Article Text

Abstract
Background Few data exist on tuberculosis (TB) incidence according to time from HIV seroconversion in high-income countries and whether rates following initiation of a combination of antiretroviral treatments (cARTs) differ from those soon after seroconversion.
Methods Data on individuals with well estimated dates of HIV seroconversion were used to analyse post-seroconversion TB rates, ending at the earliest of 1 January 1997, death or last clinic visit. TB rates were also estimated following cART initiation, ending at the earliest of death or last clinic visit. Poisson models were used to examine the effect of current and past level of immunosuppression on TB risk after cART initiation.
Results Of 19 815 individuals at risk during 1982–1996, TB incidence increased from 5.89/1000 person-years (PY) (95% CI 3.77 to 8.76) in the first year after seroconversion to 10.56 (4.83 to 20.04, p=0.01) at 10 years. Among 11 178 TB-free individuals initiating cART, the TB rate in the first year after cART initiation was 4.23/1000 PY (3.07 to 5.71) and dropped thereafter, remaining constant from year 2 onwards averaging at 1.64/1000 PY (1.29 to 2.05). Current CD4 count was inversely associated with TB rates, while nadir CD4 count was not associated with TB rates after adjustment for current CD4 count, HIV-RNA at cART initiation.
Conclusions TB risk increases with duration of HIV infection in the absence of cART. Following cART initiation, TB incidence rates were lower than levels immediately following seroconversion. Implementation of current recommendations to prevent TB in early HIV infection could be beneficial.
- Tuberculosis
Statistics from Altmetric.com
Key messages
What is the key question?
-
Few data exist on tuberculosis (TB) incidence according to time from HIV seroconversion in high-income countries and whether rates following combined antiretroviral therapy (cART) initiation differ from those soon after seroconversion. This information is important to inform the optimal timing of implementation of TB-preventive strategies.
What is the bottom line?
-
In this study using CASCADE data on HIV-positive individuals with well estimated date of HIV seroconversion, we found that the risk of TB in the absence of cART increases with HIV infection duration and is lower after cART initiation than the risk immediately following HIV seroconversion.
Why read on?
-
This study suggests that a more stringent application of currently recommended TB-preventive measures early in HIV infection could help to reduce the TB burden in high-income countries.
Introduction
Active tuberculosis (TB) among HIV-positive individuals in high-income countries is of concern. Although TB morbidity has fallen since combined antiretroviral therapy (cART) became widely available,1 ,2 this reduction has not been as remarkable as that observed for other opportunistic infections3 and TB may be diagnosed at relatively high current and nadir CD4 cell counts.4 In addition, the risk of TB in high-income countries is substantial even after starting cART due to the increasing proportion of migrants from high-burden TB areas, such as sub-Saharan Africa.5–8 An additional concern about TB is immune reconstitution inflammatory syndrome (IRIS), an incompletely understood and poorly quantified immunological phenomenon consisting of a paradoxical worsening of previously treated TB or the unmasking of subclinical TB in the first few months following cART initiation.9
Effective means to reduce and prevent TB disease among HIV-positive individuals include screening for latent TB, treatment for latent infection (TLI), and initiation of cART at CD4 count thresholds as indicated by national and international guidelines.10–12 However, a clear understanding of the clinical epidemiology of TB risk at all stages of HIV infection, particularly in early infection, and how this differs from risk following cART initiation is lacking but is needed to inform healthcare personnel on the optimal timing of the implementation of TB-preventive strategies.
Using data from HIV-positive individuals with well estimated dates of HIV seroconversion, we aimed to estimate TB incidence rates following HIV seroconversion and before cART initiation and to evaluate whether the risk of TB following cART differs from the risk in early HIV infection when the immune system is still relatively intact. Finally, we wanted to explore the role of current and past levels of immunosuppression on TB risk after cART initiation.
Methods
Patients
We used data from CASCADE, a collaboration of 28 cohorts of individuals with well estimated dates of HIV seroconversion from Europe, Australia, Canada and sub-Saharan Africa.13 The date of seroconversion was estimated by various methods, most frequently as the midpoint of an interval of <3 years between a negative and a positive HIV antibody test result; laboratory evidence of seroconversion; the date of a seroconversion illness; or the most likely date of infected factor VIII concentrate infusion for haemophiliacs. As the study aims to quantify TB risk in high-income countries, data from the sub-Saharan African cohorts were excluded. Finally, individuals younger than 16 years at seroconversion were excluded. Data were pooled in 2009 within EuroCoord (http://www.EuroCoord.net).
TB diagnosis
Only the first TB diagnosis after entry into the cohort was included. This was not necessarily the first-ever TB episode per patient. TB was classified as pulmonary or extrapulmonary. Most TB diagnoses were definitive, defined as having a positive culture for Mycobacterium tuberculosis isolated from any clinical sample (sputum, bronchial washings, pleural fluid, lymph node, bone marrow aspirate, cerebrospinal fluid), and fewer were presumptive, defined as having clinical or radiological signs suggestive of TB, other causes were excluded, and showing a clinical response to TB treatment. Skin tests for M tuberculosis infection and TLI were not systematically done in most of the cohorts.
Statistical analyses
Risk of TB after HIV seroconversion in the pre-cART era
We computed TB incidence rates in the pre-cART era as the number of first-ever recorded TB events per 1000 person-years (PY). Follow-up started at seroconversion or enrolment into a cohort, whichever was later, and ended at the last visit to the clinic, death, 1 January 1997 or TB diagnosis, whichever was earliest. TB rates were computed by duration of HIV infection in 1-year intervals and time-dependent current CD4 count category (<200, 200–349, 350–499, ≥500 cells/mm3). Using all available CD4 counts, we assumed a constant CD4 count from the date of measurement until the date of the next measurement. When a CD4 count was not followed by a subsequent measurement within 6 months, the patient was excluded from the risk set until a new CD4 count became available.
We conducted the following sensitivity analyses. As pulmonary TB became an AIDS-defining event in 1993, we recomputed TB rates restricted to follow-up after 1 January 1993.14 As cART was available before 1997 in some cohorts, follow-up ended at 1 January 1996. Because of the uncertainty regarding the date of seroconversion, we recomputed TB rates including only patients with an HIV test interval <12 months. Finally, we excluded TB events and time at risk within 30 days of cohort enrolment.
Risk of TB after cART initiation
We computed TB incidence rates after cART initiation in individuals without TB with follow-up ending at death, last visit to the clinic or TB diagnosis, whichever was earliest. We presented TB rates by time-dependent duration of cART in years and current CD4 count category (<200, 200–349, 350–499, ≥500 cells/mm3). To assess the impact of late cART initiation, we also computed these rates separately by CD4 count category at cART initiation (<50, 50–199, 200–349, 350–499, ≥500 cells/mm3).
Univariate Poisson models were used to examine the association between TB rates after cART initiation and current and past level of immunosuppression measured as time-dependent current CD4 cell count, HIV-RNA, nadir, time-weighted average CD4 count and duration of HIV infection at cART initiation. These variables were included in a multivariable model, adjusting for the following potential confounders chosen a priori: risk group, sex, current age, calendar year of cART initiation (<2001 or ≥2001), and geographical region of origin. The latter was categorised as follows: very high incidence region: sub-Saharan Africa; high–mid risk regions: Eastern Europe, Central Asia, North Africa, South Asia, East Asia and the Caribbean; mid–low risk regions: Western Europe, Middle East, the Americas and Oceania; and unknown. The results were presented from a reduced model, including all covariates measuring current and past level of immunosuppression and potential confounding variables significant at the 10% level in the univariate analysis. To explore if current CD4 count was an independent predictor of TB risk after accounting for virological status, we refit the final model adjusting for current log10 HIV-RNA.
Average CD4 cell count was estimated as the area under the CD4 count curve before cART initiation against time. Then, the time-weighted average was obtained by dividing the area under the curve by duration of follow-up since seroconversion.15
TB diagnoses occurring on the same date as cART initiation were excluded. To avoid selective drop-out of patients failing to respond to cART, we assumed that, once started, patients remained on treatment.
cART was defined as a combination of at least three drugs from at least two classes or at least three nucleoside reverse-transcriptase inhibitors, one of which was tenofovir or abacavir.
As TB risk during treatment interruption could be higher due to virological rebound, we recomputed TB rates while patients were known to be off cART after interruption defined as at least 15 days without any treatment.
Data were analysed using STATA V.11.0.
Results
Patients’ characteristics
Of 19 815 patients in CASCADE, we included 9175 and 11 178 patients at risk of TB in the pre-cART era and after cART initiation, respectively. A total of 4575 patients contributed follow-up data to both analyses. Most patients were men who acquired HIV through sex with men and originated from low-burden TB countries (table 1). In the pre-cART era the proportion of patients originating from high-burden TB areas varied from 4% in France and Norway to <1% in Greece and Italy.
Characteristics of patients at risk of tuberculosis in the pre-cART era (before1 January 1997) and after cART initiation
Risk of TB following HIV seroconversion in the pre-cART era
Of 9175 patients at risk during 1982–1996 with median age of 36 years (IQR 31–42), 243 were diagnosed with TB during 35 906 PY. These men presented with a median CD4 cell count of 125 cells/mm3 (IQR 40–286) and duration of infection of 3.4 years (IQR 1.1–7.3) at TB diagnosis.
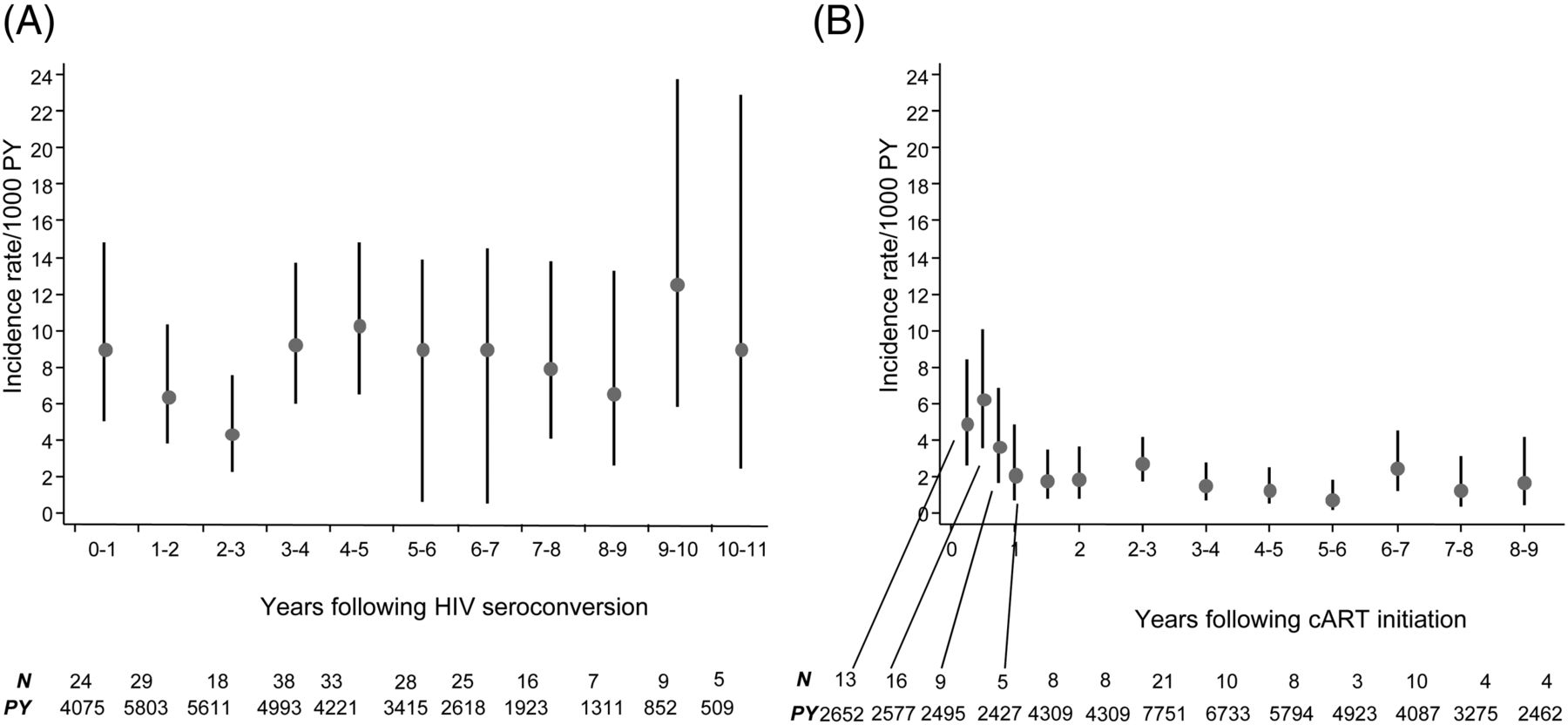
Figure 1A presents TB incidence rates according to duration of HIV infection. Although the risk decreased in the first 3 years following seroconversion, overall TB rates increased from 5.9/1000 PY (95% CI 3.77 to 8.76) in the first year following HIV seroconversion to 10.6/1000 PY (4.83 to 20.04) at 10 years (test for trend p<0.001). TB rates were 21.9 events/1000 PY (17.9 to 26.6), 6.4 (4.5 to 8.9), 3.2 (1.9 to 5.0), 3.3 (2.3 to 4.8) and 5.4 (4.0 to 7.1) for current CD4 count categories of <200, 200–349, 350–500, ≥500 cells/mm3 and missing CD4 count, respectively. The proportion of follow-up with unknown CD4 count was 26%. Median (IQR) duration of HIV infection in years was 5.7 (4.0–7.6), 5.0 (3.2–7.2), 4.0 (2.3–6.1), 3.2 (1.8–5.2), 2.4 (1.0–4.1) and 3.0 (1.7–5.1) for current CD4 categories of <50, 50–199, 200–349, 350–500, ≥500 cells/mm3 and missing CD4 count, respectively.
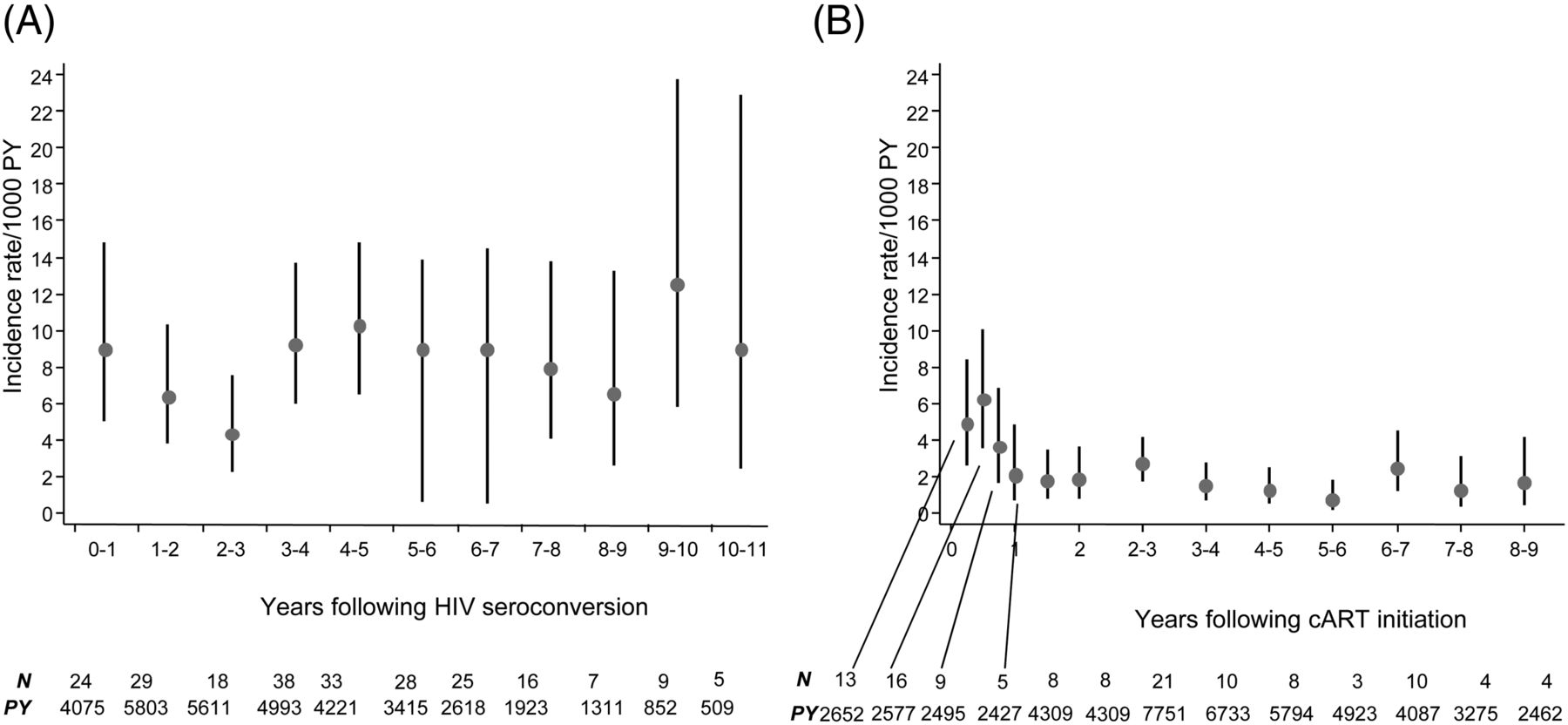
Trends in incidence rates (with 95% CIs) of tuberculosis according to (A) duration of HIV seroconversion in the pre-combination antiretroviral therapy (cART) era and (B) time since initiation of cART. CIs (as shown by error bars) were computed assuming a Poisson distribution for the number of events. PY, patient-years.
Similar TB rates were found when the 33 TB cases diagnosed on the date of enrolment were excluded, when individual follow-up was ended at 1 January 1996 and when the analyses were restricted to patients with an HIV test interval <12 months. The TB rate in the first year following seroconversion was 8.9 (95% CI 5.0 to 14.8) per 1000 PY when pre-1993 follow-up was excluded, somewhat higher than that estimated in the main analysis.
Incidence of TB after cART initiation
There were 11 178 patients without TB who started cART at a median CD4 count of 320 cells/mm3 (IQR 210–470), mostly (61%) with a combination including a protease inhibitor. Of these, 120 were diagnosed with TB during 57 104 PY at a median CD4 count of 195 cells/mm3 (IQR 55–419) and log10 HIV-RNA of 4.2 log10 copies/ml (IQR 1.8–5.3) (table 1). The overall TB incidence rate after cART initiation was 2.1/1000 PY (95% CI 1.7 to 2.5).
Trends of TB rates according to time since cART initiation are presented in figure 1B. Although TB rates increased in the first 2 months following cART initiation, they dropped from 4.2/1000 PY (95% CI 3.1 to 5.7) in the first year after cART initiation and remained constant thereafter (average rate from year 2 onwards 1.64/1000 PY; 95% CI 1.29 to 2.05). The trend of initial increase in TB incidence was particularly remarkable in patients who initiated cART at CD4 <50 cells/mm3 (figure 2). The proportion of total follow-up spent with CD4 count ≥500 was 49.4% and TB rate at these CD4 levels was 0.9/1000 PY (95% CI 0.5 to 1.4). Median (IQR) nadir and time-weighted average CD4 cell count and duration of HIV infection at cART initiation were 260 cells/mm3 (169–367), 419 cells/mm3 (309–546) and 3.42 years (1.05–7.30), respectively.

{kind=link}
{kind=link}
Trends in incidence rates of tuberculosis according to time since initiation of combination antiretroviral therapy (cART) and CD4 count at cART initiation.
TB incidence during treatment interruption was 2.2 events/1000 PY (95% CI 1.2 to 3.8). When we excluded TB events occurring within the first 30 days after cART initiation, the TB rate in the first year was 4.22/1000 PY (95% CI 3.00 to 5.76).
Effect of current and past level of immunosuppression on the incidence of TB following cART initiation
While lower CD4 nadir and time-weighted average CD4 count at cART initiation were associated with increased TB risk in the univariate analyses (p values 0.011 and 0.031, respectively), there was no evidence they were independent predictors after adjusting for current CD4 count. In the final multivariable model, higher current CD4 count category and lower HIV-RNA at cART initiation were significantly associated with lower TB incidence (table 2). Being an injecting drug user was associated with increased risk of TB following cART initiation. In the model including current HIV-RNA, current CD4 count and current HIV-RNA were independent predictors of TB risk after cART initiation (p values 0.01 and 0.001, respectively) (results not shown).
Factors associated with TB incidence after cART initiation
Discussion
In this study of individuals followed up since HIV seroconversion in high-income countries we found that the risk of TB increases with HIV infection duration in the pre-cART era, is lower after cART initiation than the risk immediately following seroconversion, and is strongly associated with current CD4 count, not past levels, once cART is initiated.
The finding that the risk of TB increases with duration of HIV infection is in agreement with previous reports from smaller cohorts from the Netherlands,16 Spain17 and South Africa18 and suggests that HIV-positive patients would benefit from TB prevention being implemented at an early stage. The trend of relatively high TB risk in the first year and of decreasing risk in the 2–3 years following seroconversion could be explained by an increased risk of reactivation of latent TB during primary HIV infection. Alternatively, this could be an artefact due to the uncertainty around the date of HIV seroconversion. This is unlikely, however, as analyses in patients with an HIV test interval <12 months showed similar patterns of TB risk in early infection. Animal models19 and in vitro studies20 suggest that, during early HIV infection, M tuberculosis-specific CD4 T cells may be selectively depleted, resulting in a rapid increase in the risk of developing active TB immediately following seroconversion. Moreover, this defect in functional anti-mycobacterial immunity can only be partially restored by ART.21 Unfortunately, we were unable to explore the impact of seroconversion on TB risk since we have no information on the risk before seroconversion. Therefore, any TB events occurring between HIV acquisition and HIV diagnosis may have been missed, although this is unlikely to be a major source of bias.
We found that the TB incidence rate after cART initiation (2 events/1000 PY) was lower than the rate observed during the first year after seroconversion, when the immune system was still relatively intact (ranging from 6 to 9/1000 PY). This result could indicate that the beneficial effect of cART on restoration of TB-specific defence cannot be solely estimated by measuring absolute CD4 counts in peripheral blood and that viral suppression restores other immune functions. This has been observed for other opportunistic diseases, such as Pneumocystis jirovecii pneumonia.22
We found that the risk of TB after cART initiation remained substantial, as the TB rate after cART initiation with current CD4 >500 cells/mm3 was 0.9 events/1000 PY (95% CI 0.5 to 1.4). This is higher than rates estimated by WHO for the general population, which ranged from 0.05 to 0.2/1000 PY in the same high-income countries (WHO 2010).23 This high rate could be explained by factors such as incomplete immune recovery which may favour reactivation of persisting latent infection, increased risk of exposure to TB in healthcare facilities, and/or the presence of a large proportion of HIV-positive patients from high TB-burden countries or injecting drug users.
To our knowledge, this is the largest study examining the association between current or previous immunosuppression and the risk of TB after cART initiation. While nadir CD4 count is a marker if the risk of TB is increased by previous immune system damage, even after subsequent immunological recovery, time-weighted average CD4 count is a summary measure of the overall immunodeficiency history. Current CD4 count and HIV RNA at cART initiation were the dominant predictors of TB risk and we found no association between markers of past history of immunosuppression, such as duration of infection, nadir and time-weighted average CD4 count at cART initiation. We also found that higher current HIV-RNA in the same CD4 count strata was associated with increased TB risk. Therefore, in addition to an increase in CD4 counts, suppression of viral replication seems to be important for immunological control of latent TB infection in patients on cART.
Consistent with previous reports,24–26 we observed an increase in TB risk immediately following cART initiation, especially in patients who were started on cART at CD4 <50 cells/mm3. As screening for TB before ART was not standard practice in the CASCADE cohorts, the high initial TB rates could be partly explained by more intensive clinical evaluation in patients starting cART, increasing the chance of diagnosis of prevalent undiagnosed TB.27 Alternately, some of these events may be due to unmasking of subclinical active infections by IRIS, a common phenomenon after cART initiation in patients with TB infection and low CD4 counts. As CASCADE does not collect clinical data on TB diagnoses, we could not identify the relevant IRIS cases. Nevertheless, the increase in risk following cART suggests that screening for latent and active TB before cART and TLI in patients with positive skin test, as recommended by national and international guidelines, could be beneficial.26
Our study has several limitations. First, we had no information on TLI. As TLI has been shown to effectively reduce the risk of active TB in patients coinfected with HIV,11 ,28 we could have underestimated the risk. However, this is unlikely to have occurred as, with the exception of the Swiss HIV cohort, TLI is rarely provided to patients with HIV in the countries contributing data to the analysis.
Second, we did not have information on treatment adherence and assumed that patients remained on therapy once it was initiated. If diagnoses of TB are largely occurring in individuals who have stopped cART or have poor adherence, then the TB incidence after cART initiation would have been overestimated. Nevertheless, our estimates are likely to be robust because we found similar estimates of TB rates after cART initiation when we only included individual follow-up time while patients were known to be on cART.
Third, a relatively large proportion of follow-up in the pre-cART era was spent with unknown CD4 cell count. Median duration of HIV infection when CD4 count was unknown was 3 years, suggesting that we might have underestimated the risk of TB at high CD4 count in the pre-cART era.
Fourth, to avoid informative censoring due to ART initiation, we estimated the TB risk in cART-naïve patients restricting analyses to the pre-cART era. TB exposure could have increased in the last decade because of increasing numbers of migrants from high-burden TB areas. However, the decreasing TB risk among patients taking cART may have reduced the risk of acquiring TB from patients visiting the same clinic.
Finally, when we compared TB risk between patients in the pre-cART era with the risk after cART initiation our estimates may have been biased through confounding by indication (ie, patients who start cART are more likely to be sicker and at higher TB risk). This would have led to an overestimate of the risk of TB among those who initiated cART and would thus tend towards estimating similar rates in the pre-cART era and after cART initiation. Of note, we observed a lower TB risk after cART, despite this potential bias.
In conclusion, in this study of patients with a well estimated date of HIV seroconversion, we found that TB risk increases from early HIV infection. More stringent diagnosis and treatment of latent TB early in HIV infection could therefore help to reduce the TB burden in high-income countries. This would also benefit patients not yet eligible for cART according to current treatment guidelines. Finally, as the TB risk after cART initiation is lower than the risk in cART-naïve individuals, access to cART and implementation of effective TB treatment is essential in reducing the TB risk in high-income countries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors Concept and design (EG, SL, JdA), statistical analyses (SL), interpretation of the data (SL, EG), drafting the manuscript (SL), critical revision of the manuscript for important intellectual content (all authors) and securing funding (KP).
-
Funding This work was supported by the European Union Seventh Framework Programme (FP7/2007-2013) under EuroCoord grant agreement 260694. Sara Lodi is holder of a Juan de la Cierva Fellowship (grant number JCI 2010-08151). Enrico Girardi was supported by the Italian Ministry of Health—Progetto AIDS, grant number 40H79. E.
-
Competing interests EG has received honoraria for presentation at workshops or travel grants from Abbott, Bristol-Myers Squibb, Boheringer Ingelheim and a non-restricted research grant from Gilead sciences; and grant support from the Italian Ministry of Health—Progetto AIDS. KP has received an honorarium from Tibotec. ADM has received honoraria for being on advisory boards from Abbott, Bristol-Myers Squibb and Jannsen, and has received unrestricted research grants from Abbott, Jannsen and Merck-Sharp and Dohme. CS has received fees for consulting, membership of data safety and monitoring boards/advisory panels, the development of educational materials, speaking engagements, and support to travel to meetings from the following companies: Gilead Sciences, Abbott Pharmaceuticals, Janssen-Cilag, Bristol-Myers Squibb, Merck Sharp and Dohme and Glaxo-Smith Kline. The institution of HF has received payments for participation in advisory boards and/or unrestricted educational grants and/or travel grants from Abbott, BMS, ViiV Healthcare, Roche, Gilead, MSD, Boehringer-Ingelheim, Tibotec-Janssen and unrestricted research support from Gilead, MSD and Roche. SA has received travel grants or honoraria from pharmaceutical companies including ViiV Healthcare, Abbott, Janssen-Cilag, Bristol-Myers-Squibb, Gilead and Boehringer Ingelheim.
-
Ethics approval All cohorts received approval from their individual ethics review boards. Two ethics review boards, the Danish cohort and the Greek Haemophiliacs cohort, deemed their cohort participants exempt from providing signed informed consent because there was no intervention, no additional clinic visits required or blood taken, and only anonymous and non-identifiable data were available for research. Signed informed consent was obtained from patients in the other cohorts. Approval was also given by all ethics review boards to pool anonymised data for analyses and dissemination.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Some of the results in this manuscript were presented at the Conference on HIV Pathogenesis, Treatment and Prevention, Rome (Italy), 17–21 July 2011. The abstract is available online at http://pag.ias2011.org/Abstracts.aspx?AID=1952