eventually made a full recovery with near-normal spirometric test results on follow-up.
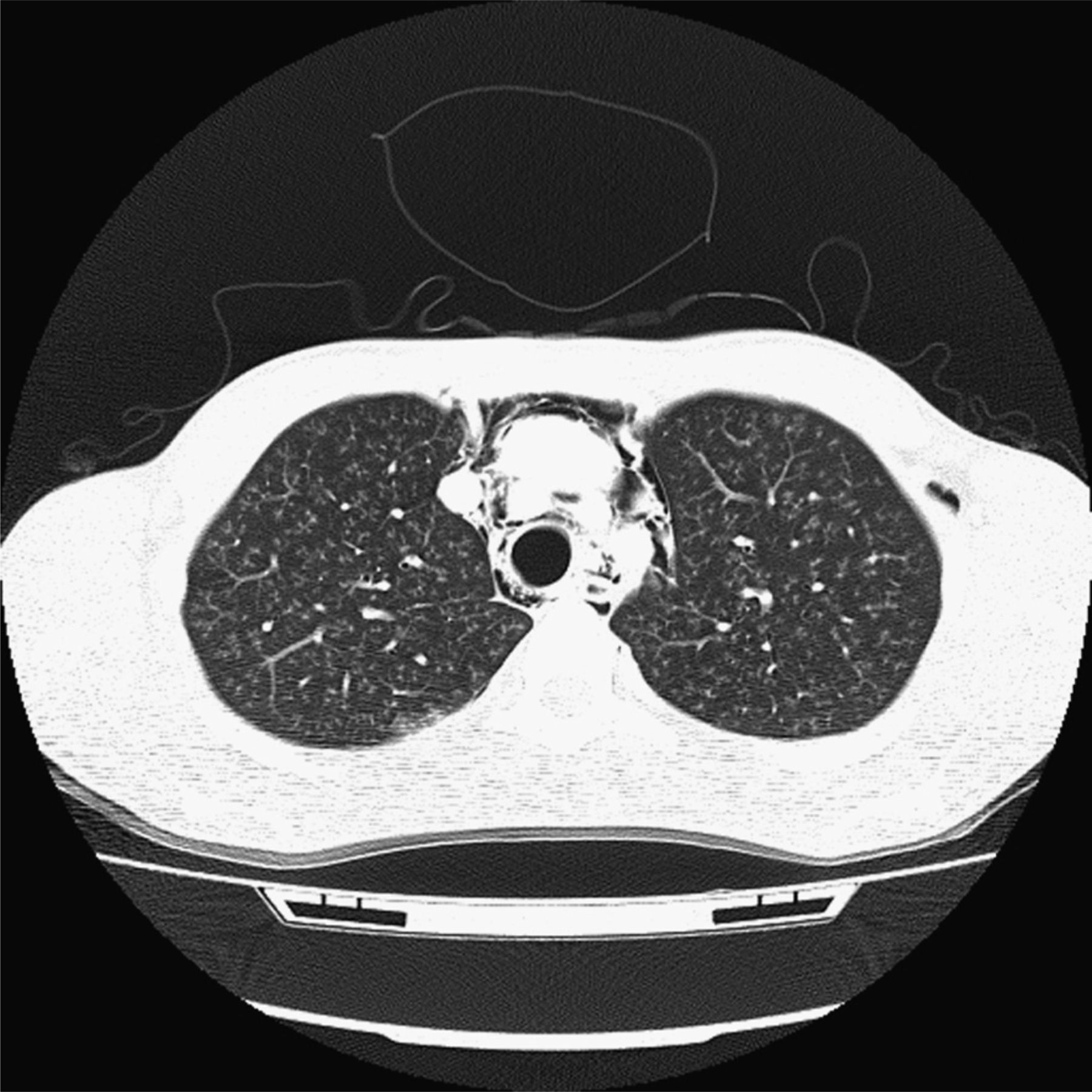
HR-CT scan shows multiple centrilobular nodules and branching linear opacities causing the tree in bud pattern next to a pneumomediastinum.

{kind=link}
{kind=link}
Histology of the open lung biopsy shows an organising pneumonia with extensive endobronchiolar granulation tissue (arrows). This figure is only reproduced in colour in the online version.
A tree in bud pattern on HR-CT correlates with filling of the small airways and respiratory bronchioles, usually with mucus and inflammatory cells. It is most commonly associated with infectious diseases affecting the bronchioles.1 OP resulting in a ‘tree in bud’ pattern has been previously suggested.2 However, a clear radiological-pathological correlation of OP filling the bronchioles resulting in a ‘tree in bud’ pattern has, to the best of our knowledge, not yet been clearly demonstrated. HR-CT patterns seen in OP are mainly characterised by consolidations in a bronchocentric pattern as the intraluminal plugs of granulation tissue are usually found within the alveolar ducts and surrounding alveoli. Frequently observed HR-CT patterns include multifocal peripheral parenchymal consolidations that tend to migrate, peribronchovascular consolidations and nodules.3
Although it is conceivable that the OP in our patient was triggered by an undetected pathogen or an unknown inhaled toxic substance, extensive investigations and enquiries did not yield an inciting agent. Furthermore, our patient did not display signs of a connective tissue disorder that has been associated with the development of both OP and a tree in bud pattern.1 ,3 After multidisciplinary evaluation of the case, a diagnosis of a Cryptogenic OP was made. This case report illustrates that a Cryptogenic OP can manifest with a ‘tree in bud’ pattern on HR-CT.
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Formal consultation with the Medical Ethical Committee of the Erasmus MC learnt that, under the Dutch act for medical research involving human subjects (Wet Medisch Onderzoek), approval of this case report by the Medical Ethical Committee is not required.
-
Provenance and peer review Not commissioned; externally peer reviewed.