Article Text

Abstract
Background Exposure to air pollution in early life contributes to the burden of childhood asthma, but it is not clear whether long-term exposure to air pollution can lead to asthma onset or progression in adulthood.
Objectives The authors studied the effect of exposure to traffic-related air pollution over 35 years on the risk for asthma hospitalisation in older people.
Methods 57 053 participants in the Danish Diet, Cancer and Health cohort, aged 50–65 years at baseline (1993–1997), were followed up for first hospital admission for asthma until 2006, and the annual nitrogen dioxide (NO2) levels were estimated as a proxy of the exposure to traffic-related air pollution at the residential addresses of the participants since 1971. The association between NO2 and hospitalisation for asthma was modelled using Cox regression, for the full cohort and in people with and without previous hospitalisations for asthma, and the effect modification by comorbid conditions was assessed.
Results During 10.2 years' median follow-up, 977 (1.9%) of 53 695 eligible people were admitted to hospital for asthma: 821 were first-ever admissions and 176 were readmissions. NO2 levels were associated with risk for asthma hospitalisation in the full cohort (HR and 95% CI per IQR, 5.8 μg/m3: 1.12; 1.04–1.22), and for first-ever admissions (1.10; 1.01–1.20), with the highest risk in people with a history of asthma (1.41; 1.15–2.07) or chronic obstructive pulmonary disease (COPD) (1.30; 1.07–1.52) hospitalisation.
Conclusions Long-term exposure to traffic-related air pollution increases the risk for asthma hospitalisation in older people. People with previous asthma or COPD hospitalisations are most susceptible.
- Asthma air pollution
- traffic
- long term
- COPD
- asthma epidemiology
- COPD epidemiology
- occupational lung disease
- lung cancer
Statistics from Altmetric.com
- Asthma air pollution
- traffic
- long term
- COPD
- asthma epidemiology
- COPD epidemiology
- occupational lung disease
- lung cancer
Key messages
What is the key question?
Does prolonged living in areas with high air pollution levels cause asthma onset in elderly adults?
What is the bottom line?
Long-varying exposure to traffic-related air pollution in adult life can give asthma.
Why read on?
To find out that people with prior chronic lung disease, in terms of asthma or COPD are most susceptible to the effects of air pollution.
Introduction
Asthma prevalence is increasing in high-income countries,1 including Denmark, where an increase in the severity of adult asthma has been documented.2 The prevalence of asthma in older adults is 6–10% in high-income countries,3 and the economic burden associated with hospital care, medications and years of work lost due to morbidity and mortality is substantial.4 This burden is projected to escalate with the increase in the number of older people with asthma due to enhanced longevity.3 Asthma management among older people has traditionally focused on diagnosis and treatment.5 A comprehensive approach to asthma control in older people should pay special attention to preventing asthma exacerbations, the main determinants of disease severity and costs.6
Air pollution from traffic is ubiquitous in urban environments, as it affects millions of people, and it has been extensively studied in relation to childhood asthma. Despite mixed evidence,7 recent data indicate that air pollution plays an important role in the burden of asthma in children.8 9 It is not known how long-term exposure to air pollution affects asthma in older adults, another susceptible population, partly due to a lack of data from cohorts of older people.
Evidence linking chronic exposure to air pollution and adult asthma is based on studies with self-reported asthma prevalence10 and incidence,11–14 which typically lack information on residential address history, and define long-term exposure to air pollution as a single-year level of nitrogen dioxide (NO2) at recruitment12 or follow-up.11 13 In a Swiss cohort study, the cumulative levels of modelled traffic-related particulate matter <10 μm in diameter over 11 years were associated with asthma incidence, but only in non-smokers.14 The same cohort linked improvements in air pollution levels over 11 years to attenuation of the decline in lung function15 and reduced rates of respiratory symptoms,16 providing important clues about the causality between long-term air pollution exposures and chronic respiratory disease.
We studied the association between weighted mean NO2 concentration at the residence over 35 years and the risk for hospital admission for asthma in a Danish cohort of older people.
Methods
Design and health outcome
The Danish Diet, Cancer and Health cohort17 consists of 57 053 people from Copenhagen or Aarhus aged 50–65 years at baseline (1993–1997) from whom information on diet, education, occupation and lifestyle was obtained using questionnaires. We linked the Diet, Cancer and Health cohort to: the Danish Hospital Discharge Register, dating back to 1976, to identify hospital admissions for asthma (ICD-10: J45–46), chronic obstructive pulmonary disease (COPD) (J40–44), ischaemic heart disease (I20–25) and stroke (I60–63); the Danish Diabetes Register to obtain the date of onset of diabetes; the Central Population Registry to obtain date of death, emigration and residential address history (1971–2006). We defined our primary outcome as the first hospital admission for asthma between baseline (1993–1997) and 2006 for the whole cohort, and additionally studied separately the first-ever asthma hospitalisation, in people without an asthma hospitalisation before baseline, and rehospitalisation for asthma, in people with asthma hospitalisations before baseline. Comorbidity with COPD, ischaemic heart disease, stroke or diabetes was defined prior to admission for asthma.
Exposure assessment
The Danish AirGIS dispersion modelling system18 (described in the online supplement) was used to model outdoor mean annual concentrations of NO2 at the residential addresses since 1971 of the cohort members with an 80% or better residential history (97.6% of the cohort). Missing values due to missing address or missing geographical coordinates were substituted by the levels calculated for the preceding address or, when the first address was missing, for the subsequent address. We thus obtained a complete series of annual mean NO2 concentrations at the residential addresses of each cohort member since 1971, with an average of the 35-year weighted mean NO2 levels, which is the main exposure metric used in this study.
We defined shorter exposure windows with NO2: 15-year mean (since 1991), 1-year mean at baseline and 1-year mean at the follow-up; and proxies based on traffic proximity at baseline residence: the presence of a major road (density ≥10 000 vehicles/day) within a 50 or 100 m radius and traffic load (total kilometres driven by vehicles) within a 200 m radius.
Statistical methods
We applied the Cox proportional hazards model to study the association between hospital admission for asthma and exposure to NO2, with age as the underlying time, event at age at admission for asthma, and censoring at date of death, emigration or 27 June 2006, which ever came first. Models were adjusted for a priori defined confounders, in three steps: (1) age; (2) also including smoking status, duration and intensity, and environmental tobacco smoke at home or work; and (3) also including gender, occupational exposure, obesity and educational level, all defined as in table 1. NO2 levels were log-transformed and modelled as a time-dependent variable. Estimates were presented per IQR. Occupational exposure was defined as working in industries linked to occupational asthma19 from a list of self-reported occupations. The effect modification of an association between NO2 and asthma hospitalisation by baseline characteristics and comorbid conditions was evaluated by introducing interaction terms into the model and tested by the Wald test. The results are presented as HRs with 95% CIs, estimated using Proc PHREG, SAS V.9.2. The dose–response function was produced using a restricted cubic spline in the plot.design function of the R statistical software.
Characteristics of the Diet, Cancer and Health cohort (n=53 695) by first asthma hospitalisation status at follow-up for full cohort
Results
Of the 57 053 people in the cohort, we excluded 571 with a cancer diagnosis before baseline, 962 with missing baseline residential address, 1236 with <80% residential address history available (1971 to end of follow-up) and 589 with missing information on covariates. Of the remaining 53 695 people, 977 (1.9%) had a first hospital admissions for asthma between baseline (1993–1997) and 2006, over 10.2 years' median follow-up (533 234 person-years). Of the 53 143 people without asthma hospitalisation before baseline, 821 (1.5%) had a first hospitalisation over 10.2 years' median follow-up (528 940 person-years). Of the 552 people hospitalised for asthma before baseline, 176 (31.9%) were readmitted for asthma, over 9.5 years' median follow-up (4294 person-years). Of the 53 695 people, 37 836 (70.5%) did not change their address between baseline and the end of follow-up (non-movers).
Women were more often admitted to hospital for asthma (table 1). Current and previous active smoking, passive smoking, employment in occupations related to asthma and obesity were significantly associated with an increased risk, while medium and high educational levels were associated with a reduced risk for asthma hospitalisation (table 1). Patients with COPD and diabetes were significantly more, whereas patients with stroke were less likely to be hospitalised for asthma than persons without these comorbid conditions.
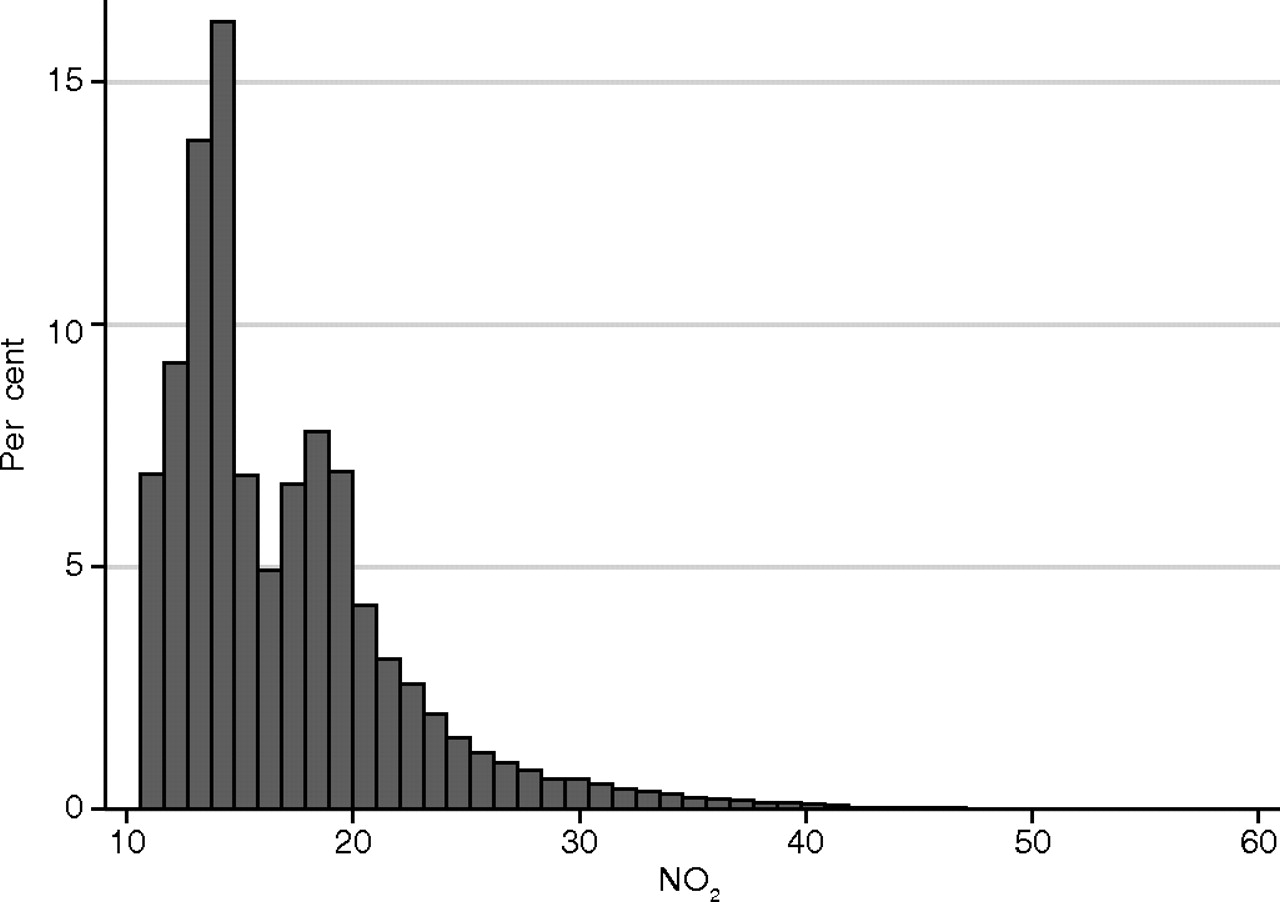
The estimated NO2 levels varied widely (figure 1) with a median of 15.2 and IQR 5.8 μg/m3, and were higher in the 997 asthma cases (16.4 and 6.3 μg/m3). The distribution of alternative traffic proxies is shown in online supplementary table W1.

Distribution of the estimated mean levels of nitrogen dioxide (NO2) at residence for the 53 695 Diet, Cancer and Health cohort members.
We found significant positive associations between NO2 level and first hospital admission in the full cohort (HR per IQR 5.8 μg/m3: 1.12; 1.04−1.22), which was insensitive to choice of confounders (table 2). The associations were similar for the first-ever asthma hospitalisation (1.10; 1.01−1.20), but markedly higher for rehospitalisation in people with a previous asthma hospitalisation (1.41; 1.15−1.71) (p=0.05, Wald test for interaction). The associations indicated a dose–response relationship (figure 2): cohort members living in areas with high (upper quartile) air pollution levels have a significantly higher risk for asthma hospitalisation (30% for first admission and 87% for readmission) than those living in areas with low air pollution levels (lower quartile) (table 2). Sensitivity analyses in the full cohort showed significant or borderline significant associations with alternative definitions of NO2 with HR of 1.11 (1.03−1.20) for the 15-year (since 1971) mean, 1.08 (1.00−1.17) for the 1-year mean at baseline (1993−1997) and 1.18 (1.09−1.28) for the 1-year mean at follow-up (asthma admission), and similar results with the first-ever hospitalisations and rehospitalisations (online supplementary table W2). No associations were detected with traffic proximity proxies at baseline residence in non-movers (online supplementary table W2).
Association between exposure to nitrogen dioxide (NO2) and first asthma hospital admission after baseline (1993–1997) in the Diet, Cancer and Health cohort

{kind=link}
{kind=link}
Association between exposure to nitrogen dioxide (NO2) levels at residence and asthma hospitalisation (log relative hazard with 95% CI) for the 53 695 Diet, Cancer and Health cohort members, adjusted for smoking status (never, previous, current), smoking intensity, smoking duration, environmental tobacco smoke, occupational exposure, gender, body mass index and educational level.
The risk for asthma hospitalisation associated with NO2 was four times higher in people with previous COPD hospitalisations (1.30; 1.07−1.52), with significant effect modification (p=0.04).
Our results were not sensitive to the inclusion of the time under study in the model as a non-parametric term, in order to adjust for possible secular changes in air pollution over the follow-up time.
Discussion
The risk for asthma hospitalisation in this cohort of older people was significantly positively associated with increasing levels of NO2 assessed over 35 years at their residences, and was most pronounced for people with a previous asthma or COPD hospitalisation.
This is the first study to relate the hospital admission for asthma to long-term exposure to air pollution. Our results are generally in agreement with those of asthma prevalence10 and incidence,11–14 but formal comparisons are limited due to different definitions of asthma and air pollution exposure. Whereas doctor-diagnosed asthma was used as an outcome in a single study,11 others relied on self-reports.10 12–14 Asthma is a chronic disease of complex phenotype and recurring symptoms, and it is difficult to define its presence or absence at a definite point of time or to identify its time of onset.20 The rates of self-reported asthma depend on awareness of asthma in the population studied1 and are, especially in epidemiological surveys specifically of respiratory disease,10 12–14 subject to recall and information bias. Similarly, the self-reported onset of asthma is often loosely defined and subject to recall bias.11–14 Overdiagnoses of asthma by primary care physicians, estimated at about 30%,21 is another source of bias, due to the widespread practice of symptoms-based diagnosis without objective measurements of reversible airflow obstruction. Hence, the use of an objective measure of asthma by means of hospital admission from a nationwide register is appealing. Asthma requiring hospital admission is mainly at the severe end of the disease spectrum and is traditionally confirmed by objective measurements of lung function and reversible airflow obstruction in Danish hospitals. The specificity of asthma diagnoses in the Danish Hospital Discharge Register was found to be as high as 0.98,22 validating their use in epidemiological studies.
An important limitation of this study is that asthma hospitalisation is not an accurate marker of asthma onset and under-represents the real asthma burden, as asthma often remains undiagnosed for many years and only a fraction of asthma patients are hospitalised. Rather, the first hospitalisation for asthma should be regarded as a hallmark of asthma progression to a more severe stage or exacerbation. Owing to the lack of self-reports of asthma, we were not able to define the incidence of asthma in this cohort.
Assigning individual exposure to air pollution with high spatial (address-specific) and temporal (annual mean) resolution and assessment over 35 years is a novel approach. Typically, single-year mean NO2 levels were assigned at the residential address at recruitment10 11 or follow-up,12 13 neither of which captured the dynamics of the exposure history. Furthermore, higher risk estimates were observed in non-movers,13 14 suggesting that greater precision in exposure assignment would improve the chances of detecting associations with asthma. We found significant positive associations for asthma admissions with all definitions of the mean NO2 reflecting different exposure windows, detecting almost identical but slightly smaller HRs with the 15-year mean (since 1991) (1.11; 1.03–1.20) than with 35-year mean (since 1971) (1.12; 1.04–1.22), attenuated HRs with the 1-year mean at baseline (1.08; 1.00–1.17) and enhanced HRs with 1-year mean at the follow-up (1.18; 1.09–1.28) (online supplementary table W2). Correlation between the 35-year mean (since 1971) and the 15-year mean (since 1991) and the 35-year mean and the 1-year mean at the follow-up, respectively, was high (correlation coefficient r=0.92 and 0.88). It is likely that the performance of the dispersion model estimating NO2 levels was poorer longer back in time, owing to the higher uncertainty of model input data such as emission factors and traffic counts. Thus, we cannot discern whether the stronger associations with NO2 levels at follow-up, when compared with the 35-, 15- and 1-year means at baseline, reflect the relevance of more recent exposures for asthma hospitalisation or merely the better performance of the dispersion model in more recent years. However, we found no significant associations with traffic proximity proxies at baseline residence (online supplementary table W2), implying that these naive surrogates of long-term exposure to air pollution are inferior to the modelled levels of NO2, as observed earlier,14 and that the modelled air pollution exposure was a likely condition for detecting associations in this study.
We were not able to estimate early-life exposures to air pollution in this cohort, and do not know how these relate to adult-life exposures and how much their inclusion would affect our estimates. Early-life exposures have an adverse effect on asthma in childhood,7–9 but no data have yet examined the relevance of life-time exposures on the risk for asthma in adulthood.
We cannot conclude from our data whether traffic-generated gas and airway irritant NO223 are relevant agents or merely indicators of other traffic-related pollutants, such as particulate matter. Stronger evidence suggests that particulate matter capable of triggering inflammation and inducing oxidative stress24 may be a responsible agent. Studies on humans in exposure chambers25 and of real-life exposures26 illustrated that diesel exhaust can provoke increased airway resistance and bronchial inflammatory changes. Repeated inhalation injury of lung tissues by long-term exposure to air pollution is believed to be central to the exacerbation of asthma.24 However, some of the observed effects could possibly be ascribed to the short-term effects of increases in air pollution on the days prior to asthma admission,27 which, perhaps in synergy with accumulated chronic effects, provoke asthma exacerbation. Discerning acute from chronic effects of air pollution on asthma is important to understand the underlying mechanisms and warrants more studies in cohorts with available daily measurements and individual level air pollution data.
The association between NO2 and asthma hospitalisations was strongest among previous and current smokers and people exposed to environmental tobacco smoke (table 3), in agreement with Jacquemin et al13 and in contrast to Künzli et al,14 who detected associations between air pollution and asthma only in non-smokers. We cannot exclude the possibility that the observed results reflect misclassification of asthma as COPD, which is more strongly related to smoking than asthma, or residual confounding in our estimates due to inadequate adjustment for smoking; however, this is unlikely, as in other studies of this cohort smoking has shown the expected associations with COPD28 and lung cancer,29 indicating that the data on smoking are of high quality. Our results rather suggest modification of the effect of air pollution by smoking, hinting at additive harmful effects of smoking and air pollution on asthma. The biological plausibility of the additive effects of synergistic exposure to tobacco and air pollution particles on asthma is supported by a study showing more rapid loss of lung function in smokers with asthma than in non-smokers with asthma.30 Künzli et al14 attributed the lack of an effect in smokers due to a very marginal contribution of air pollution to the development of asthma in smokers. These conflicting results merit more research on the effects of joint exposures to air pollution and tobacco smoke on asthma development and progression.
Modification of associations* between NO2 (per IQR of 5.8 μg/m3) and first asthma hospital admissions (n=977) by baseline characteristics and comorbid conditions among the 53 695 Diet, Cancer and Health cohort participants
We found a threefold to fourfold enhancement in the effects of exposure to NO2 on asthma admissions among people with previous asthma or COPD hospitalisation, respectively, when compared with those without chronic lung disease. Although asthma and COPD have distinct risk factors and clinical phenotypes, establishing a clear separation between the two is difficult. They are both inflammatory disorders, and often coexist, with both chronic and reversible airway obstruction being present, resulting in misdiagnoses of the two conditions.31 Although objectively measured lung function is required for discharge diagnoses of asthma and COPD, and reversible airway obstruction is usually required for a discharge diagnosis of asthma in Danish hospitals, it is likely that some of the asthma patients in this study also had an irreversible component of airway obstruction. Previously, we have found slightly weaker associations between NO2 and first-ever COPD hospital admission to that observed with first-ever asthma admission in this study,28 implying comparable effects of long-term exposures of air pollution on both COPD and asthma. Finally, the observed associations in this study were not sensitive to the exclusion of 452 people with COPD hospitalisations before baseline (HR for the 35-year NO2 mean: 1.11 (1.02–1.21) in the full cohort, 1.10 (1.01–1.21) and 1.29 (1.03–1.60) in those without and with asthma hospitalisations before baseline, respectively).
Our results suggest that air pollution exacerbates asthma leading to rehospitalisation in those with prior asthma or COPD hospitalisations to a greater extent than it causes new asthma hospitalisations. Increasing susceptibility with age, due to accelerated loss of lung function,30 and increasing prevalence of asthma and comorbid conditions3 including COPD suggest that the effect of air pollution is even greater in the oldest of the older people.
We lacked data on the familial history of asthma and atopy, which is an important risk factor for asthma and a potential modifier of the effects of air pollution. Mixed evidence exists on the latter, with two studies showing enhanced11 14 and two studies showing attenuated12 13 effects of exposure to NO2 in people with atopy or allergy.
The dispersion models used to assess NO2 levels have been validated32–34 and applied.28 29 35 The correlations between modelled and measured NO2 concentrations at 204 locations in Copenhagen (1994–1995),32 and in a busy street canyon in Copenhagen (1995–2006),33 were high (r=0.90 and 0.67, respectively). Thus, the model predicted both geographical and temporal variation well. We do not have data for validation of the model in the early period (before 1994), but the weaker associations observed with the 15-year NO2 mean (since 1991) than with the 35-year NO2 mean (since 1971) with asthma (online supplementary table W2) and COPD28 suggest the validity of the predicted NO2 levels from the 1970s and 1980s. Although the modelled concentrations are only surrogates of real exposure and are inevitably associated with some exposure misclassification, this is not likely to be different with respect to asthma hospitalisation. Further limitations of the exposure assessment method are that we assessed only outdoor concentrations and had no information on work address, commuting habits or personal activities.
Our study offers new evidence that long-term exposure to traffic-related air pollution in adult life is a risk factor for asthma hospitalisation among older people. The effect was most notable for those with the greatest propensity for admission, namely people with prior hospitalisations for asthma or COPD. Our study adds to the existing evidence that reductions in traffic emissions might also mitigate the asthma burden in older people.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
See Editorial, p 2
Funding The study was funded by the Danish Research Council and Danish Cancer Society.
Competing interests None.
Patient consent Obtained.
Ethics approval Relevant Danish ethical committees and data protection agencies approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.