Article Text

Statistics from Altmetric.com
Case presentation
A 55-year-old previously fit and well woman was admitted with a 4-week history of dry cough and 1-week history of progressive breathlessness. She had never smoked, was on no regular medications and there was no history of heart disease, malignancy, rheumatological disease or tuberculosis.
Physical examination revealed signs of a moderate right-sided pleural effusion but was otherwise unremarkable. Full blood count, clotting, and renal and liver function tests were normal. C reactive protein was <5 mg/l. Chest x-ray revealed a moderate right sided pleural effusion.
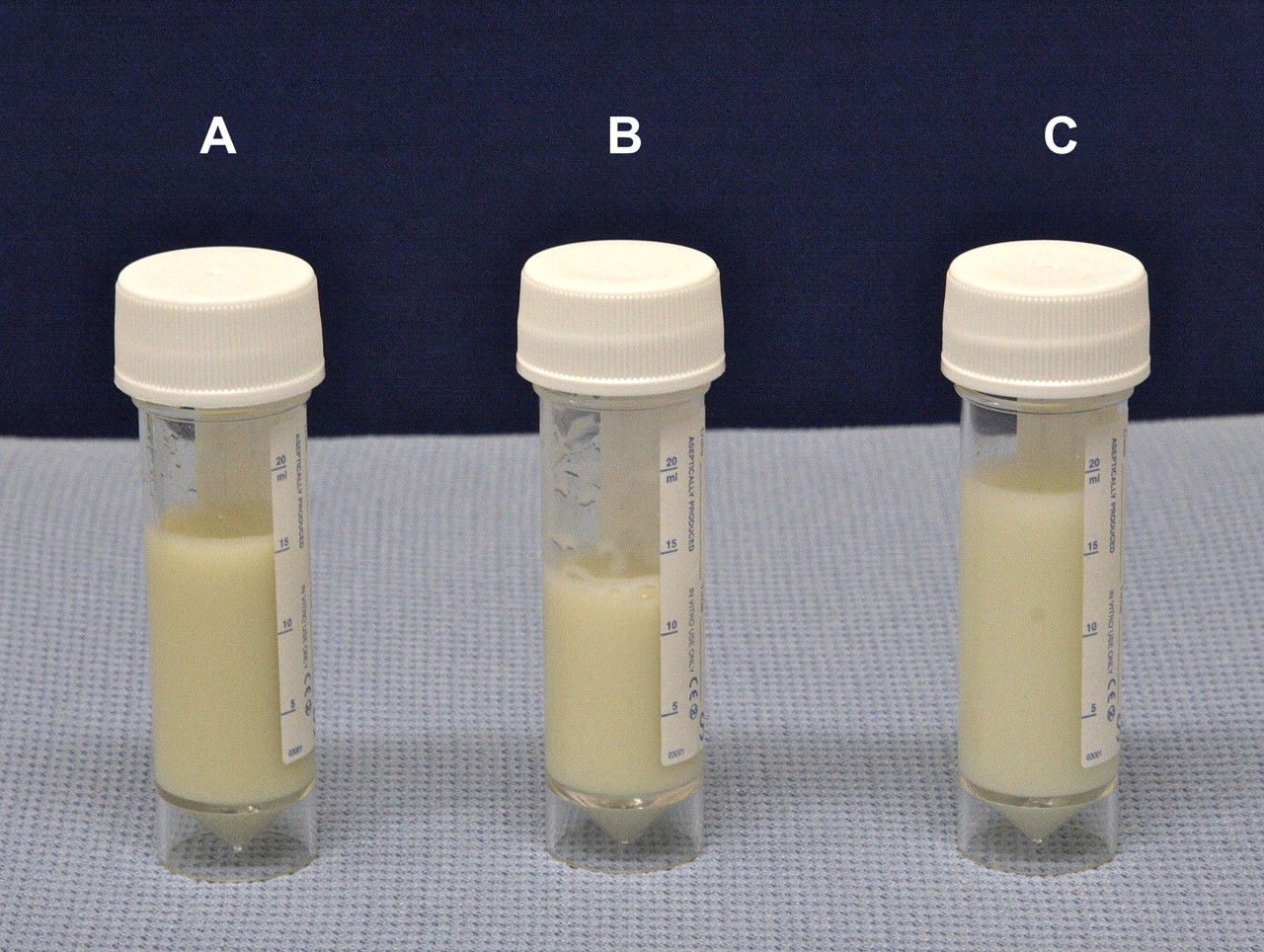
She underwent bedside diagnostic aspiration of 50 ml of pleural fluid which macroscopically appeared cloudy (figure 1A). The sample was centrifuged (figure 1B) and subsequently 10 ml of ethyl ether was added (figure 1C). Results of pleural fluid biochemistry were as follows: protein 68 g/l, lactate dehydrogenase 2030 IU/l, glucose 1.8 mmol/l, pleural fluid cholesterol was 11.2 mmol/l (normal range 3.5–6.5 mmol/l) while triglyceride level was 1.8 mmol/l (normal level <2 mmol/l). Gram's stain was negative and there was no growth on culture. Pleural fluid smear for acid-fast bacilli was negative. A sample was sent for cytological examination (figure 2).

(A) Cloudy pleural fluid on aspiration. (B) Lack of clearing after centrifugation. (C) Lack of clearing on addition of ethyl ether.

{kind=link}
{kind=link}
Cytological examination of pleural fluid demonstrating large numbers of rhomboid shaped cholesterol crystals.
CT thorax revealed a moderate right-sided pleural effusion with minimal pleural thickening. The patient was referred for a video-assisted thoracoscopic surgery (VATS) pleural biopsy. On inspection of the pleura on VATS, both visceral and parietal pleurae were found to be mildly thickened. Multiple pleural biopsies were taken and she was discharged 4 days after the procedure.
Question
What is the diagnosis?
See page 659 for the answer
Answer
From the question on page 658
The lack of clearing of cloudy pleural fluid either with centrifugation (cf. empyema) or with the addition of ethyl ether (cf. chylothorax) raises the suspicion of pseudochylothorax. An alternative to centrifugation is to simply let the sample stand on the bench for an hour. The diagnosis of pseuodochylothorax was confirmed by the presence of typical rhomboid shaped cholesterol crystals on cytological examination and elevated cholesterol level with normal triglycerides on pleural fluid biochemistry.
Histology on the pleural biopsy specimens revealed chronic inflammation without definite evidence of granulomas and Mycobacterium tuberculosis complex was isolated on pleural fluid culture confirming that this was a tubercular pleural effusion presenting as a pseudochylothorax. Standard four-drug anti-tuberculosis treatment was started and the pleural effusion had resolved on follow-up in the clinic.
A pseudochylothorax is a pleural effusion characterised by high cholesterol content and milky pleural fluid. The majority of cases are associated with chronic tuberculous or rheumatoid pleuritis and it is believed that a pleural inflammatory process of at least 5 years is required for its development.1 Such chronicity and thickening are considered to be a prerequisite for a diagnosis of pseudochylothorax and it is very uncommon to be able to grow M tuberculosis on culture. To the best of our knowledge, only one case of rapid-onset pseudochylothorax associated with tuberculous pleurisy has been reported previously.2
The source of cholesterol in pseudochylothorax remains intriguing. The conventional belief is that the high concentration of cholesterol in pleural fluid originates from degraded erythrocytes and neutrophils; these are ‘trapped’ in the pleural cavity as fibrosis blocks their drainage via parietal lymphatics. More recently, six cases of arthritis-associated pseudochylothorax have been reported with minimal pleural thickening and a median duration of symptoms of 15 months.3 The authors hypothesise that an active acute or subacute process produces the intrapleural accumulation of cholesterol, rather than the previously suggested cellular breakdown and cholesterol release within an entrapped pleural space.
The lack of significant pleural thickening and the short history in our patient suggests that this may have been the case in our patient. The exact pathogenesis of pseudochylothorax remains a topic for further research.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves