Article Text

Abstract
Rationale Placebo responses are complex psychobiological phenomena and often involve patient expectation of benefit. With continuous positive airway pressure (CPAP) treatment of obstructive sleep apnoea, greater hours of CPAP use are associated with reduced sleepiness. However, these open-label studies have not controlled for patient expectation of benefit derived from their knowledge of hours of device use.
Objectives To investigate the relative effectiveness of the use of real or placebo CPAP on daytime sleepiness.
Methods Patient-level meta-analysis combining data on sleepiness measured by the Epworth Sleepiness Scale from three randomised placebo-controlled crossover trials. Mixed model analysis of variance was used to quantify the effects of real versus placebo device treatment, usage, their interaction and regression to the mean.
Measurements and main results Duration of real and placebo CPAP use was correlated within patients (r=0.53, p<0.001). High use of real CPAP reduced sleepiness more than high use of placebo (difference 3.0 points; 95% CI 1.7 to 4.3, p<0.001) and more than low use of real CPAP (difference 3.3; 95% CI 1.9 to 4.7, p<0.0001). High use of placebo was superior to low use of placebo (difference 1.5; 95% CI 0.1 to 2.8, p=0.03). Twenty-nine per cent of the effect of high usage of CPAP (4.2 points; 95% CI 3.3 to 5.1) was explained by the expectation of benefit effect associated with high use of placebo (1.2 points ; 95% CI 0.2 to 2.3).
Conclusions A clinically significant proportion of the effectiveness of high CPAP use in reducing sleepiness is probably caused by patient expectation of benefit.
- Adherence
- compliance
- placebo effects
- dose–response
- psychology
- respiratory measurement
- sleep apnoea
- clinical epidemiology
- oxidative stress
- assisted ventilation
- pneumonia
- rare lung diseases
- non-invasive ventilation
- COPD exacerbations
- emphysema
- asthma
- ambulatory oxygen therapy
- COPD pharmacology
- long term oxygen therapy
- lung physiology
- respiratory muscles
- short burst oxygen therapy
Statistics from Altmetric.com
- Adherence
- compliance
- placebo effects
- dose–response
- psychology
- respiratory measurement
- sleep apnoea
- clinical epidemiology
- oxidative stress
- assisted ventilation
- pneumonia
- rare lung diseases
- non-invasive ventilation
- COPD exacerbations
- emphysema
- asthma
- ambulatory oxygen therapy
- COPD pharmacology
- long term oxygen therapy
- lung physiology
- respiratory muscles
- short burst oxygen therapy
Key messages
What is the key question?
-
How much of the benefit associated with high compliance with continuous positive airway pressure (CPAP) for obstructive sleep apnoea is caused by real treatment effects and how much by patients' expectations of benefit?
What is the bottom line?
-
High use of CPAP does confer real benefits but about 29% of the benefit felt by highly adherent patients in regular clinical care is due to expectation of benefit.
Why read on?
-
Clinical care is a complex psychobiological environment so the benefits that seem to accrue to patients who effectively use treatments are partly caused by real effects of those treatments and partly by the expectations that these highly adherent patients bring with them into the clinical environment.
Poor compliance with medical treatments is a major barrier to clinical effectiveness for many chronic conditions.1 ,2 Recent studies suggest that placebo effects may involve crucial psychobiological factors influencing treatment effectiveness and clinical practice.3 Placebo treatments are not necessarily inert; one principal component is the expectation of future benefit responses following administration of a placebo.3 ,4 Patients who accept treatment are expecting that it will help them. These observations have primarily been made in a range of pharmaceutical and other therapeutic interventions. However, the availability of real and placebo continuous positive airway pressure (CPAP) for obstructive sleep apnoea (OSA) provides an almost unique opportunity to examine the relationships between treatment usage, expectation of benefit, relief of symptoms and the placebo effect, including expectation of benefit.
Unblinded cohort studies have shown a dose–response relationship in which greater usage of CPAP was associated with better symptomatic outcomes for patients.5–8 However, because these studies were open label, patients were largely aware of how many hours a night they had been using CPAP. Therefore it is possible that some of the symptomatic benefit associated with greater use might have arisen from an expectation of benefit.
Randomised placebo CPAP controlled crossover trials provide a method to determine whether the symptomatic response to higher use of CPAP is related to a real effect or expectation of benefit from their high use. Given the complexity of human psychobiology, crossover trials offer a better comparison as patients act very well as their own controls because usage of real and placebo CPAP seems to be highly correlated.9 Placebo control via an almost identical sham device also helps to quantify the size of the expectation of benefit effect associated with using CPAP therapy. We combined three crossover trials9–11 in an individual patient-level meta-analysis to quantify the relative effects of real and placebo CPAP compliance on sleepiness measured using the Epworth Sleepiness Scale (ESS).
Methods
Participants
We combined data from the 91 patients who completed one of the crossover trials. Detailed descriptions of the study designs, patients' characteristics, and primary outcome findings of the studies can be found in the original publications.9–11 Table 1 briefly describes the patients included in the analysis.
Patient characteristics across the three trials
Study design and procedure
Trials were combined as they had congruent study designs with all patients receiving in random order standard individually titrated real CPAP and placebo CPAP (sometimes called ‘sham CPAP’ and simply described here as placebo). In all trials the placebo was identical to the CPAP machine in terms of noise, mask temperature, mask humidity and airflow through the exhalation port. To create a sub-therapeutic treatment, the placebo machine was set to 8 cm H2O, yet delivered <1.0 cm H2O pressure. The datasets were merged and we analysed the effects of real and placebo treatment and the effects of greater use of both of these devices on sleepiness as measured by the ESS.12 The ESS was the only outcome in common among the trials.
Data preparation and statistical analyses
Statistical analyses were performed using SAS (V.9.2) and SPSS for Windows (V.17). Continuous variables were presented as mean ± SD or 95% CIs, and p values of <0.05 were considered statistically significant. We considered the interaction of compliance and treatment to be significant when p<0.1 because this was the primary screening method for our hypothesis. The specific group-by-group analyses arising from such an interaction were then judged by the p<0.05 criteria.
We used mixed model analyses of variance (using variance components structure of covariance) to quantify the effects of usage (high vs low cut at 4 h/night) and the interaction between treatment and compliance. These models also included the effects of treatment (CPAP or placebo) and regression to the mean (the baseline severity in ESS). A priori we specifically tested the following: the superiority of high CPAP use compared with high placebo use; the superiority of high CPAP use compared with low CPAP use; and the superiority of high placebo use compared with low placebo use (all using p<0.05 as the critical threshold level). Inter-trial and inter-individual variability were classified as random effects; all previous variables (treatment, compliance, regression to the mean, and the interaction between treatment and compliance) were fixed effects. We also estimated the proportion of improvement associated with high use in clinical practice that is probably attributable to expectation of benefit by dividing the effect associated with high placebo use by the effect associated with high CPAP use. Effect sizes were calculated by dividing the mean effects by the SD of the ESS, which is often around 4 points in clinical and population samples. Small effect sizes are between 0.20 and 0.50, medium between 0.50 and 0.80, and large over 0.80.13
These main analyses were conducted using compliance as a dichotomous variable based on compliance cut-off at the standard 4 h/night. In a second model we investigated the relationship between outcome and compliance as a continuous variable using the mixed model analysis described above. In sensitivity analyses we tested different dichotomous cut-off points and whether the order the treatment was given may have influenced our final conclusions by using an order and an order by treatment interaction in our final model. We also examined the correlation between CPAP and placebo use.
Results
Correlation between placebo and real CPAP compliance
Real and placebo device usage was correlated (r2=0.53, p<0.001; see figure 1). Individuals who used placebo for more than 4 h/ night were also very likely to be high CPAP users with only three of those patients having compliance below 4 h when on CPAP (see figure 1).

Patient use of treatment is stable between a real continuous positive airway pressure (CPAP) device and a placebo version of the same device (r2=0.53, p<0.001). X and Y axes are in units of average hours per night of use.
Epworth Sleepiness Scale (ESS)
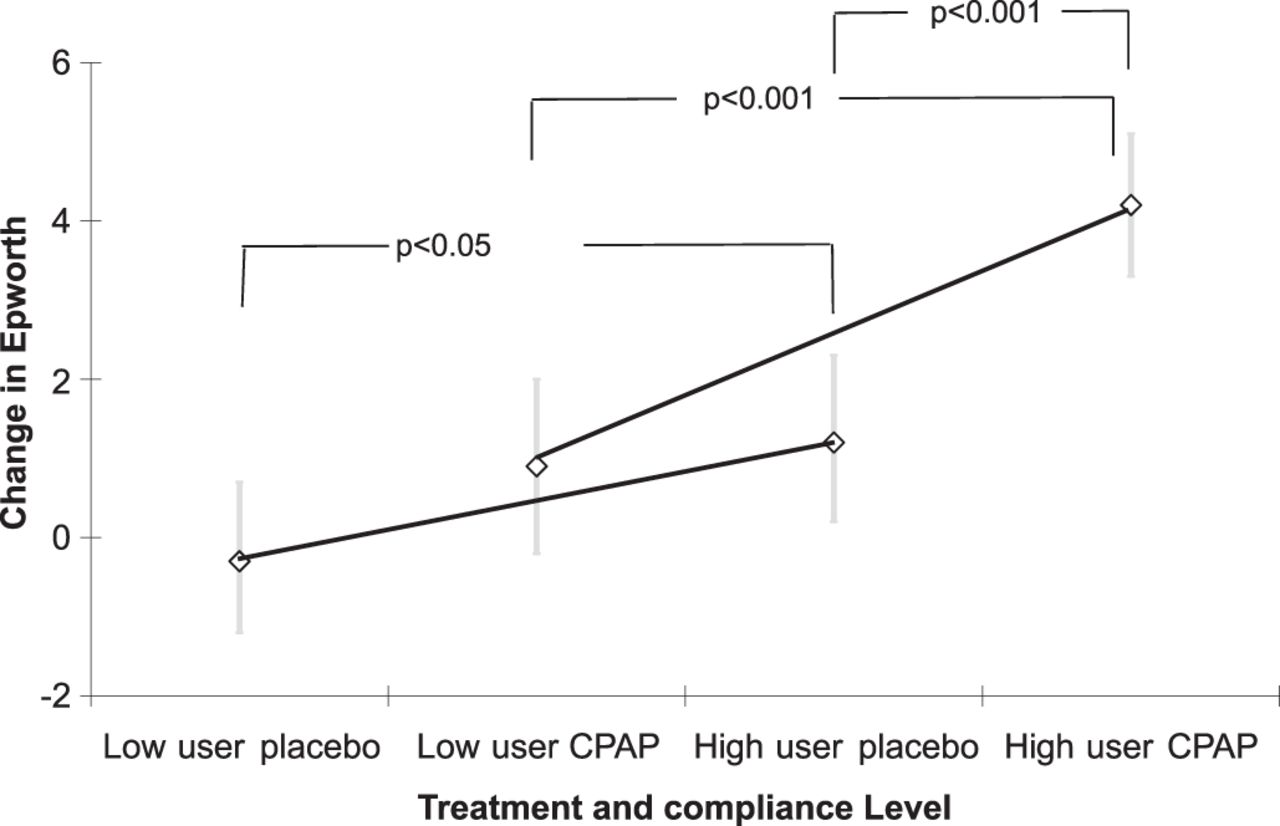
High use was associated with superior improvement in the ESS across both treatments (mean difference 2.2 points; 95% CI 1.0 to 3.3, p<0.001; effect size (ES) based on a SD of 4 points 0.55). Real CPAP improved sleepiness more than placebo irrespective of usage (2.1; 95% CI 1.1 to 3.0, p<0.001; ES 0.53). The interaction between hours of usage and type of treatment (real or placebo) was significant (p=0.056), using a significance threshold level of 0.1 for investigating the specific comparisons of interest. The effect on ESS of high use of real CPAP was greater than higher usage of placebo CPAP (difference 3.0 points; 95% CI 1.7 to 4.3, p<0.001; ES=0.75) and low use of CPAP (3.3; 95% CI 1.9 to 4.7, p<0.0001; ES=0.83). Additionally, high placebo use was better than low placebo use (1.5; 95% CI 0.1 to 2.8, p=0.03; ES=0.33). These effects were not influenced by order or order by treatment interaction. These results are presented in table 2 and figure 2.
Effects of high and low CPAP and placebo use on sleepiness

{kind=link}
{kind=link}
Effects of different treatment types and use on improvements measured by the Epworth Sleepiness Scale (ESS; y axis is in points of improvement from baseline in the 24-point ESS). Diamonds indicate the estimated mean effects (bars the 95% CI). High use (>4 h/night) of either machine confers greater benefits but the symptomatic benefits accruing to high users are greater when using real CPAP than placebo CPAP. CPAP, continuous positive airway pressure.
High use of CPAP was associated with a 4.2-point reduction in Epworth score (95% CI 3.3 to 5.1 points, p<0.0001) and high use of placebo was associated with a 1.2-point reduction in Epworth score (95% CI 0.2 to 2.3 points, p=0.03). As such, we estimate about 29% of the improvement in Epworth scores associated with high CPAP compliance seen in clinical practice is probably attributable to expectation of benefit in patients who are high users of CPAP (ie, 1.2 points on high-use placebo divided by 4.2 points on high-use CPAP).
We also investigated usage as a continuous linear variable. In these models, both treatment and usage were significantly related to Epworth improvement in the expected direction (mean estimate 2.1 points (95% CI 1.2 to 2.9) and 0.6 points per hour (95% CI 0.3 to 0.9), respectively, both p<0.0001). In contrast to the findings in the dichotomous model, there was no significant interaction between treatment type and usage duration (p=0.54). In other words, the effect of duration of use, measured as a continuous linear variable, on ESS did not significantly differ between CPAP and placebo devices.
In sensitivity analyses we analysed the cut-off points for high and low use using 5, 6.5 and 7.5 h/night. The combination of these analyses, plotting raw data and fitting curves to the data indicated the likely existence of no additional benefit beyond about 5.5 h, but with significant uncertainty about the exact location of the asymptote (see online supplementary figure).
Discussion
Using data from three randomised placebo CPAP controlled crossover trials, we estimate that 29% of the reduction in sleepiness seen in patients with OSA who use CPAP for more than 4 h a night is probably caused by an expectation of benefit. The expectation of benefit is one of the components of the placebo effect and is caused by patients inferring benefit from treatments they choose to use. Conversely, patients who do not use treatments do not expect to feel better. Because clinical interaction is such a complex psychobiological phenomenon, these effects are best quantified in randomised crossover trials in which patients act as their own controls and tend to use the active treatment (CPAP) as often as they use the placebo.
Previous open-label cohort studies5–7 and parallel design clinical trials14 ,15 have shown that there is a dose-dependent association between greater use of CPAP and better patient outcomes.16 We analysed three placebo CPAP controlled randomised crossover trials to distinguish between symptom improvement resulting from real treatment use from improvement related to placebo-like expectation of benefit for each patient (see figure 2 and table 2). As expected, real CPAP had a beneficial effect over placebo as did high use of either device compared with low use. Fortunately, not all of the benefits of high use were driven by expectation of benefit as patients using CPAP for more than 4 h a night had greater reduction in sleepiness than patients using placebo for more than 4 h/night. We infer expectation of benefit effects because patients using placebo for more than 4 h a night exhibited greater reduction in sleepiness than patients who used placebo for less than 4 h a night, despite this device having no physiological effect on OSA. These high users of placebo were also 94% likely to be high users of CPAP (46 out of 49, see figure 1) indicating the existence of a compliant patient phenotype who will use the device regardless of its ability to control OSA. Conversely, there were also patients who used placebo CPAP less than normal CPAP (see the lower right quadrant of figure 1). This may be further evidence that patients who feel benefit from CPAP treatment tend to use it more.5
The main effect reported here cannot be observed in clinical practice because patients in routine clinical care are not given placebo CPAP therapy. Additionally, placebo devices are not commonly employed in crossover trials due to a fear of unblinding,17 so the number of clinical trials available for this sort of analysis is limited.
The uncertainty about whether the dose effect is linear, stepped or asymptotic led us to treat compliance as a dichotomous (the widely used 4 h/night threshold value) and a continuous hours of use variable.6 When compliance is treated as a continuous linear variable in the same models, treatment with CPAP and high usage confer significant benefits. However, the non-significant interaction term in that linear model indicates that the use effects of CPAP and placebo do not differ in a way that is consistent with a linear-dose response. In sensitivity analyses we dichotomised hours-of-use data at different cut-off points (5, 6.5 and 7.5 h) and additionally visually plotted the raw data (see online supplemental figure). These analyses raised questions about the linearity of the relationship between compliance and symptomatic improvement. Thus we can also confirm previous reports that after controlling for placebo effects, the association between compliance and better patient outcome is weaker than expected5 and may not be linear6 as benefit ceases to accrue at an asymptote of about 5.5–6.5 h per night.
Figure 1 shows patients using the real or placebo device for similar lengths of time. Whether this ‘high-use’ trait might generalise between CPAP and pharmacological compliance is the subject of conflicting reports.18–20 Additionally, the possibility of modifying psychological characteristics of non-compliance with CPAP treatment should continue to be the subject of clinical trials (eg, Richards et al 21 and ACTRN: 12606000065594). The characterisation of patients into ‘high’ and ‘low’ users is defensible because CPAP compliance is often bimodally distributed (see figure 1 and the relative paucity of data points centred around 4 h compared with 0–2 hours and 6 h). However this classification may still be flawed as recent investigations of both pharmacological treatment of epilepsy and CPAP indicate there may be more than two compliance phenotypes.22 ,23
The use of crossover trials with placebo control offers only a partial solution to the problem that patients are aware of (unblinded) their ‘dose’ of treatment. A trial in which patients are randomised to 2, 4, 6 or 8 h/night of effective treatment might offer superior data to the data presented here. Our approach of using each patient with their highly correlated9 use of CPAP and placebo to act as their own control offers an advance on previous analyses. However, such highly selected and motivated patients may not be generalisable to normal clinical populations. Data from clinical trials and unselected cohorts provide useful clinically applicable information when used together. However, we were limited by the availability of only one subjective outcome variable and by the small numbers of patients (n=91) participating in these technically challenging clinical trials. Two of the trials did not have second-arm baseline measurements10 ,11 and one did not have a washout period,11 which might have affected the results. The Australian-based study10 also had lower baseline ESS scores than would be expected for a symptomatic clinical sample and this may have made it more difficult to detect treatment and use differences because of a possible floor effect. One of the implications of this effect is that in patients in clinical practice who have very high ESS scores, the dose–effect relationship may be stronger than reported here and the dose–benefit relationship may extend well beyond the asymptote reported here. More accurate treatment estimates may have been possible if we had measured percentage of sleep with CPAP rather than the crude measure of hours per night, however we lacked a good objective measure of sleep duration. Nevertheless, these data provide an opportunity for understanding aspects of CPAP compliance that have not previously been investigated.
Longstanding efforts to improve compliance to CPAP by employing technological solutions aimed at reducing pressure may be questionable as figure 1 also suggests compliance has little relationship to pressure. This also explains why the two most recent meta-analyses of pressure modification approaches to improving CPAP compliance show little or no compliance benefit and no symptomatic benefit.24 ,25 In this context it is not surprising that the largest effect of any treatment intended to increase use of CPAP therapy tested in a randomised trial has been cognitive behavioural therapy.21
Summary
This patient-level meta-analysis of three randomised placebo-CPAP-controlled crossover trials for patients with OSA confirms that high use of CPAP provides greater sleepiness reduction benefits than high use of a placebo device. Interventions that improve CPAP use from low levels (ie, less than 4 h/night) are likely to result in real benefits for patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Footnotes
A version of this study has been presented in poster format at the 20th Congress of the European Sleep Research Society, Lisbon, Portugal, September 2010, at the Australasian Sleep Association meeting in Christchurch, New Zealand, October 2010 and at the World Sleep Federation meeting in Kyoto, Japan, October 2011.
Funding The Health Research Council of New Zealand (grant 00/285); The National Health and Medical Research Council of Australia (grants 202916; 301936; 457355; 571179; 571421 and 512498); British Heart Foundation (grant 2001).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.