Article Text

Abstract
Objectives To address whether the effect of BCG vaccination against tuberculosis (TB) infection lasts to adulthood.
Methods A cross-sectional study on the prevalence of latent TB infection (LTBI) among HIV-negative men, using QuantiFERON-TB Gold In-tube (QFT-IT), was conducted at a prison in northern Taiwan with >3000 inmates. A QFT-IT ≥0.35 IU/ml was defined as LTBI. A QFT-IT ≥0.7 IU/ml was defined as recent LTBI. The association between the number of BCG scars and LTBI stratified by age was analysed. The study procedure was approved by the institutional review board, and all participants gave written informed consent before receiving screening tests.
Results Among the 2385 participants, 25% had a QFT-IT ≥0.35 IU/ml. Increasing LTBI (14%, 32% and 50%) was observed with increased age (18–34 years, 35–54 years and ≥55 years) (p<0.001 by the Cochran–Armitage Trend Test). The number of BCG scars were found to be inversely correlated with QFT-IT results for both LTBI and recent LTBI in all three age groups (p<0.001 by Cochran–Mantel–Haenszel statistics).
Conclusions Our results suggest that BCG vaccine seems to have a protective effect in adults decades after vaccination according to the number of recent infections (QFT-IT ≥0.7 IU/ml). This finding has important implications for national policy of BCG vaccination. Further prospective cohort studies on the protective effect of BCG vaccination against TB infection in adults are warranted.
- Not Applicable
Statistics from Altmetric.com
Key messages
What is the key question?
-
Does the effectiveness of BCG vaccine on latent TB infection last into adulthood?
What is the bottom line?
-
There is an inverse correlation between the number of BCG scars and the prevalence of positive QFT-IT in all three age groups (18–34, 35–54 and ≥55 years). which indicates a lasting protective effect of BCG against TB infection into adulthood.
Why read on?
-
This finding has important implications for the national policy of BCG vaccination.
Introduction
The Bacillus Calmette–Guerin (BCG) vaccine was developed 90 years ago.1 BCG vaccine has a documented protective effect against tuberculosis (TB) meningitis and disseminated TB in children, and is used as a complementary strategy for TB control.2 ,3 Greater than 80% of neonates and infants are covered by BCG in countries where the vaccine is part of the national childhood immunisation programme.4
However, the protective effect of BCG against pulmonary TB in previous studies remains controversial. A long-term follow-up study in Native Americans and two studies of cohorts in Brazil and the UK demonstrated 48%–59% protection against TB from BCG vaccine 10–50 years after vaccination in newborns, schoolchildren and the community.5–7 Nevertheless, no evidence of substantial protection against TB from BCG vaccine was observed among schoolchildren and young adults in several randomised, controlled trials in the US State of Georgia and in Chennai, South India.8 ,9 Environmental mycobacteria exposure, differences between BCG strains used, genetic susceptibility and several other factors have been proposed as possible reasons for variable efficacy.1 ,10
In immunocompetent individuals, TB infection often has an initial latent phase, in which the spread of TB bacilli is contained by the immune system and the subjects remain asymptomatic.11 In these patients, progression to symptomatic TB disease occurs only after the breakdown of this containment.12 Measuring BCG impact on latent TB infection (LTBI) may provide insight on the protective effect of BCG against the initial stage of TB pathogenesis.
Before the development of the interferon gamma release assay (IGRA) in early 2000, the tuberculin skin test (TST) was the only diagnostic tool for LTBI. Nevertheless, BCG vaccine per se can yield a false positive TST that complicates interpretations as evidenced by the discordance between TST and IGRA in persons who had received BCG.13 The arrival of IGRA provides a specific diagnostic tool for LTBI in BCG vaccinees.14 IGRA was used as an indicator for LTBI in children in Turkey in a 2005 study that demonstrated a 40% efficacy of BCG against LTBI.15 One outbreak investigation in a nursery for 2- to 5-year-old children in the UK revealed that BCG vaccination provided 66% protection from infection.16 Does the same protective effect against LTBI from BCG vaccination also hold true in adults who received BCG vaccine after infancy? How long can BCG protect vaccinated individuals from LTBI? There are currently no answers for these questions.
The first BCG used in Taiwan was a liquid vaccine from an old Pasteur strain, which was certified by WHO and provided to TST-negative schoolchildren after 1953.17 BCG vaccine was subsequently changed, first to a new Pasteur strain in 1956 and then to a freeze-dried vaccine manufactured from the Japan Tokyo 172 strain in 1979. Since 1965, BCG has been provided to all infants and TST-negative schoolchildren.17 Revaccination of schoolchildren was halted in 1997 per WHO recommendation.18
To survey the prevalence of LTBI and its risk factors in adult prison inmates, a group vulnerable to TB transmission, the Centers for Disease Control, Taiwan (Taiwan CDC) provided a voluntary and free LTBI screening programme (including both TST and IGRA) to inmates at a prison in northern Taiwan.19 Among the inmates who agreed to participate, we analysed the effects of BCG vaccination on the prevalence of LTBI. We hypothesise that if BCG protects vaccinated individuals from TB infection, then in a cross-sectional LTBI survey stratified by age groups, we should observe an inverse association between the number of BCG inoculations and the prevalence of LTBI as determined by IGRA.
Materials and methods
Study setting
Participants were enrolled from April to October 2008, from a prison near Taipei, Taiwan, that is capable of accommodating 3000 adult male inmates. The turnover of inmates in and out of the prison is high. Up to 300 new inmates arrive at this prison every 4 weeks.
Ethics
The institutional review board of the National Taiwan University Hospital reviewed and approved the study protocol (No. 200707047M). The screening was not compulsory. All participants gave written informed consent before receiving screening tests. Any active TB cases identified in this study were offered appropriate anti-TB drug therapy. Participants found to have LTBI by this study were also offered the option to receive LTBI treatment.19
Eligibility
HIV-negative inmates without active TB who understood the screening programme and who gave informed consent were enrolled. HIV-positive inmates were enrolled in another study. The exclusion criteria were as follows: inmates who had a prison term less than 6 months, who had received complete treatment for TB, or who had evidence based on a chest radiograph suggesting active TB.
Evaluation for active TB disease
All inmates were routinely offered a chest radiography evaluation and HIV testing upon their arrival at the prison. The frequency of chest radiography screening for new inmates was once per month.20 Inmates who had not yet completed screening radiographies were isolated from the other inmates. Sputum cultures for mycobacteria were used to exclude active TB when there were suspicious chest radiography findings or symptoms. Chest radiography was provided to all participants who decided to receive the screening in our study, and the procedure of excluding active TB diseases was the same as the above process of sputum collections.
Evaluation for LTBI
The TST with purified protein derivative (RT 23 2 TU, Statens Serum Institute, Copenhagen, Denmark) and the QuantiFERON-TB Gold In-tube test (QFT-IT, Cellestis Ltd., Carnegie, Victoria, Australia) were conducted with the flow of drawing blood first, followed by performance of TST. The transverse induration size of the TST was read by the nurses who administered the test between 48 and 72 h after administration. Experts from the TST training committee double-checked the reading result of both BCG scars and the TST as part of a biannual training programme. A TST≥10 mm (according to the Taiwan guidelines of TB diagnosis and treatment) and a QFT-IT ≥0.35 IU/ml (according to the rules of the manufacturers) were defined as positive.21 When analysing the association between the number of BCG scars and the TB infection risk, we further defined cases of recently acquired LTBI (recent LTBI) using a cut-off point of QFT-IT ≥0.7 IU/ml. After acquisition of LTBI, the risk for progression to active TB is the highest in the first 2 years.22 In parallel, a higher level of IFN-γ response corresponds to a higher risk for progression to active TB,23 ,24 which indicates that a high IFN-γ response may be used as a marker for recent LTBI in immunocompetent persons. We chose 0.7 IU/ml as the cut-off value for recent LTBI because studies on serial testing of healthcare workers showed 0.35–0.7 IU/ml to be an uncertainty zone for recent TB infection.25 ,26
Number of BCG inoculations
The number of BCG scars was counted immediately prior to administration of the TST by trained public health nurses. Because there was no record of BCG immunisation in this study, we used BCG number as a proxy for previous BCG vaccination.
Statistical analysis
We compared categorical data by using the Pearson χ2 or Fisher exact tests, as appropriate. When analysing the association between the number of BCG scars and the TB infection risk, 2×N tables were analysed by the Cochran–Armitage trend test. Age-stratified analysis for the number of BCG scars and the TB infection risk was summarised by Cochran–Mantel–Haenszel statistics. The κ value and agreement were calculated to compare the concordance of TST (three cut-off values) and QFT-IT (LTBI and recent LTBI). All analyses were conducted by using SAS, V.9.1 software (SAS Institute, Cary, North Carolina, USA).
Role of the funding source
The sponsor of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report. The corresponding authors have full access to all the data in the study and have final responsibility for the decision to submit for publication.
Results
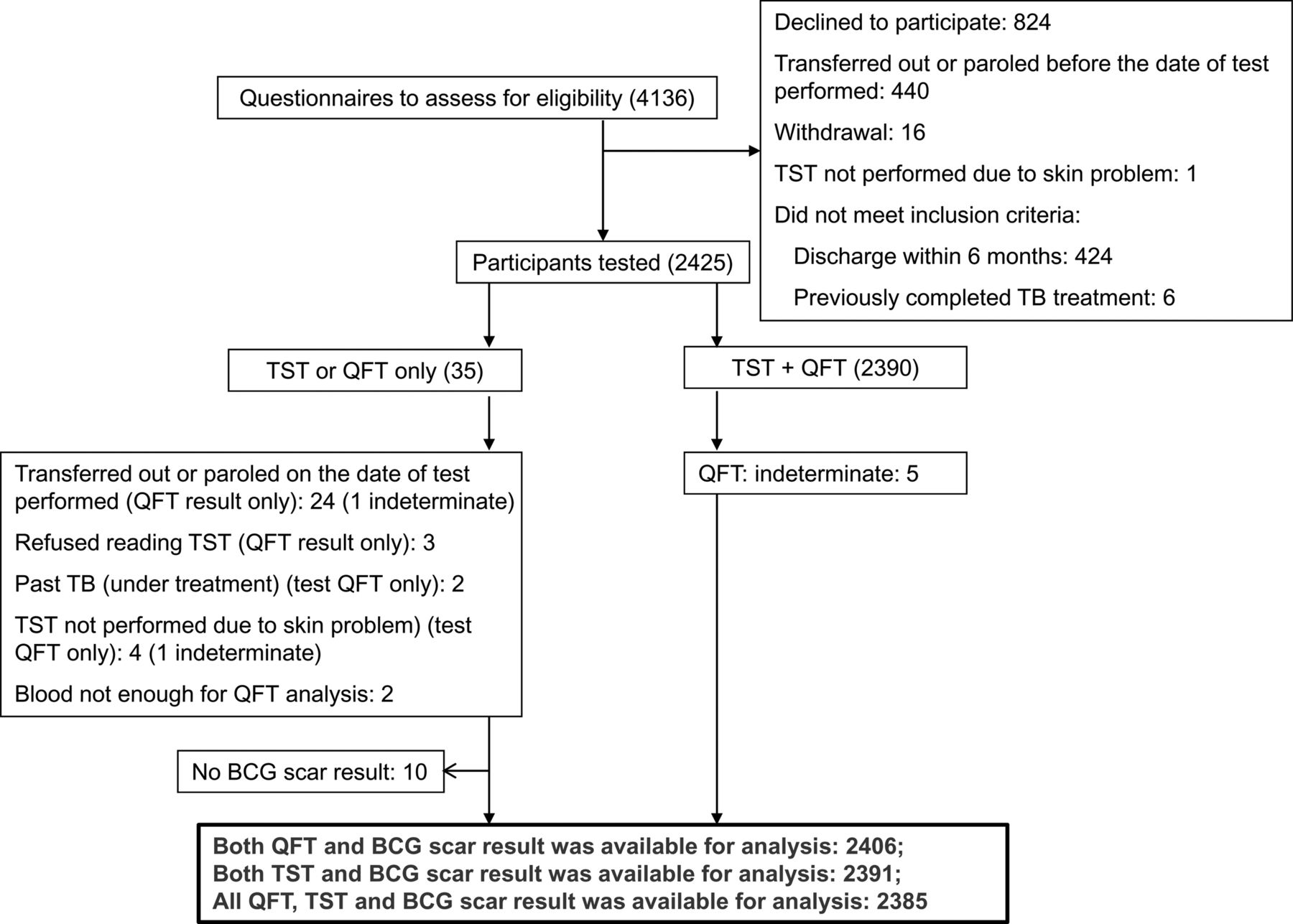
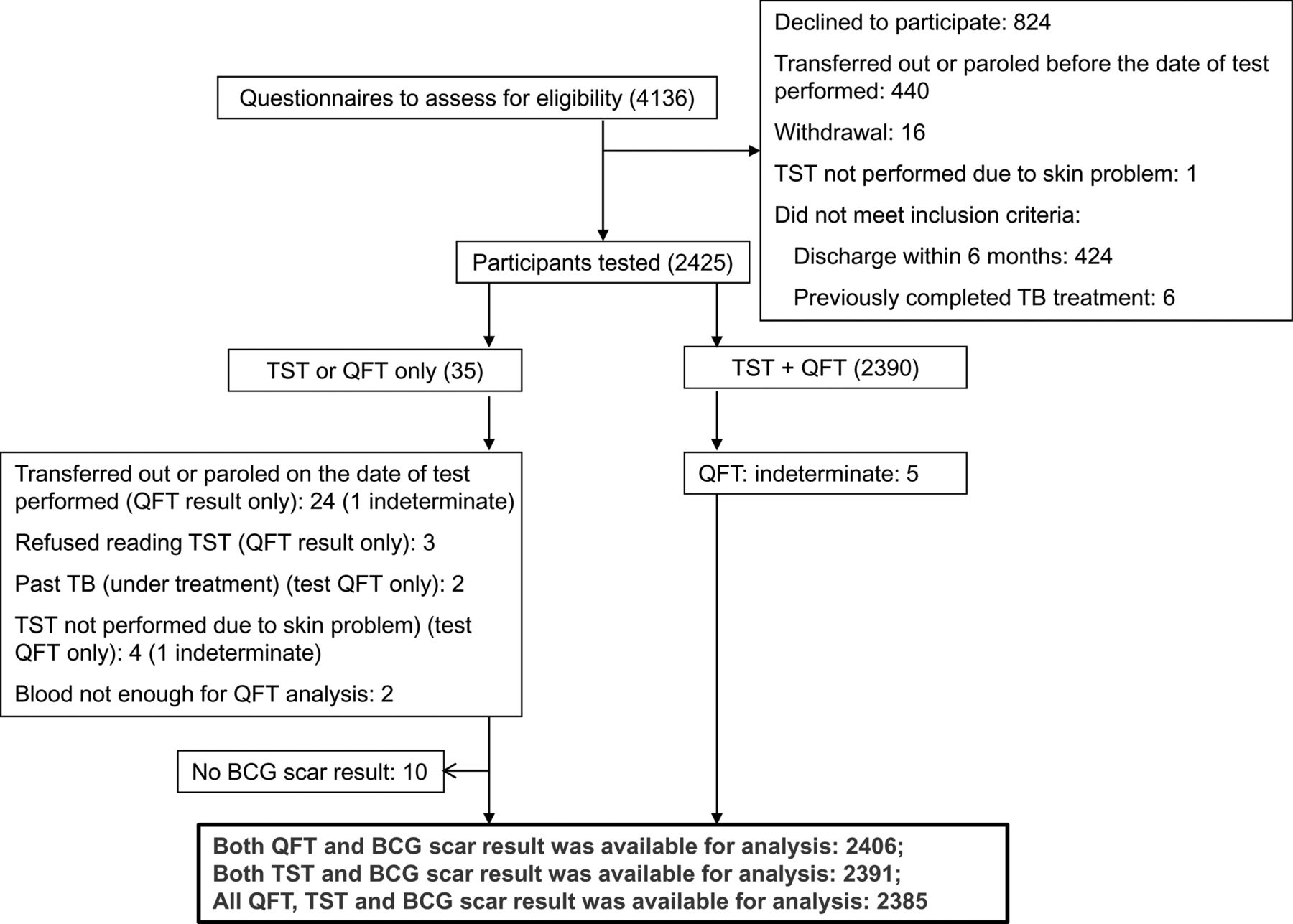
A total of 4136 inmates were invited to complete the questionnaires for enrolment. Of a total of 3312 (80%) inmates who agreed to be enrolled in our study, 2425 received at least one LTBI screening test, and 2385 had QFT-IT, TST and BCG data available for analysis (see figure 1 and table 1 for details).
Characteristics of participants who received at least one test in this study
{kind=link}
The flowchart of enrolment.
Overall, the QFT-IT was ≥0.35 IU/ml (LTBI) in 25% of the subjects and ≥0.7 IU/ml (recent LTBI) in 19% of the 2385 subjects included in the analysis. The TST was positive in 82% of the subjects with a cut-off point of 10 mm, 45% of the subjects with a cut-off of 15 mm, and 17% of the subjects with a cut-off of 18 mm. The concordance of these two tests was analysed according to different cut-offs for both the TST and QFT-IT (table 2). The κ values were 0.09 for a TST≥10 mm and a QFT-IT≥0.35 IU/ml, indicating a poor concordance between the two tests. The κ values were up to 0.243 for a TST≥18 mm and a QFT-IT≥0.7 IU/ml.
Summary statistics for the double positive results (QuantiFERON-TB Gold In-tube and TST) and the analysis for concordance between the two tests
Tables 3 and online Appendix table 2 show the positive rate of QFT-IT and TST, stratified by age groups and the number of BCG scars. Increasing positivity of QFT-IT was observed with increased age (p<0.001 by the Cochran–Armitage Trend Test). QFT-IT results were found to be inversely correlated with the number of BCG scars when two different cut-offs were used (LTBI or recent LTBI) in all three age groups (p<0.001 by Cochran–Mantel–Haenszel statistics) (table 3). By contrast, the TST positivity increased with the number of BCG scars when a cut-off of 10 mm was used (p<0.001), but the trend was not observed when cut-offs of 15 mm or 18 mm were used (appendix table S2).
Summary statistics for results of QuantiFERON-TB Gold In-tube
The evaluation for active TB disease identified only one case. The individual was asymptomatic at the time of arrival, but the chest radiograph showed a suspicious pulmonary lesion during the entry screening. However, 2 months later, the individual was determined as not having active TB because his cultures were negative and his chest radiography was stable. He therefore received an LTBI test, and the double-positive result was confirmed. He did not receive LTBI treatment. Two years later, bacteriology determined that the individual had active TB.
Discussion
Our results showed that after stratification by age, there was an inverse correlation between the number of BCG scars and the prevalence of positive QFT-IT, which indicates a protective effect of BCG against TB infection. Because the association was significant in all age groups (18–34 years, 35–54 years and ≥55 years), our results suggest that BCG vaccine seems to have a protective effect in adults decades after vaccination.
Our observation that BCG vaccination may provide protection against TB infection in adults is consistent with the previously reported findings in Turkey and the UK that there is a higher LTBI rate in unvaccinated children compared with those who were vaccinated.15 ,16 Diel et al also reported some evidence supporting a protective effect from BGC vaccination in 104 children aged <16 years in a cohort in Hamburg, Germany.24 The QFT-IT positive rate was higher in unvaccinated children (26.5%) than in those who were vaccinated (13.9%), although this difference did not reach statistical significance due to the small sample size.
Whether revaccination in adolescents or adults is beneficial or useless in TB control has long been a subject of debate. A double-blind, randomised, placebo-controlled trial conducted in Karonga, Malawi, between 1986 and 1987 showed that revaccination with BCG did not provide any protection against TB, but that primary vaccination or revaccination did provide protection against leprosy.27 WHO officially recommended to not revaccinate with BCG in 1995,18 and Taiwan followed the recommendation and stopped the revaccination programme in 1997.17 However, we should note that the Karonga trial in Malawi that documented the failed BCG revaccination strategy also failed to find primary BCG vaccination protective against TB.10 A retrospective cohort consisting of 303 692 children born between 1978 and 1982 in Hong Kong who received the primary BCG in infancy and a booster at 6–9 years of age also failed to demonstrate any significant difference in the TB rate between participants and non-participants in a school revaccination programme.28 An open-label, no-placebo, clustered, randomised, controlled trial was conducted among 200 805 schoolchildren aged 7–14 years in Salvador and Manaus, Brazil, 5 years later.29 In the initial follow-up for 3–4 years, no substantial additional protection from BCG revaccination in schoolchildren was found. However, after 9 years of follow-up, a 33% (3%–54%) vaccine efficacy in children aged <11 years was reported recently in Salvador, a location with a lower non-tuberculous mycobacteria (NTM) prevalence.30 This finding was comparable with the 30% (3%–52%) protective effect from BCG revaccination observed in non-reactors to NTM, 15 years after a double-blind, randomised, controlled trial conducted in South India.31 The inverse dose response of BCG vaccine over the TB infection risk noted in our study further supports the possibility that revaccination may have some protective effect.
The inconsistent protective effect from either BCG vaccination or revaccination has caused a number of debates over the past two decades.1 ,10 The difference in antigenicity between BCG strains and the epidemic strains prevalent in some regions could be factors behind the discrepancies between studies conducted in different geographical regions. Theoretically, the heavy use of BCG in high-burden regions could also drive the evolution of prevalent Mycobacterium tuberculosis strains. This hypothesis was proposed because of a case-control study of TB patients conducted in Vietnam, Hong Kong, China and The Netherlands, which revealed that a higher proportion of BCG-vaccinated TB cases were infected with the modern Beijing strain of M tuberculosis after age stratification.32 Further studies using cohort or randomised control trial designs to compare the protective efficacy of BCG against Beijing strains versus non-Beijing strains are required to clarify these important issues.
Consistent with previous reports from Korea, which has 95.7% BCG coverage and moderate LTBI risk,33 our results showed only an unsatisfactory concordance between TST and QFT. Similarly, discordance between TSTs and IGRAs was observed in Japanese health workers who had predominately undergone multiple BCG vaccinations.34 The concordance between the TST and QFT was also low in BCG-vaccinated Korean healthcare workers (κ=0.31, agreement 67.5%).35 The high false positive rates of the TST after BCG vaccination has raised concerns of unnecessary LTBI diagnosis and treatment,36 ,37 and can explain why the inverse correlation between BCG vaccination and LTBI could not be discovered by previous TST-based studies.
Similar to many previous studies,15 ,38 we used the number of BCG scars as a proxy for BCG vaccination record. The proportion of vaccinated people who develop and retain a recognisable scar following vaccination has been reported to vary from 98.9%, in a vaccine trial in South India 4 years after vaccination,38 to 60% in Swedish children assessed 14 years after vaccination at birth.39 In the present study, nurses did not know the result of LTBI when they counted the number of BCG scars. Therefore, any misclassification of a BCG scar would very likely be non-differential and yield a bias toward null. Our estimate for the correlation of more BCG scars with a lower rate of LTBI is, therefore, a conservative one.
In the present study, the lower prevalence of LTBI in BCG vaccinees is unlikely to be confounded by social economic status in early life because (1) BCG vaccination is free in Taiwan and (2) BCG vaccination is universally provided through public health stations (newborn and school children), hospitals (newborn), and schools (school children) in Taiwan. Thus, families from all social classes have the same access to BCG vaccination.
Our study has some limitations. Although up to 80% (3312/4136) of inmates were willing to be enrolled, 13% (440/3312) of them could not receive the test due to transfer or parole. As the age categories in stratification are broad (spanning 20 years), the relationship between BCG vaccination and LTBI could be confounded by a birth cohort effect if the TB trends changed rapidly over time. However, the nationwide TB registry data in Taiwan over the past half century (appendix table S1) show no such change, which makes confounding by birth cohort effect unlikely. Because of the limitations in the design of the cross-sectional study, the temporality between a lack of BCG vaccination and the occurrence of LTBI in participants is unclear. Furthermore, we were not informed of the reasons for the different numbers of vaccinations (or the lack of vaccination) among the participants. Therefore, factors influencing whether BCG has been received during infancy or childhood could confound our results. Nevertheless, analysis using QFT-IT≥0.7 IU/ml as a cut-off value, a marker of recently acquired LTBI, also yielded the same result, indicating that the observed effect is genuine rather than confounded or a coincidence. Therefore, our results justify further prospective cohort studies to clarify the causal relationship between BCG vaccine and protection against LTBI.
In conclusion, our results suggest that BCG vaccine seems to have a protective effect in adults decades after vaccination according to the number of recent infections (QFT-IT≥0.7 IU/ml). This finding has important implications for the continuation of a national policy of BCG vaccination. Further prospective cohort studies on the protective effect of BCG vaccination against TB infection in adults are warranted.
Acknowledgments
We thank all the participants who took part in the study, and the employees and physicians in Taipei Prison, Guishan Township, Taoyuan County. We acknowledge the crucial support of the Third Division, Taiwan CDC. We thank all the public health nurses who conducted the standard operational procedures for TST injection and reading in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online apendix
Footnotes
-
Contributors PCC, CHY, LYC, KFW, PRH, LMH: designed the study; PCC, CHY, LYC, KFW, YCK, CJL, SWL, PRH, LMH: conducted the study; PCC: performed the statistical analysis; PCC, CTF: wrote the first draft of the manuscript, with all authors contributing to the final draft; all authors contributed to the data interpretation and critically reviewed the manuscript; CTF, LMH: contributed equally to the study.
-
Funding This study was supported by the Centers for Disease Control, Taiwan (Grant DOH97-DC-1502), to which interim progress reports were submitted. The funding body had no role in study design, data analysis, data interpretation or writing of the report, except data collection.
-
Competing interests All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics approval The institutional review board of the National Taiwan University Hospital reviewed and approved the study protocol (No. 200707047M).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The dataset is available from the corresponding author at pcanita.tw@cdc.gov.tw.