Article Text

Abstract
Background Intravenous magnesium has been shown to cause bronchodilation in acute severe asthma and in small trials in acute exacerbations of chronic obstructive pulmonary disease (AECOPD). There is also some evidence of benefit from nebulised magnesium in acute severe asthma. Our hypothesis was that adjuvant magnesium treatment administered via repeated nebulisation was effective in the management of AECOPD.
Methods In this randomised double-blind placebo-controlled trial, we approached 161 patients with AECOPD presenting to the emergency departments at two New Zealand hospitals with a forced expiratory volume in 1 s (FEV1) <50% predicted 20 min after initial administration of salbutamol 2.5 mg and ipratropium 500 µg via nebulisation. Patients received 2.5 mg salbutamol mixed with either 2.5 ml isotonic magnesium sulphate (151 mg per dose) or 2.5 ml isotonic saline (placebo) on three occasions at 30 min intervals via nebuliser. The primary outcome measure was FEV1 at 90 min.
Results 116 patients were randomised, 52 of whom were randomly allocated to the magnesium adjuvant group. At 90 min the mean (SD) FEV1 in the magnesium group (N=47) was 0.78 (0.33) l compared with 0.81 (0.30) l in the saline group (N=61) (difference −0.026 l (95% CI −0.15 to 0.095, p=0.67). No patients required non-invasive ventilation. There were 43/48 admissions to hospital in the magnesium group and 56/61 in the saline group (RR 0.98, 95% CI 0.86 to 1.10, p=0.69).
Conclusions Nebulised magnesium as an adjuvant to salbutamol treatment in the setting of AECOPD has no effect on FEV1.
Australian New Zealand Clinical Trials Registry ACTRN12608000167369.
- COPD Exacerbations
- COPD Pharmacology
Statistics from Altmetric.com
Key messages
What is the key question?
-
Is there a role for nebulised magnesium treatment in the management of acute exacerbations of chronic obstructive pulmonary disease (AECOPD)?
What is the bottom line?
-
Both single and repeated doses of nebulised magnesium, as an adjunct to nebulised salbutamol treatment in the setting of AECOPD, have no effect on FEV1.
Why read on?
-
Intravenous or nebulised magnesium is attractive as a bronchodilator because it is relatively cheap and has minimal side effects. There is an ongoing interest in a possible therapeutic role for intravenous or nebulised magnesium in obstructive airways disease. The result of this randomised double-blind placebo-controlled trial in AECOPD is discussed in the context of available evidence.
Introduction
Magnesium has a key role in numerous physiological processes.1 ,2 Important underlying mechanisms of action of magnesium include calcium antagonism via calcium channels, regulation of energy transfer (such as the production and function of ATP) and membrane stabilisation.1 ,2 In the airways, magnesium is a bronchodilator through various mechanisms including an inhibitory effect on bronchial smooth muscle contraction mediated by calcium3 and an inhibitory effect on acetylcholine release from cholinergic nerve terminals4 and histamine from mast cells.3
Experimental studies have variably demonstrated a benefit of magnesium in acute severe asthma since the first report over 50 years ago.5 Magnesium has been administered via the intravenous route6–10 and via nebuliser,11–14 with interest in the latter route of administration because of practical and potential safety advantages. In a randomised double-blind placebo-controlled trial, we have previously shown that isotonic nebulised magnesium sulphate results in an enhanced bronchodilator response in severe exacerbations of asthma.13 However, fewer studies have addressed the effects of magnesium in chronic obstructive pulmonary disease (COPD)15–20 even though asthma and COPD share some pathophysiological characteristics (such as bronchial hyper-responsiveness) as well as numerous therapies, particularly bronchodilator treatments.
We are aware of reports of only six studies investigating the bronchodilator efficacy of magnesium sulphate in COPD. Three studies have reported the efficacy of intravenous magnesium in the setting of acute exacerbations of chronic obstructive pulmonary disease (AECOPD), improving patient symptoms and reduced length of stay,15 increasing peak expiratory flow16 and increasing forced expiratory volume in 1 s (FEV1).19 This last study only showed an effect as an adjunct to inhaled β2 agonists. A fourth study combined one intravenous bolus of magnesium with repeated nebulised magnesium and terbutaline. There was no difference in the primary combined outcome of hospital admission, intubation and hospital death rate compared with terbutaline and ipratropium.20 However, the terbutaline and ipratropium group showed a greater improvement in peak expiratory flow. Two studies in stable COPD have been undertaken, reporting a reduction in hyperinflation with intravenous magnesium17 and an increase in FEV1 when magnesium was added to nebulised salbutamol.18
Nebulised magnesium is attractive as a therapeutic option because it is easily administered, relatively cheap and has minimal side effects. In light of some evidence for an effect when nebulised in severe exacerbations of asthma, the similarities between asthma and COPD (especially with regard to bronchodilator therapy) and the practical advantages of administration via nebuliser, we sought to focus on the nebulised route of delivery in AECOPD. Our hypothesis was that adjuvant magnesium treatment administered via nebuliser was effective in the management of patients with AECOPD.
Methods
Participants
Patients with an AECOPD who presented to the emergency departments (EDs) of two university hospitals in New Zealand (Wellington Regional Hospital and Hutt Hospital) were invited to participate in the study between June 2008 and November 2011, if a study investigator was available. Inclusion in the study required age ≥35 years, a doctor diagnosis of COPD, ratio of the FEV1 to forced vital capacity (FVC) (FEV1/FVC) <70% and an FEV1≤ 50% predicted 20 min after initial treatment with 2.5 mg salbutamol and 500 µg ipratropium bromide by nebulisation. We excluded patients if they required intubation or non-invasive ventilation (NIV), were unable to perform spirometry or had evidence of pneumothorax, hypotension, any other serious medical condition that would prevent their participation in the trial or were pregnant.
Study protocol
On presentation to the ED with a provisional diagnosis of an AECOPD, potential subjects were clinically assessed and received standard initial treatment (ie, 2.5 mg salbutamol and 500 µg ipratropium bromide by jet nebulisation and 40 mg prednisone). Oxygen (2 l/min nasal prongs) was given if oxygen saturations on room air were <90%. Only subjects with an FEV1≤ 50% predicted measured 20 min after commencement of the initial salbutamol/ipratropium nebulisation were enrolled in the trial. During this 20 min period informed consent was obtained and a brief questionnaire administered, obtaining information with regard to duration and severity of symptoms, medication use and smoking status. Routine blood tests (creatinine, sodium, potassium, full blood count) were done, as well as a serum magnesium level. After randomisation, patients received by jet nebulisation 2.5 mg salbutamol (GlaxoSmithKline, London, UK) mixed with 2.5 ml isotonic magnesium sulphate (250 mmol/l, tonicity 289 mosmol; 151 mg per dose) or 2.5 ml isotonic saline (placebo) on three occasions at 30 min intervals. The majority of nebulisers were driven by air, 14 patients received supplemental oxygen via nasal prongs during the nebuliser (1–2 l/min) and 21 had their nebuliser driven by oxygen (6 l/min), most commonly because medical air was not available.
We recorded FEV1 (and FVC) using a hand-held spirometer (Micro Medical, Rochester, Kent, UK) on first referral (‘presentation’ FEV1), before the first study nebuliser (‘baseline’ FEV1), before each subsequent nebulisation and then 30 min after the last nebule. Three measurements were made at each time point and the highest recording used for analysis. All those performing spirometry received training from a respiratory scientist. Pulse oximetry was done as part of routine clinical observations (blood pressure, pulse, respiratory rate) and otherwise as clinically indicated. After the final recordings the decision to admit the patients was made at the discretion of the clinical team.
Randomisation and masking
Patients were randomly allocated in a double-blind fashion to receive one of two treatment regimens. The study statistician performed block randomisation with a block size of eight using a computer-generated random sequence. This was administered by a third-party process so that participants and investigators were unaware of treatment allocation through provision by the hospital pharmacy of pre-prepared identical syringes containing the study drug or placebo according to this random allocation.
Statistical analysis
Analysis was by intention-to-treat. The primary outcome was FEV1 at 90 min. Secondary outcomes were FEV1 at 30 and 60 min, hospital admission, episodes of NIV and admission to ICU.
The significance level was set at p=0.05. The primary analysis was a t test comparing FEV1 between the randomised groups at 90 min. Secondary analyses were t tests to compare FEV1 at 30 and 60 min as well as ANCOVA with adjustment for baseline FEV1. The calculation of relative risk of the secondary categorical outcome measurements with appropriate CIs was planned but, in the event, there were no episodes of NIV or ICU admissions and this could only be calculated for hospital admissions. An exploratory analysis of the relationship between the change in FEV1 and serum magnesium was carried out using simple correlation coefficients and ANCOVA. SAS V.9.2 (SAS Institute, Cary, North Carolina, USA) was used for the analysis.
The planned sample size of 200 participants was estimated based on the SD of the FEV1 at the last measurement time from our previous study.13 In that study, the difference between the mean FEV1 in the magnesium group (1.94 l) and in the saline group (1.58 l) was 0.36 l with a pooled SD of 0.74 l. To detect an absolute difference in FEV1 of 0.30 l at an α of 5% and a power of 80% required 194 subjects in a two-arm trial.
Results
One hundred and sixty one patients were assessed between May 2008 and December 2011. Following exclusion of 45 patients, 116 patients were randomised (figure 1). The reasons for exclusion included not meeting the inclusion criteria (lack of formal COPD diagnosis, significant other comorbidity such as pneumonia and congestive heart failure, receiving NIV on arrival at the ED, FEV1>50% predicted post-bronchodilator), declined to participate and other (eg, unable to consent secondary to language barrier or dementia, unable to perform adequate spirometry, given intravenous magnesium by ED staff).
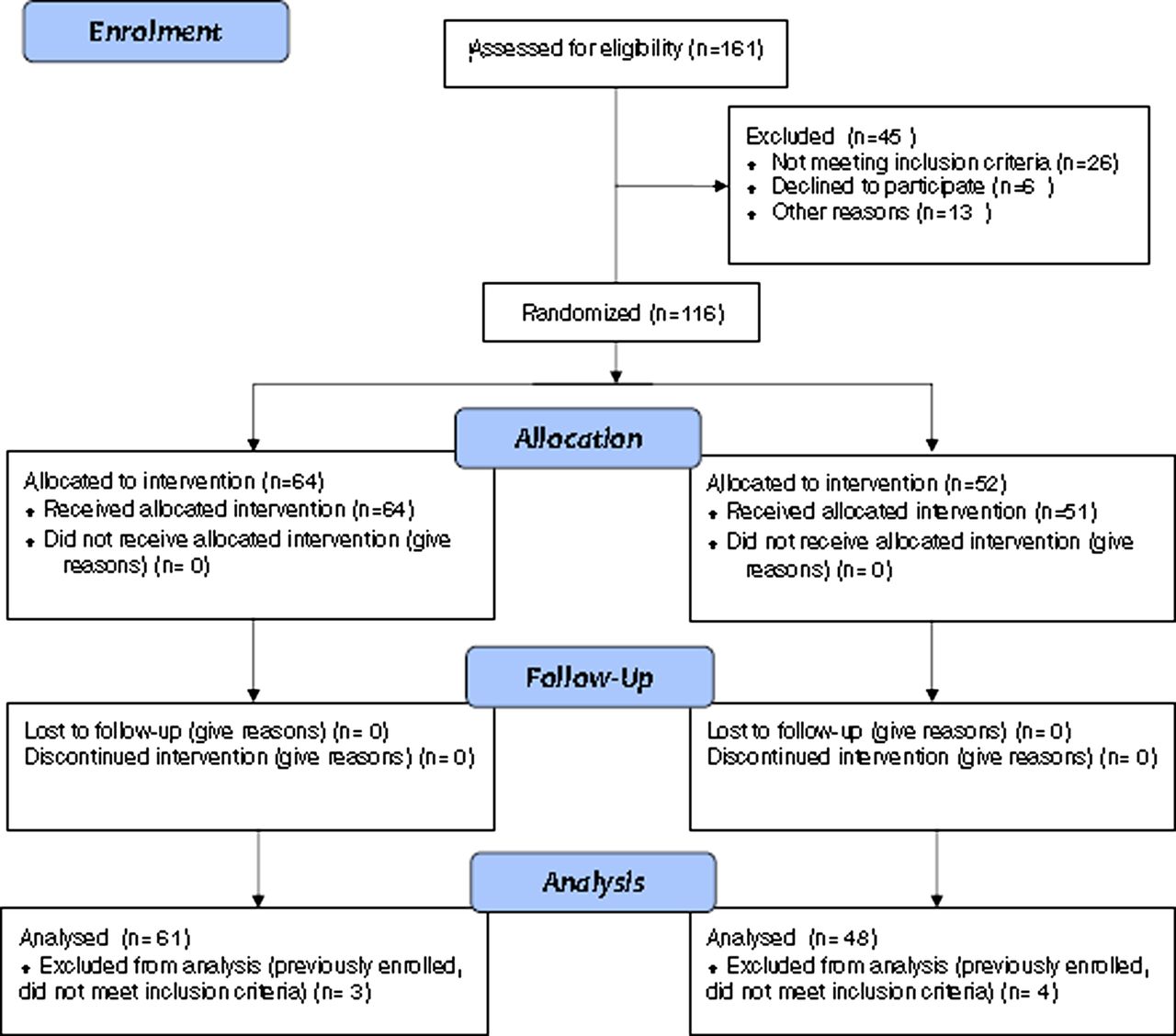
Consort trial profile. This figure is only reproduced in colour in the online version.
Of the 116 remaining patients, 52 were randomly allocated to the magnesium adjuvant group. Two patients in the placebo group and three in the magnesium group were inadvertently enrolled twice and the second presentation was excluded from the analysis (five events). Two other patients were excluded prior to analysis because of an inaccurate calculation of the percentage predicted FEV1 and initial failure to recognise pneumonia as the primary diagnosis.
Table 1 shows the baseline characteristics of the 109 patients included in the analysis. The denominator for some of the characteristics varies due to missing data for eight patients (five in the placebo group and three in the magnesium group). The mean age was 71 years (range 36–89); 53% were men and 40% were current smokers. Nearly 20% were on domiciliary oxygen and the average number of admissions in the last year was one. Mean (SD) FEV1 on arrival was 0.71 (0.25) l (range 0.15–1.43 l). The proportion of patients with an FEV1 on arrival of >1000 ml was 8/48 (16.7%) in the magnesium group and 6/61 (9.8%) in the placebo group.
Baseline characteristics of patient group
Serial forced expiratory volume in 1 s (FEV1) in patients receiving nebulised magnesium or placebo
For the primary outcome variable, FEV1 at 90 min (30 min after the third administration of the study drug), the mean (SD) FEV1 in the magnesium group (N=47) was 0.78 (0.33) l compared with 0.81 (0.30) l in the saline group (N=61), difference −0.026 l (95% CI −0.15 to 0.095, p=0.67). After adjustment for baseline FEV1 the difference was −0.024 l (95% CI −0.07 to 0.026), p=0.34 (see table 2).
For FEV1 at 30 and 60 min, ANCOVA showed an adjusted difference of −0.043 l (95% CI −0.08 to −0.009, p=0.014) and −0.042 l (95% CI −0.08 to −0.007, p=0.02) respectively (ie, FEV1 was lower in the magnesium group after adjustment for baseline). No patients required NIV and there were no ICU admissions in either group. There were 43/48 (89.6%) admissions to hospital in the magnesium group and 56/61 (91.8%) in the saline group (RR of admission for magnesium vs placebo group 0.98, 95% CI 0.86 to 1.10, p=0.69).
Reversibility (based on absolute change in FEV1 of at least 200 ml and >12% change from baseline using 90 min and baseline FEV1) by randomised group was as follows: 5/47 (10.6%) in the magnesium group vs 6/61 (9.8%) in the placebo group (RR 1.08, 0.35 to 3.33, p=0.89). One participant in the magnesium group had missing 90 min FEV1 data.
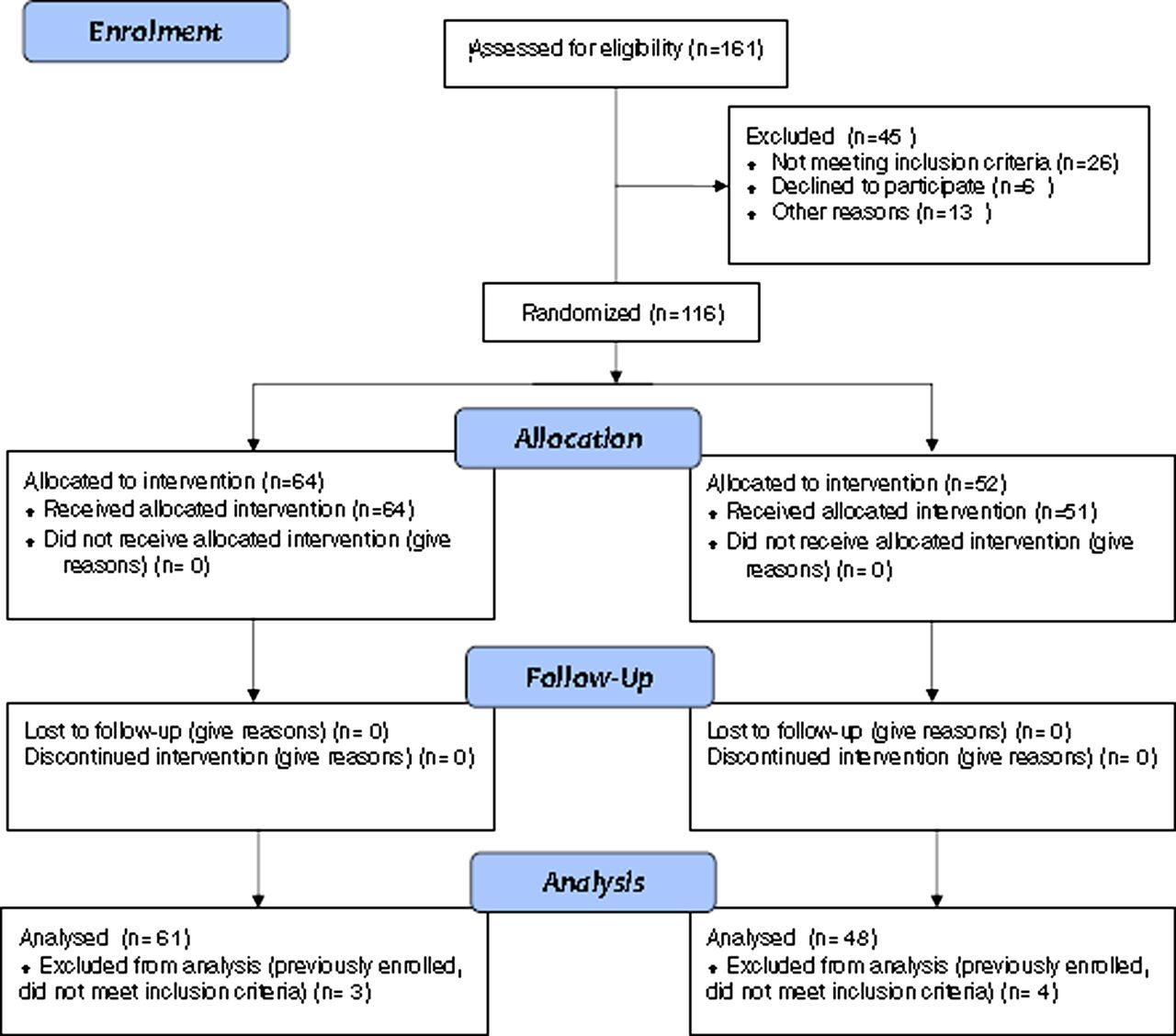
Baseline serum magnesium levels ranged from 0.45 to 0.97 mmol/l (normal reference range 0.76–0.99 mmol/l). There was no evidence that serum magnesium levels influenced the FEV1 response (p for interaction=0.51), and the common correlation coefficient for the association between change in FEV1 at 90 min and time zero was 0.17 (p=0.13, N=77 with complete data; figure 2).

{kind=link}
{kind=link}
Change between forced expiratory volume in 1 s (FEV1) at baseline and at 90 min in relation to magnesium level (open symbols represent magnesium, closed symbols represent placebo).
No clinically significant adverse events were reported and no patients in either group needed additional bronchodilator therapy within the 90 min time period or were withdrawn because of clinical deterioration.
Discussion
In this randomised double-blind placebo-controlled trial we were unable to demonstrate any clinical benefit with single or repeated administration of nebulised magnesium given as an adjunct to bronchodilator treatment on presentation to hospital with an AECOPD. In this study, the largest to date of nebulised magnesium in COPD, we were also unable to show any evidence of a relationship between serum magnesium, change in FEV1 and randomised treatment group.
We considered several methodological issues in the design of the study that are relevant to its interpretation. The primary reason for including only subjects with an FEV1<50% predicted (measured 20 min after commencement of initial salbutamol and ipratropium) was that, in groups with asthma, an effect with intravenous magnesium has been found in those with more severe disease.10 FEV1 was chosen as the primary outcome variable as a sensitive, objective and repeatable measure of bronchodilator response in AECOPD.21 ,22 Specifically, the administration of a bronchodilator during AECOPD can increase the FEV1 and the FVC by 15–29% over a period of 60–120 min.23
With regard to the protocol of bronchodilator administration, the reason for the initial salbutamol/ipratropium nebulisers at presentation was safety as well as ensuring some standardisation of bronchodilator treatment in the 20 min prior to randomisation. Guidelines for managing an AECOPD generally agree that bronchodilators are considered first-line treatment24–26 but may not recommend a specific dose. In stable COPD it has been shown that 88% of patients achieved 90% of maximal bronchodilation with doses of inhaled salbutamol ≤1.2 mg.27 It could be argued that this pre-dosing with bronchodilators meant patients had already reached their maximum bronchodilator response before administration of magnesium. Additionally, the combination of ipratropium and salbutamol is known to be superior to either agent alone.28 ,29 The magnesium used was formulated as an isotonic solution. This was important because both hypotonic and hypertonic nebuliser solutions can induce bronchoconstriction in patients with bronchial hyper-responsiveness.30
Recruitment proved difficult with 109 of a planned 200 patients studied, despite the extension of the study by 10 months. However, the study had equivalent power to that planned due to the smaller SD for FEV1 in the study compared with that used in the power calculations (based on our previous study of nebulised magnesium in acute severe asthma).13 This resulted in 95% CIs that excluded the pre-nominated clinically important difference. The reason for the unequal numbers in the two groups was that the batches of magnesium and placebo provided by the hospital pharmacy were often incompletely used before expiring and a new batch being issued. Also, we recruited a group with severe airflow obstruction with a mean FEV1 of 0.74 l.
The findings of this study raise a number of points for discussion. The first is the relation of this study to other studies of magnesium in COPD. There are only six placebo-controlled trials involving intravenous15–17 ,19 or nebulised18 magnesium or both20 in either acute exacerbations15 ,16 ,19 ,20 or in the stable outpatient setting,17 ,18 and three are in abstract form only.15 ,18 ,19
In two that involve intravenous magnesium in the setting of AECOPD,15 ,16 1.2 g was administered following standard nebulised bronchodilator treatment. In their randomised double-blind placebo-controlled trial of 24 subjects with an AECOPD, Hogg et al15 reported a significant reduction in the Modified Borg Dsypnoea Score 30 min after the start of the infusion (2.33 vs 1.08, p<0.01) and a reduced length of inpatient stay in the intravenous magnesium group compared with placebo (4.27 vs 7.33 days, p<0.05). In their randomised double-blind placebo-controlled trial of 72 subjects with AECOPD, Skorodin et al16 reported a significant increase in peak expiratory flow from initiation to 30 and 45 min later (25.1 vs 7.4 l/min, p=0.03) and a statistically non-significant trend towards a reduced need for hospitalisation with intravenous magnesium. Abreu Gonzalez et al administered either 1.5 g of magnesium (intravenous) or placebo on the first day and then vice versa on the other day in a randomised double-blind crossover design of 24 patients. Salbutamol was administered 45 min after the placebo or magnesium. The mean increase in FEV1 was 0.18 l compared with 0.081 l after placebo (p=0.004). Interestingly, this bronchodilating effect was only observed after salbutamol administration.19
In a randomised double-blind placebo-controlled trial of 22 subjects with stable COPD, Do Amaral et al17 reported that an intravenous infusion of magnesium sulphate resulted in a significant reduction in lung hyperinflation measured as functional respiratory capacity (−0.53 vs −0.05 l, p=0.04) and an increase in respiratory muscle strength measured as maximum inspiratory pressure (6.9 vs −3.1 cm H2O, p=0.02). Together these studies indicate that a single intravenous dose of magnesium has clinical efficacy in both stable and acute exacerbations of COPD.
More recently, Nouira et al randomised 62 patients presenting to the ED with an AECOPD to receive either multiple nebulisations of terbutaline plus ipratropium or terbutaline plus a once-only bolus of intravenous magnesium (1.5 g) followed by repeated nebulised terbutaline and nebulised magnesium (150 mg/nebule). There was no significant difference between the two groups in their primary outcome variable (which included hospital admission, intubation and hospital death rates). Patients given ipratropium (and terbutaline) had an average improvement in peak expiratory flow of 32 l/min (95% CI 19 to 43) compared with the magnesium group. Their reason for combining an intravenous bolus and repeated nebulisations was to ensure an adequate dose but to avoid potentially toxic blood levels.20
The only other study of nebulised magnesium investigated its effect in patients with stable COPD recruited from outpatients. The group that received magnesium as an adjunct to nebulised salbutamol showed a significant increase in FEV1 from 1.44 l to 1.67 l at 60 min (p<0.05).18 However, this study does not appear to have been randomised or double-blind and was inadequately powered with only 18 patients studied. It is difficult to reach any conclusion about nebulised magnesium in COPD on the basis of this trial. We propose that our randomised double-blind placebo-controlled design and greater power provide a higher level of evidence that nebulised magnesium as an adjunct to salbutamol treatment in the setting of AECOPD had no effect.
The second point is consideration of our findings in relation to the asthma literature. This is relevant because the reported efficacy of magnesium in asthma exacerbations is the pretext for its use in COPD. In asthma, magnesium has been administered both intravenously and via the nebulised route. The recent Cochrane review and meta-analysis of intravenous magnesium reported an improvement only in the severe subgroup in whom peak expiratory flow improved by 52.3 l/min (95% CI 27 to 77.5) and FEV1 by 9.8% predicted (95% CI 3.8% to 15.8%).10 However, the Cochrane review of nebulised magnesium as an adjunct in acute asthma reported a non-significant improvement in pulmonary function in the nebulised magnesium group, but significant heterogeneity between trials precluded a definitive conclusion.14
This leads on to the third point, which concerns route of administration. Although individual trials in acute asthma, including our own, may show some benefit with nebulised magnesium,12 ,13 this was not conclusively shown in the meta-analysis14 and the efficacy of this route must remain in question. The benefits of repeated administration of nebulised magnesium include ease of administration with no need for an intravenous line. With regard to the dose of magnesium, this was based on the work in asthma.13
The fourth point for discussion, and related to the patient group, is that of the definition of asthma versus COPD and the spectrum of obstructive airways disease, particularly in the older age group. Increasingly, the complexity and heterogeneity of these conditions is recognised31 ,32 and better definition of the patient group who may respond to magnesium may be crucial in clarifying its therapeutic effect.
The fifth point concerns the association between serum magnesium levels and COPD.33–35 Aziz et al retrospectively reviewed charts of 50 patients with stable COPD and 50 with an AECOPD. Those in the latter group had significantly lower magnesium levels.35 Bhatt et al34 also retrospectively reviewed magnesium levels and readmission rate and death in 100 patients with AECOPD. The sole predictor of frequent readmissions was low serum magnesium. Rolla et al measured magnesium levels in a group of 95 with severe but stable COPD; 11% had hypomagnesaemia and there was a significant inverse relationship between serum magnesium and the use of diuretics or length of oral steroid treatment. The authors concluded that serum magnesium should be routinely checked because of potential negative effects on respiratory muscle power.33 Earlier work has shown that correction of hypomagnesaemia is associated with improved respiratory muscle power.36 Interestingly, we did not find any relationship between serum magnesium, change in FEV1 and randomised treatment group. We are aware of one study that has characterised metallic elements in exhaled breath condensate and serum as novel biomarkers of exposure and susceptibility in AECOPD. Corradi et al found that exhaled magnesium levels were 50% higher in an exacerbation than at recovery (but there was no change in serum level). Manganese was the only other metallic element to show a similar pattern.37 The meaning of this is unclear; perhaps the high local magnesium levels in the airways explain why there is no great response to nebulised magnesium.
In conclusion, this randomised double-blind placebo-controlled trial has shown no evidence of efficacy of single or repeated nebulised magnesium as an adjunct to nebulised salbutamol in AECOPD. Our findings, together with previous studies, suggest that the priority for further investigation of magnesium in AECOPD should be with the intravenous route of administration.
Acknowledgments
We thank staff at the emergency departments of Wellington and Hutt Hospitals New Zealand and the Pharmacy Staff at Wellington Hospital. Particular thanks are due to research fellows at the Medical Research Institute of New Zealand (who comprise the rest of the Magnesium COPD Study Team) who helped staff the roster. They are Dr Kyle Perrin, Dr Meme Wijesinghe, Dr Janine Pilcher, Dr Mitesh Patel, Dr James Fingleton, Dr Laird Cameron. Thanks are also due to the Medical Registrars at Wellington Hospital who also helped out on occasion.
References
Footnotes
-
Contributors The study was designed by RB, MW and PS. LE and PS coordinated the study and collected the data with KW, BH and SJ. MW assisted with the statistical analysis. PS and RB wrote the report with help from the other authors.
-
Funding The study was funded by the Health Research Council of New Zealand.
-
Competing interests None.
-
Ethics approval The trial was approved by the Central Regional Ethics Committee and written informed consent was obtained from all patients.
-
Provenance and peer review Not commissioned; internally peer reviewed.