Article Text

Statistics from Altmetric.com
- Solitary fibrous tumour
- pleural
- imaging/CT MRI
- pleural disease
- thoracic surgery
- rare lung diseases
- thoracic surgery
- lung cancer
- lung trauma
- paediatric lung disease
- pleural disease
- pulmonary rehabilitation
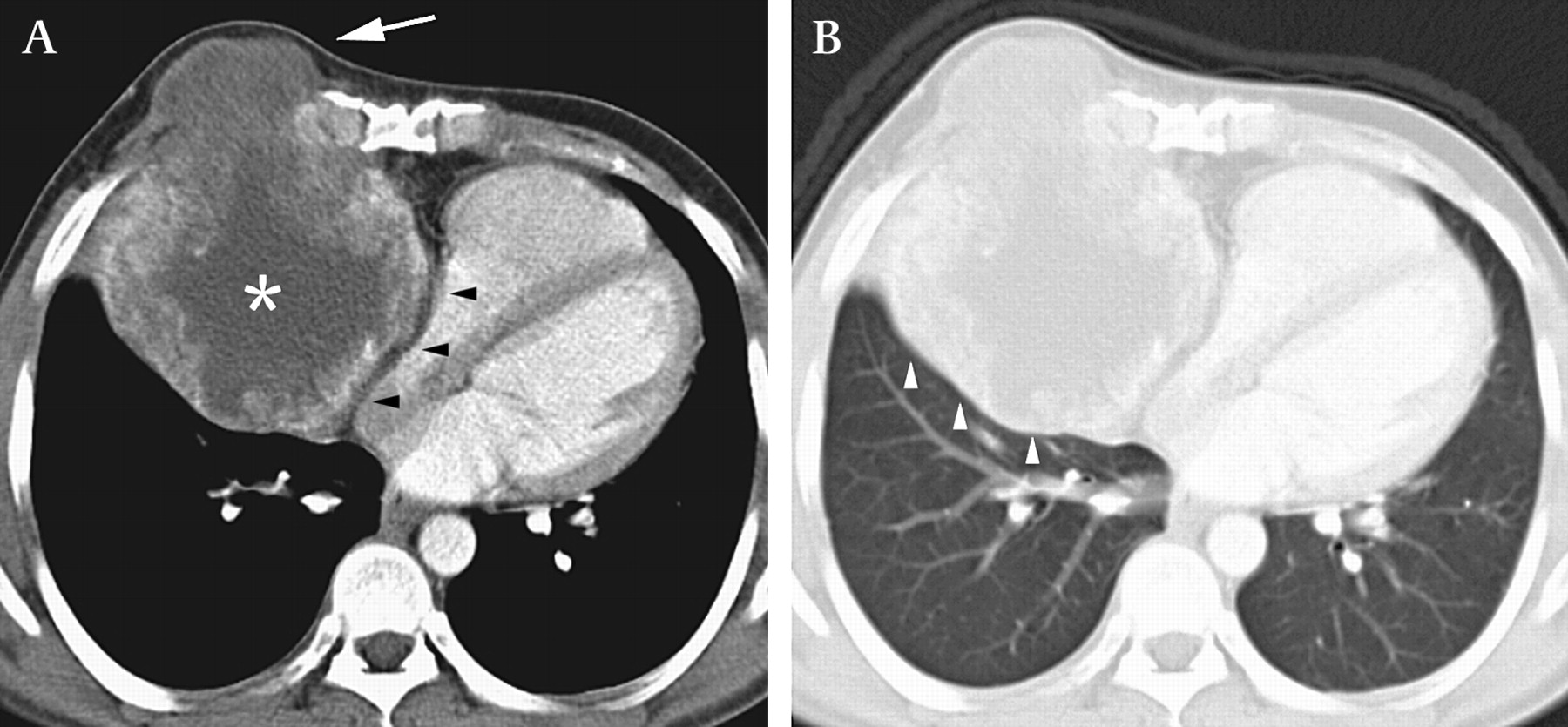
A 44-year-old male patient presented with right chest pain for 6 years, along with progressive swelling in the same region. He did not report fever, weight loss, trauma or previous surgery. On physical examination, a 5 cm focal bulge was observed in the right hemithorax just below and medial to the nipple (figure 1). Chest x-ray showed opacification of the anterior lower third of the right hemithorax (figure 2), which on CT scan corresponded to a heterogeneous mass, compressing the right lung parenchyma and the mediastinum, partially protruding through the chest wall (figure 3). These findings were confirmed by an MRI scan, which also showed that there were no signs of cardiac invasion (figure 4, online supplementary movies 1 and 2). A transparietal biopsy of the mass revealed a proliferative lesion with fusocellular areas. Immunohistochemical examination was compatible with solitary fibrous tumour of the pleura. Surgery was indicated and a heterogeneous pale mass measuring 12.5 cm in diameter was removed confirming the diagnosis (figure 5). Pathology showed an absence of rib or muscular infiltration, while the adjunct lung showed recent haemorrhage. Postoperative recovery was uneventful and the patient was discharged from the intensive care unit on the first postoperative day and from the hospital on the fifth postoperative day.

Focal bulging in the right hemithorax, as seen on physical examination.
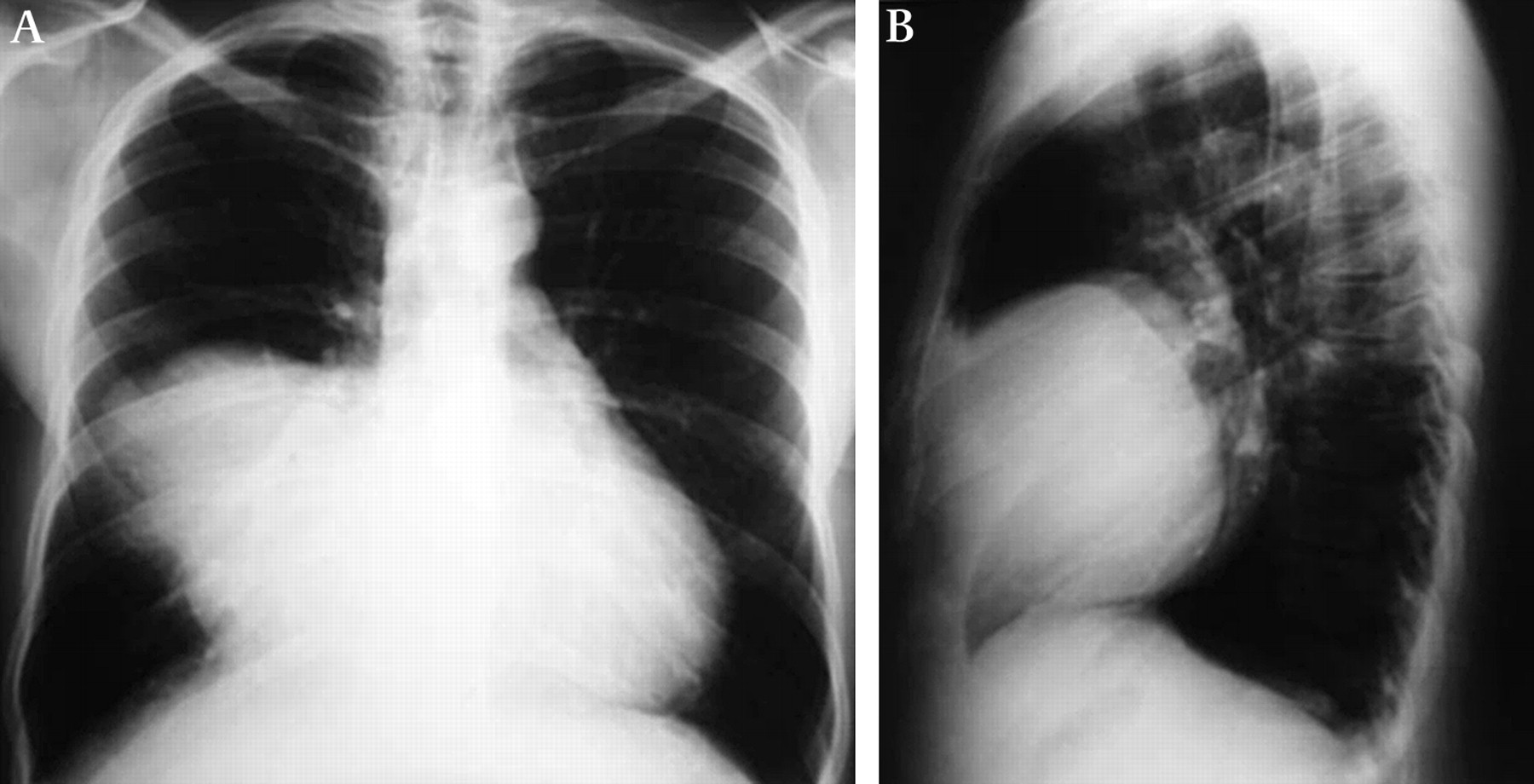
Chest x-ray showing opacification of the anterior lower third of the right hemithorax, with well-defined borders.

CT scan, (A) mediastinal window and (B) lung window, demonstrating a heterogeneous mass (asterisk), compressing the right lung parenchyma (white arrowheads) and the mediastinum (black arrowheads), partially protruding through the chest wall (white arrow).

MR images in the (A and B) axial and (C) coronal planes confirming the findings observed on CT, better demonstrating the protrusion of the lesion through the chest wall (white arrows), between ribs (asterisks), with no signs of cardiac invasion (white arrowheads).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pathological specimen of the resected fibrous tumour of the pleura.
Solitary fibrous tumour of the pleura is an infrequent tumour (5% of pleural neoplasms) originating from mesenchymal tissue and is benign in 80% of cases.1 It affects both sexes equally and is not related to tobacco or asbestos. Its origin may be from the visceral pleura (80%) or from other regions with mesenchymal cells—parietal pleura, pericardium, peritoneum or the tunica albuginea. It is usually asymptomatic, but tumours larger than 10 cm frequently cause non-specific symptoms such as cough, dyspnoea and thoracic pain. Rarely, it causes hypoglycaemia or hypertrophic osteoarthropathy. Malignancy criteria include abundant cellularity, more than four mitoses per 10 fields at high magnification, cytonuclear atypicality, large haemorrhage/necrosis areas, pleural effusion and invasion of adjacent structures. Treatment consists of complete resection when possible, or radiotherapy/chemotherapy in cases with malignant degeneration.2
Acknowledgments
The authors would like to thank Andrea Puchnick for editing assistance.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was approved by the IRB of the Federal University of Sao Paulo.
Provenance and peer review Not commissioned; externally peer reviewed.