Article Text

Abstract
Background This study evaluated the efficacy of a mindfulness training programme (mindfulness-based stress reduction (MBSR)) in improving asthma-related quality of life and lung function in patients with asthma.
Methods A randomised controlled trial compared an 8-week MBSR group-based programme (n=42) with an educational control programme (n=41) in adults with mild, moderate or severe persistent asthma recruited at a university hospital outpatient primary care and pulmonary care clinic. Primary outcomes were quality of life (Asthma Quality of Life Questionnaire) and lung function (change from baseline in 2-week average morning peak expiratory flow (PEF)). Secondary outcomes were asthma control assessed by 2007 National Institutes of Health/National Heart Lung and Blood Institute guidelines, and stress (Perceived Stress Scale (PSS)). Follow-up assessments were conducted at 10 weeks, 6 and 12 months.
Results At 12 months MBSR resulted in clinically significant improvements from baseline in quality of life (differential change in Asthma Quality of Life Questionnaire score for MBSR vs control: 0.66 (95% CI 0.30 to 1.03; p<0.001)) but not in lung function (morning PEF, PEF variability and forced expiratory volume in 1 s). MBSR also resulted in clinically significant improvements in perceived stress (differential change in PSS score for MBSR vs control: −4.5 (95% CI −7.1 to −1.9; p=0.001)). There was no significant difference (p=0.301) in percentage of patients in MBSR with well controlled asthma (7.3% at baseline to 19.4%) compared with the control condition (7.5% at baseline to 7.9%).
Conclusions MBSR produced lasting and clinically significant improvements in asthma-related quality of life and stress in patients with persistent asthma, without improvements in lung function.
Clinical Trial Registration Number Asthma and Mindfulness-Based Reduction (MBSR) Identifier: NCT00682669. clinicaltrials.gov.
- Asthma
- mindfulness training
- quality of life
- lung function
- stress
- asthma guidelines
- respiratory measurement
Statistics from Altmetric.com
- Asthma
- mindfulness training
- quality of life
- lung function
- stress
- asthma guidelines
- respiratory measurement
Key messages
What is the key question?
Can a mind–body training programme bring about a lasting improvement in quality of life and lung function in patients with asthma?
What is the bottom line?
Compared with an educational control, a mind–body training programme was found to result in lasting improvements in patients' quality of life.
Why read on?
This is the first report of a controlled trial of a mind–body training programme that used an active control programme, followed patients for 12 months, and included clinically accepted disease outcome markers. It has significant implications for the clinical management of asthma.
Introduction
Asthma places considerable demands on patients, and interventions to facilitate adjustment to the disease may be important in asthma management even when lung function does not improve.1 Psychosocial factors are also implicated. The elevated perceived stress prevalent in patients with asthma negatively affects their quality of life (QOL) and is strongly associated with reduced medication adherence and worse asthma control,2 and with over-perceiving dyspnoea and respiratory symptoms unaccompanied by objective measures.3 To limit exacerbations related to these factors, patients need to be able to discriminate between their asthma symptoms and the associated affect-related sensations and cognitions4; nevertheless, self-management programmes typically focus on education about external triggers and medication usage. While cognitive behavioural therapy appears to have a positive effect on asthma QOL and relaxation therapy reduced ‘as needed’ medication use, the heterogeneity and low quality of studies of the complementary approaches used by 40% of patients with asthma preclude firm conclusions on their role in asthma.5 ,6
Mindfulness training involves learning to recognise and discriminate between components of experience, including thoughts, feelings, and sensations, and developing a non-reactive awareness of these. Mindfulness-based stress reduction (MBSR) is a widely available group-based mindfulness training programme that reduces perceived stress, disease-related distress and reported medical symptoms in a range of chronic diseases,7 but has not been studied for its effect on asthma QOL and management. We hypothesised that MBSR would result in greater QOL and lung function improvements compared with an education control condition.
Methods
Study sample
Participants were adult patients recruited between October 2006 and December 2007 from primary and pulmonary care clinics at UMass Memorial Health Care (UMMHC) in Worcester, Massachusetts, USA.
Inclusion criteria were physician-documented asthma with an objective indicator of bronchial hyper-responsiveness (positive methacholine challenge test, ≥12% improvement in forced expiratory volume in 1 s (FEV1) or forced vital capacity (FVC) in response to bronchodilator, or 20% variability in diurnal peak expiratory flow (PEF) variation), or ≥12% improvement in FEV1 in response to inhaled bronchodilator on spirometry at study entry; and met 2007 National Institutes of Health/National Heart Lung and Blood Institute (NIH/NHLBI)8 criteria for mild, moderate, or severe persistent asthma.
Patients were excluded if they had intermittent asthma (symptoms less than once/week, brief exacerbations, nocturnal symptoms ≤ twice/month, and normal lung function between episodes); smoked in the past year; other lung diseases; current treatment for symptomatic cardiovascular disease; history of a positive tuberculosis test; participated in MBSR and/or practicing meditation regularly.
Figure 1 shows the flow of participants. Eighty-three proceeded to randomisation. Follow-up occurred between April 2007 and February 2008. The University of Massachusetts Medical School Institutional Review Board approved the protocol. Participants gave informed consent and continued to be managed by their physician.

Consort diagram. HLC, healthy living course; MBSR, mindfulness-based stress reduction.
Intervention groups
The intervention was MBSR; the control was a Healthy Living Course. Group assignment was by a random allocation scheme with block sizes of four and six.
MBSR consisted of 8 weekly 2.5 h sessions, and an all-day (6 h) session in week 6.9 To enhance generalisability, participants were integrated into regularly scheduled UMMHC MBSR classes and had approximately two study and 28 non-study participants. Mindfulness training was through the following techniques: body scan, when attention is systematically moved through the body to bring awareness to sensations; sitting meditation focusing on awareness of breathing, thoughts and feelings; and gentle stretching exercises to develop awareness during movement. The classes emphasised integration of mindfulness into everyday life to support coping with symptoms and stress. Two CDs containing guided mindfulness exercises were provided to be practiced for 30 min, 6 days/week.
To control for as many non-specific factors as possible, we developed a healthy living course (HLC) matched for time, instructor attention and format. Classes consisted of lectures and discussion of self-care topics: healthy nutrition; physical activity; coping with stress (not including mindfulness); sleep hygiene; balancing work and personal life; and living a drug-free life. Homework was assigned consistent in time with MBSR. To match the MBSR mix of participants, HLC was offered to community members in addition to study participants and consisted of approximately 7 study and 18 non-study participants. Classes were held during the same timeframe as MBSR to control for seasonal variation.
Outcome measures
Assessments occurred at baseline, and at 10 weeks and 6 and 12 months post baseline by evaluators blind to treatment assignment.
Primary outcomes were QOL and lung function. The Asthma Quality of Life Questionnaire (AQOL)10 ,11 (32-items) assesses the degree to which important activities were limited by asthma during the last 2 weeks in four domains: activity limitations, asthma symptoms, emotional function and environmental exposure. The overall QOL score, an average of the domains, is valid, reliable and sensitive to changes in asthma symptoms.10 The minimum important change in overall QOL score and each of the domains is 0.5.11
Lung function was assessed by change from baseline in 2-week average morning PEF (litres/min), consistent with studies by the National Heart, Lung, and Blood Institute's Asthma Clinical Research Network (ClinicalTrials.gov). While correlation with FEV1 is not always ideal, PEF is easily performed at home and often used as an indicator of lung function. Additional lung function measures were spirometry and PEF variability. Spirometry was performed in the UMMHC Pulmonary Diagnostic Laboratory according to American Thoracic Society guidelines12 and assessed FEV1 and FVC. PEF variability compared the minimum morning pre-bronchodilator PEF with the recent best (day's highest minus lowest/mean), providing an amplitude per cent mean.13
Secondary outcomes were perceived stress, and asthma control classification based on 2007 NIH/NHLBI criteria.8 Those in a less well controlled category for any component were classified at the higher category. The 10-item Perceived Stress Scale (PSS)14 assessed the degree to which the person appraised their coping resources as insufficient to meet the demands of events in the past month.
At each assessment, participants recorded frequency of asthma rescue medication use (short-acting bronchodilators) over a 14-day period, and days of work or school missed due to asthma. Asthma exacerbations were assessed by self-reported initiation of prednisone in the last 30 days.
Analysis
Analyses were carried out using Stata V.10.1 (Stata Corporation). This was a pilot study powered at the 10% significance level for a mean difference in AQOL between groups of <0.5,11 and a difference in mean per cent change in PEF of 10%.15 At the 10% significance level, there was 80% power with n=35/group. At the 5% significance level the effective power was 70%. With a predicted 15% dropout, the recruitment goal was 42/group. A significance threshold of p<0.05 was used for all analyses. Baseline distributions of important patient characteristics were compared by study group based on non-missing data. T-tests compared AQOL, FEV1, per cent predicted FEV1 and perceived stress, and Wilcoxon rank sum tests compared variables with skewed distributions (short short-term inhaler use, days absent due to asthma). Fisher's exact tests compared all categorical variables.
Prednisone use differed between groups at baseline and was included in final models if associated with time trends and altered estimates of study arm effects.
For the peak flow/medication form and spirometry, there were up to 21 missing data points at follow-up. For short-term rescue medication use, 2-week average morning PEF, PEF variability, and FEV1, missing values were extrapolated using the slope of the two closest non-missing values; for 10 patients, single non-missing values were carried forward to all subsequent time points. The results presented are from these imputed models. Difference in improvement in AQOL (by 1 or 1.5 points) at 12 months was tested using Fisher's exact test. Class attendance was compared using the Wilcoxon rank-sum test.
The basic analytic strategy was to compare differential trends over time for the intervention versus comparison group. The main outcomes were derived from a difference-of-difference analysis representing over-time change in the intervention group after accounting for simultaneous change in the comparison group. Trends over time in AQOL, PSS, PEF variability, morning PEF and FEV1 were analysed using linear mixed models with random intercepts and slopes, with participant as the random effect. Each outcome was modelled as a function of group, categorical time and the group–time interaction. The group–time coefficients reflected differential over-time change for the intervention versus comparison group. Time coefficients reflected over-time change in the comparison group, while the sum of time and group–time coefficients provided change in the intervention group. Dichotomous outcomes (well controlled asthma, prednisone use in past 30 days and long-term controller use) were analysed using Generalised Estimating Equation logistic regression. Times/week using short-term rescue medication was modelled with Generalised Estimating Equation negative binomial regression. For all models, clustering was on participant and an exchangeable correlation structure was assumed. Each outcome was modelled as a function of group, categorical time, and the group–time interaction. The model for rescue medication also included baseline prednisone use and the interaction of baseline prednisone use and time as covariates. Estimates of ORs, incidence rate ratios and CIs were derived from the models.
Results
Baseline characteristics
The 56 women and 27 men had a mean age of 52.8 years (see table 1). The majority were white (93.8%), non-Latino (92.3%) and had either some college or a college or advanced degree (68.8%). Per cent with well controlled asthma was very low (7.4%), consistent with the exclusion of intermittent or well controlled asthma. Of those whose asthma was not well controlled, 80.0% in HLC and 83.8% in MBSR were on inhaled corticosteroid or oral prednisone. The number of years taking asthma medication was 13.3. Mean baseline AQOL (5.20 overall; 5.46 men, 5.08 women) was similar to a cross-sectional study of US adults with asthma.16 Mean perceived stress (16.6) was 0.5 SD above the US norm.17 The only significant difference between arms in demographical and clinical characteristics was prednisone/Methylprednisolone use in the past 30 days (MBSR 24.4% vs HLC 4.9%, p=0.026). The two conditions did not differ on any other asthma control measures.
Baseline socio-demographical and clinical characteristics
Primary outcomes
Asthma-related QOL
At 12-month follow-up, overall AQOL had significantly improved in the MBSR group compared with controls, increasing by 0.72 and 0.06 respectively (differential change of 0.66, p<0.001) (see table 2 and figure 2). The MBSR group also improved in three of the four AQOL components: activity limitations (differential change of 0.66, p=0.0.003), symptoms (differential change of 0.63, p=0.002) and emotional function (differential change of 0.81, p=0.002) (see table 2). At 12 months the effect of MBSR versus control on overall AQOL (differential change of 0.66) was >0.50, which is considered a clinically significant improvement, and more patients in the MBSR group achieved moderate (≥1 point) (34% vs 12%, p=0.031) and large improvements in AQOL (≥1.5 points) (18% vs 5%, p=0.080).11
Asthma Quality of Life (AQOL): model-derived estimates for baseline, follow-up and change from baseline
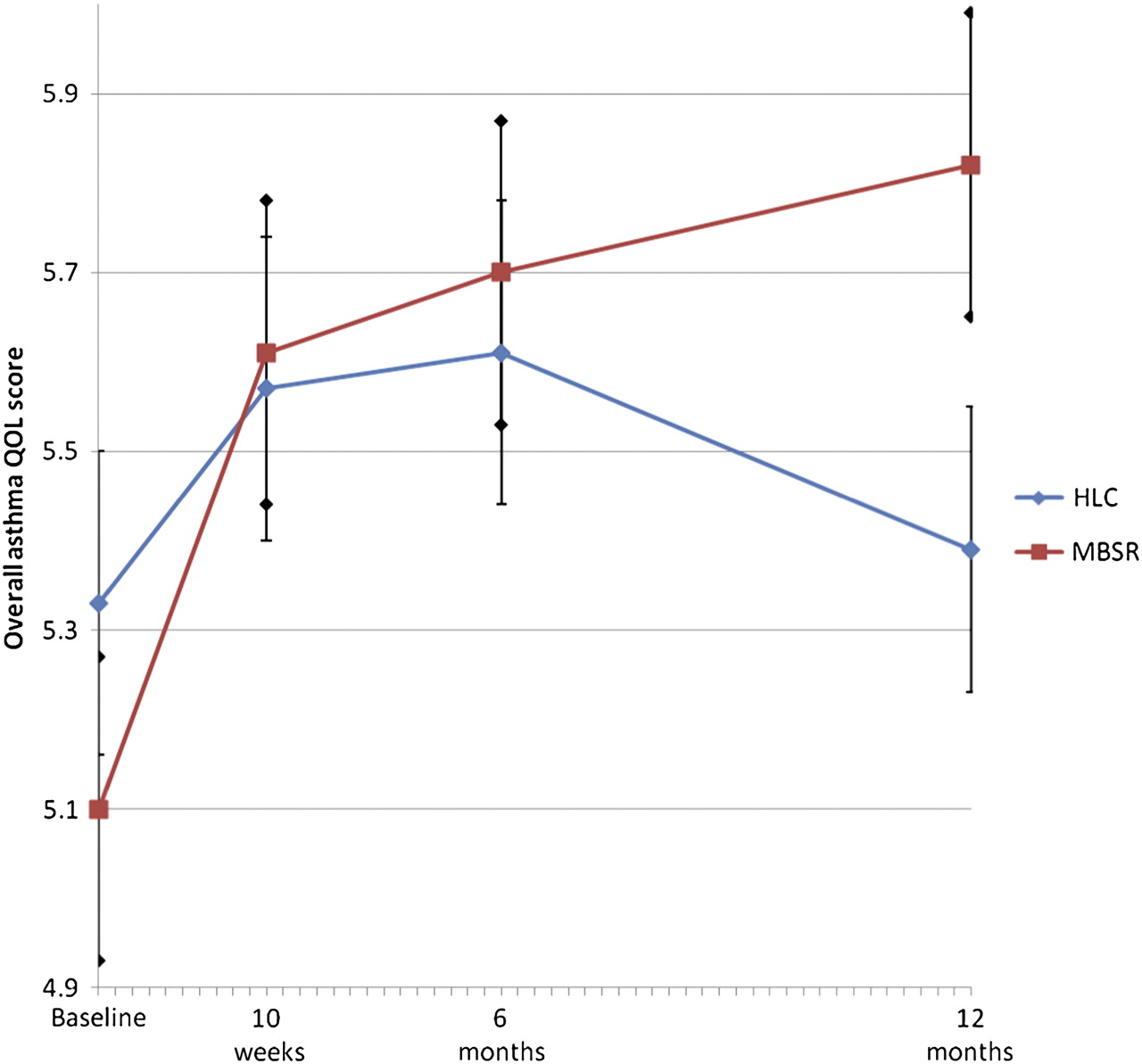
Overall asthma quality of life (AQOL). HLC, healthy living course; MBSR, mindfulness-based stress reduction.
Lung function
The primary lung function measure (2-week average morning PEF (litre/min)) did not improve in the MBSR group compared with controls; changes from baseline were −4.2 and 6.5 respectively (differential change at 12 months −10.7, p=0.588) (see table 3). Similarly, effects were not demonstrated in PEF variability (amplitude % mean) or FEV1 (litres), with respective changes of −0.27% in the MBSR group and −0.05% in the control group (differential change of −0.22%, p=0.879), and 0.04 in the MBSR group and 0.02 in the control group (differential change of 0.01, p=0.809) (see table 3). Adherence to PEF monitoring, defined as completing at least one full day of monitoring, was 78% at 10 weeks, 77% at 6 months and 78% at 12 months.
Lung function: model estimates for baseline, follow-up and change from baseline
Secondary outcomes
Asthma control
The percentage of well controlled asthma in the MBSR group went from 7.3% at baseline to 19.4% at 12-month follow-up compared with 7.5% to 7.9% in the controls. This differential change was not significant (p=0.301) (see table 4 and figure 3).
Asthma control, perceived stress, rescue medication and prednisone use: model-derived estimates for baseline, follow-up, and follow-up versus baseline

Asthma control. HLC, healthy living course; MBSR, mindfulness-based stress reduction.
The percentage of patients in the MBSR group using long-term controller medication decreased from 80.5% at baseline to 71.4% at 12-month follow-up, while the percentage of controls increased from 74.4% to 81.25%. This differential change was not significant (p=0.064) (data not shown).
Perceived stress
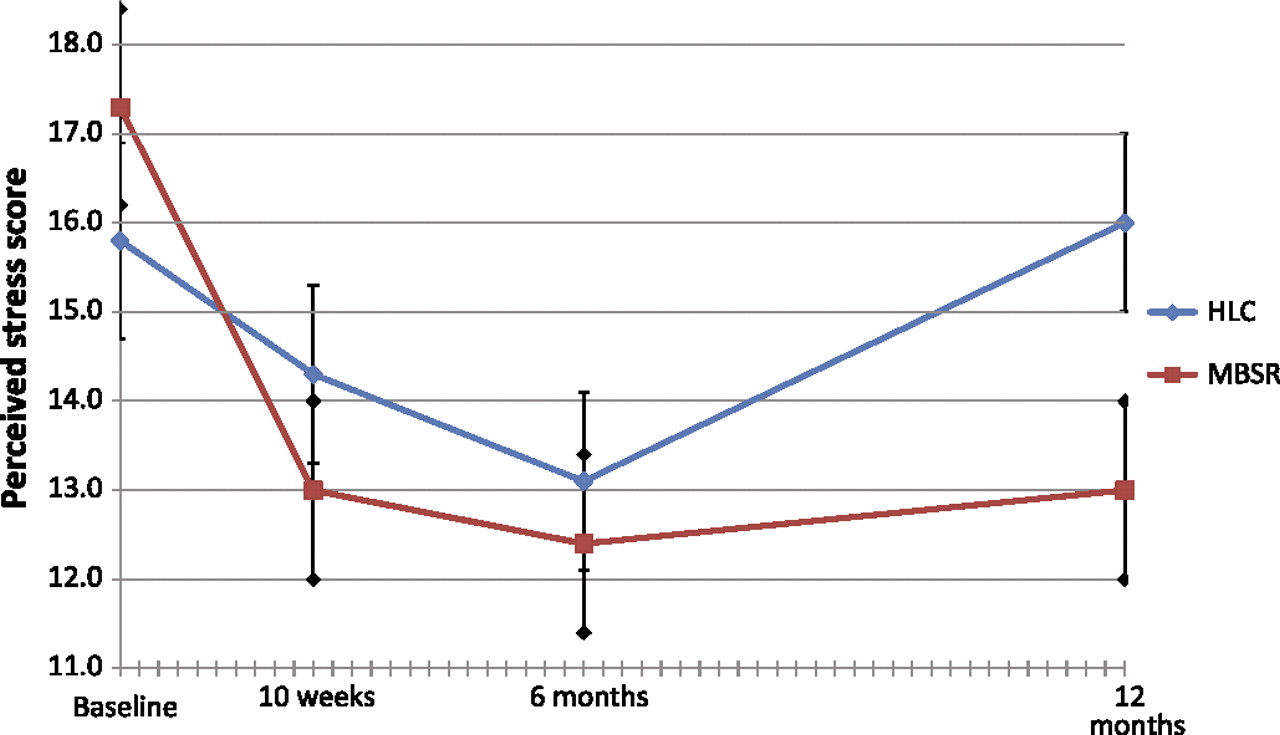
At 12-month follow-up, perceived stress (PSS) had significantly improved in the MBSR group compared with the controls, decreasing by 4.3 and increasing by 0.2 respectively (differential change of −4.5, p=0.001) (see Table 4 and figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Perceived stress. HLC, healthy living course; MBSR, mindfulness-based stress reduction.
Asthma medications, exacerbations, days of work/school missed
In an unadjusted model, there were no significant differences in change between conditions in use of rescue medications (bronchodilators) (p=0.095) or prednisone for asthma exacerbations (p=0.084) (see table 4). However, when adjustment was made for prednisone use in the 30 days before baseline assessment, the MBSR group showed a significant decrease compared with the control group in use of rescue medications at 12 months (p<0.001). There were no differences in long-term controller medication use and no change in use over time overall. There was no difference between conditions in days of work or school missed (p=0.538).
Intervention and control sessions attended
Of the nine programme sessions, the mean number attended was 5.64 in the MBSR group and 4.54 in the HLC group (p=0.047).
Discussion
Participation in an MBSR programme as an adjunct to asthma treatment resulted in enduring, clinically significant improvements in AQOL in patients with persistent asthma.11 For clinical perspective, these are comparable to QOL improvements in trials of widely prescribed asthma medications, including inhaled corticosteroids18 and an anti-IgE antibody.19 Other complementary programmes have not shown similar definitive improvements in asthma QOL,6 suggesting mindfulness training may have uniquely supportive features. The independence of QOL improvements from lung function is consistent with a normative study which also found no correlation between AQOL and lung function.16
It was hypothesised that changes in appraisal and reduced reactivity to asthma symptoms from mindfulness training would increase coping resources and affect QOL through decreases in PSS. A number of findings support this model. Baseline PSS (17.3) in the MBSR arm was at the 75th percentile for a US normative sample17 and was significantly and substantially reduced to the norm (13.0) at 12 months compared with controls, who remained relatively unchanged (from 15.8 to 16.0). Together with the finding that the largest effect in AQOL was in emotional function, this suggests coping resources increased in patients in the MBSR group. The finding of reduced stress has important clinical implications because higher stress levels are associated with increased asthma morbidity, poorer QOL and suboptimal disease management.2
The lack of accompanying improvements in lung function has implications for debate on the causal relation between stress and asthma. Laboratory-induced stress increases airway resistance in patients with asthma,20 but longer-term life stress is not associated with lung function.21 Our findings support the view that life stress, while affecting asthma QOL, may not contribute to impairment in lung function.
An interesting and encouraging finding is the pattern of change between treatment conditions over 12 months. While both conditions tended towards improvement in QOL, stress and asthma control in the first 6 months, the smaller gains achieved by controls largely deteriorated to baseline levels at 12 months. The MBSR programme maintained or improved their gains without further intervention. The HLC programme may have produced an initial placebo effect, a suggestion supported by a recent trial demonstrating some placebo effect of bronchial thermoplasty on QOL in patients with asthma,22 and a cognitive behavioural intervention trial for patients with asthma and panic disorder that found AQOL gains during an 8-week intervention were not sustained at 6 months.23 To our knowledge this is the first randomised trial using an active control that has followed MBSR participants for 12 months. It may be that more accurate discrimination between thoughts, sensations and feelings, and the reduced urgency and distress resulting from non-reactive awareness associated with mindfulness training is a lasting perceptual change.24
The study addresses criticism that studies of mindfulness training25 and complementary programmes used by patients with asthma6 lack credible active controls, include only subjective endpoints, inadequately define participant characteristics and treatment methods, and fail to control for the supportive interaction with a practitioner, the most potent component of non-specific effects in medical encounters.26 While the non-specific effects of the MBSR and control interventions could differ, the finding that increased mindfulness from MBSR programmes mediates reductions in PSS27 adds support to mindfulness training as the active ingredient. Additionally, by enrolling participants in a widely available programme rather than an experimental programme tailored to patients with asthma, the study addresses the more general criticism that behavioural trials create intervention conditions that are not generalisable, or translatable into the ‘real world’. It is reasonable to expect similar findings in the approximately 200 MBSR programmes available at US and European healthcare facilities, many of which are covered by third party payers, making this a realistic adjunctive asthma treatment.
There were a number of study limitations. The modest sample size of this pilot study limited power to detect differences in a number of variables, including asthma control, and the ability to detect whether the intervention effect was specific to patients with asthma of a particular severity and whether it was related to changes in concomitant medications. Also, a substantial number of results have been calculated in a fairly restricted dataset; some results may be due to chance, especially when p values are close to 0.05. Generalisability of the findings is limited by a number of factors. First, patients were recruited from a pulmonary medicine and primary care population in an academic medical centre and may not be representative of the general asthma patient population. Second, refusal rate was high among eligible patients (71%), raising concerns about the self-selected nature of the sample. However, while our rate is higher than some other randomised controlled trials of behavioural interventions (approximately 37%)28 ,29 it is similar to the 75% who declined a randomised controlled trial of a behavioural programme for asthma.30 The challenge of recruiting participants to clinical trials is widespread, with many factors involved in refusal that may have little to do with the generalisability of the intervention.31 ,32 The most frequent reason for declining to participate in the present study was being too busy to participate in a clinical trial (23%), suggesting the trial requirements were a barrier, rather than a rejection of the intervention itself. Third, the majority of patients in the trial were white, non-Latino and of higher socioeconomic status. Lastly, attendance at five of the nine MBSR sessions suggests its traditional delivery may not be suitable for people with a chronic illness, and that a shorter programme may be equally effective.33
Acknowledgments
We gratefully acknowledge the technicians in the UMMHC Pulmonary Diagnostic Laboratory for conducting the spirometry, and Dr Sarah Reiff-Hekking for conducting the Healthy Living Course (compensated financially for their work on this study).
References
Footnotes
Funding Study supported by grant R21 AT002938 (awarded to Drs Pbert and Carmody) from the NIH National Center for Complementary and Alternative Medicine. The sponsor provided financial support only and had no role in the design, conduct, data collection, management, analysis, and interpretation of the study; or in the preparation, review, or approval of the manuscript.
Competing interests None.
Ethics approval Ethics approval was provided by the Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Drs Pbert and Carmody had full access to all of the data and take responsibility for the integrity and the accuracy of the data and analysis.
Linked Articles
- Airwaves