Article Text

Abstract
Background Obstructive sleep apnoea (OSA) is commonly associated with obesity and can be improved by weight loss. Changes in upper airway size related to regional fat loss may mediate the improvement in OSA. This study aimed to assess changes in upper airway size and regional facial and abdominal fat with weight loss and their association with OSA improvement.
Methods Middle-aged obese men with moderate-to-severe OSA underwent a 24-week sibutramine-assisted weight loss trial. Polysomnography and CT of the head and neck were performed at baseline and 24 weeks. The upper airway lumen and facial and parapharyngeal fat were measured with image analysis software.
Results Post-intervention there was a significant reduction in weight (−7.8±4.2 kg, p<0.001) and apnoea-hypopnoea index (AHI) (−15.9±20.5 events/h, p<0.001). Velopharyngeal airway volume significantly increased from baseline (5.3±0.4 to 6.3±0.3 cm3, p<0.01) and facial and paraphayngeal fat volume significantly reduced. A reduction in upper airway length was associated with improvement in AHI (r=0.385, p=0.005). The variance in AHI improvement was best explained by changes in upper airway length and visceral abdominal fat (R2=0.31, p=0.004).
Conclusions Weight loss increases velopharyngeal airway volume, but changes in upper airway length appear to have a greater influence on the reduction in apnoea frequency. Inter-individual variability in the effects of weight loss on OSA severity cannot be explained in terms of changes in upper airway structure and local fat deposition alone.
- CT
- obesity
- obstructive sleep apnoea
- upper airway
- weight loss
- sleep apnoea
Statistics from Altmetric.com
Key messages
What is the key question?
Does improvement in OSA with weight loss reflect an increased upper airway size related to regional fat loss?
What is the bottom line?
Velopharyngeal volume increased slightly in obese men with OSA after a 6-month weight loss programme; however, change in airway length and visceral abdominal fat were the only measured variables to relate to OSA improvement.
Why read on?
This is the largest published study to date to explore the relationship between weight loss and improvement in OSA in terms of changes in upper airway structure and regional fat deposition.
Introduction
Obesity is the most common known risk factor for obstructive sleep apnoea (OSA) and is identifiable in at least 50% of adults with the disorder.1 Obesity is unique among other major risk factors (eg, age, male gender, postmenopausal status, craniofacial morphology) in that it is reversible and therefore represents a target for treatment. Indeed, weight loss—through lifestyle, surgical or pharmacological manipulations—improves OSA.2–4
The exact mechanisms by which obesity contributes to upper airway collapse during sleep are not completely understood. Increased local fat deposition presumably compromises airway space, while abdominal obesity reduces lung volume and therefore caudal traction on the pharynx.5 Although weight loss reduces OSA severity, it does not necessarily resolve and there is substantial individual variability in the impact of weight loss on OSA.3 4 It is likely that other factors, rather than total weight reduction, may be more closely linked to the outcome of weight loss. An anatomically smaller pharyngeal airway has been identified in patients with OSA6 and may result from enlargement of surrounding soft tissues, reduced craniofacial skeleton or a combination of both.7 Other OSA treatments (eg, positive pressure therapy and oral appliance therapy) increase upper airway volume.8 9 Weight loss in non-apnoeic women has been reported to increase upper airway size6; however, the effect of weight loss on upper airway structure in OSA has received little attention to date. Two previous studies have reported no changes in pharyngeal cross-sectional area (CSA) after weight loss; however, these studies were small in sample size.10 11
Regional fat may play an important role in the improvement in OSA subsequent to weight loss. Visceral abdominal fat is reported to be most closely associated with OSA,12 and buccal fat (chubby cheeks) has been shown to correlate with visceral fat and may be equally metabolically active.13 14 We have previously shown that surface face width is greater in patients with OSA than in non-OSA controls, and that this measurement relates strongly to measures of obesity (eg, neck and waist circumference).15 Furthermore, this surface facial metric is more important than other known anthropometric and craniofacial risk factors in predicting OSA.16
The aims of this study were to assess the effects of weight loss on the upper airway and surrounding regional facial fat in obese men with OSA and to assess the relationship between these changes and changes in general obesity and OSA severity. We hypothesised that improved sleep apnoea after weight loss would be associated with an increase in airway dimensions related to facial fat loss, and also that facial fat loss would be closely related to changes in visceral abdominal volume.
Methods
Subjects
The study subjects were a subset of those in a 24-week sibutramine-assisted weight loss study4 17 who additionally underwent upper airway and abdominal imaging. Inclusion criteria were men with OSA aged 30–70 years, body mass index ≥30 kg/m2, apnoea-hypopnoea index (AHI) ≥15 events/h and an Epworth Sleepiness Scale score >10 (see online supplement).
Weight loss and polysomnography
Subjects were treated with sibutramine (serotonin and norepinephrine reuptake inhibitor, 10 or 15 mg daily) and followed a 2500 kJ daily deficit diet with exercise advice for 24 weeks.4 Anthropometric data (height, weight, neck and waist circumference) were collected and standard polysomnography (Compumedics, Melbourne, Australia) was performed at baseline and 24 weeks.4 17
Computed tomography
Patients underwent a low-dose CT scan of the upper airway and abdomen using a 16-slice scanner (GE Medical Systems, Milwaukee, USA) (see online supplement for additional details).
CT image analysis
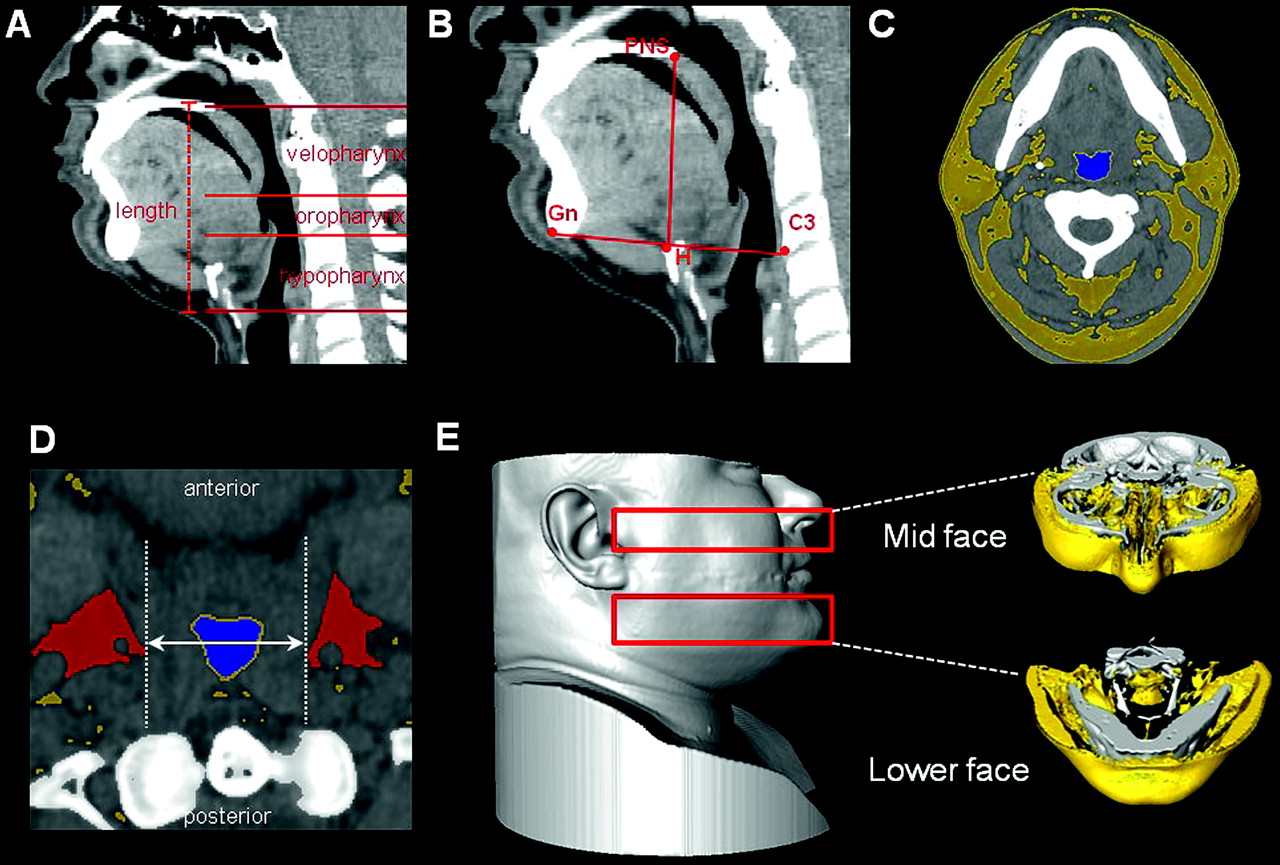
CT images for upper airway and facial fat analysis were processed using image analysis software (Amira 4.1; Visage Imaging Inc, Carlsbad, California, USA). CT images were automatically segmented based on Hounsfield unit (HU) values18 (figure 1C; see online supplement for additional details).
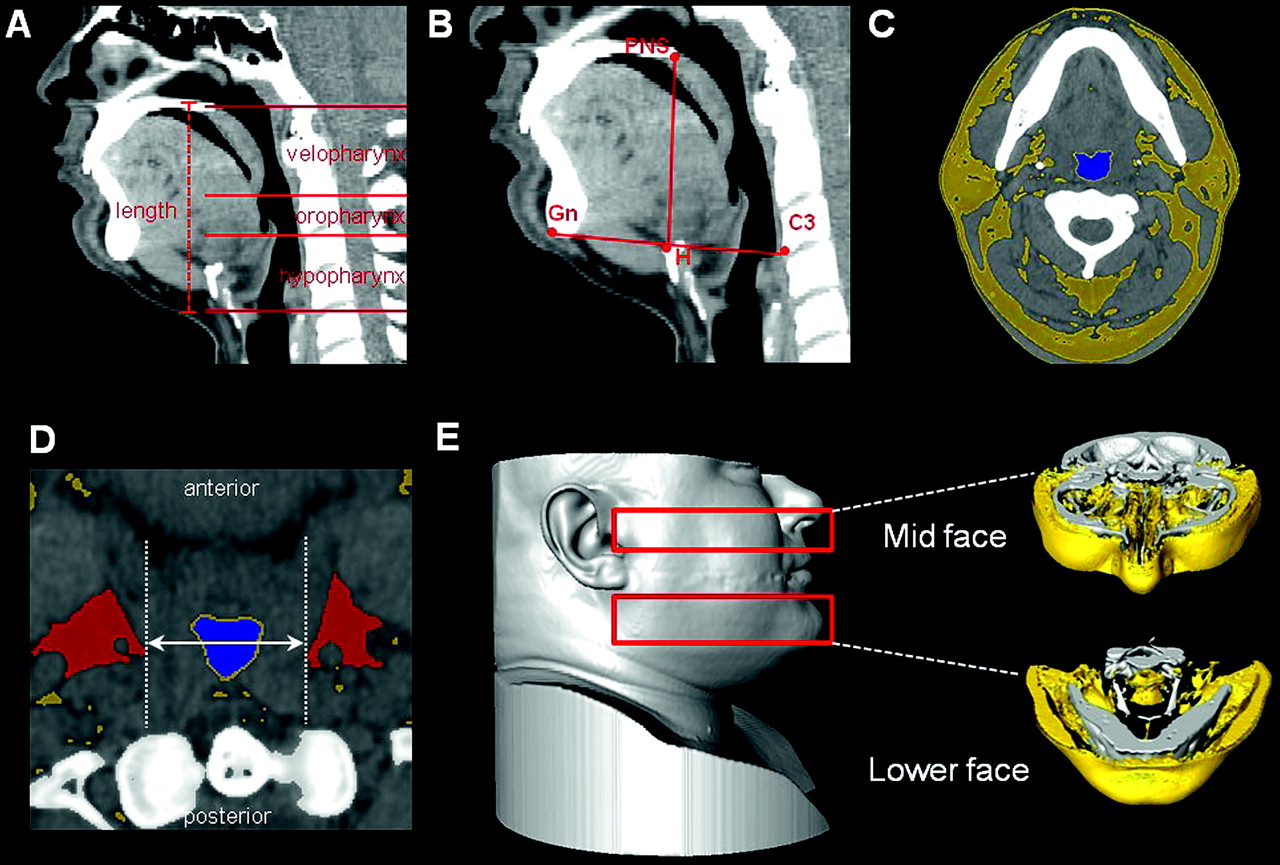
CT image analysis. (A) Mid-sagittal representation of the velopharyngeal, oropharyngeal and hypopharyngeal upper airway regions. Airway length was calculated as the sum of the thickness of the total number of image slices in the upper airway. (B) Hyoid bone position was determined on the mid-sagittal slice by the measurement of three linear distances between the hyoid (H) and C3 (C3 vertabrae), H and posterior nasal spine (PNS), and H and gnathion (Gn). (C) Representative axial CT slice illustrating segmentation of fat (yellow), upper airway lumen (blue) and bone (white) based on the Hounsfield scale where individual voxels are assigned to a tissue category based on their CT value. (D) The parapharyngeal fat pads were segmented separately (red). A measure of fat pad distance was made on axial slices by the length of a horizontal line spanning the distance between two vertical lines (anteroposterior direction) drawn along the medial borders of the fat pads. (E) Surface reconstruction of CT scan of the head depicting the mid and lower facial regions analysed (red rectangles). Corresponding three-dimensional reconstructions of internal fat volume (yellow) and bone (white) in the analysed regions (frontal view).
Upper airway regions were defined as velopharynx (hard palate to uvula tip), oropharynx (uvula tip to epiglottis base) and hypopharynx (epiglottis tip to vocal fold) (figure 1A). Upper airway length was calculated as the sum of the thickness of airway axial slices (figure 1A). Anteroposterior (A-P) and lateral (L) diameters were obtained for the velopharynx and oropharynx on the axial slice at the midpoint of the region.
Fat volume was measured in two defined regions of the face: mid-face and lower face. Facial regions and fat volumes measured are depicted in figure 1E. Bone volume in these regions was also recorded for methodology validation. The parapharyngeal fat pads were segmented separately for volume calculation. The distance between the fat pads was measured on the axial slice that intersected in the middle of the fat pads as shown in figure 1D.19
Hyoid position was measured on the mid-sagittal slice by three linear distances between the anterosuperior point of the hyoid (H) and three other points: posterior nasal spine (PNS), gnathion (Gn) and the anteroinferior point of the C3 vertebrae (C3) (figure 1B).
Abdominal subcutaneous and visceral adipose tissue (SCAT and VAT) volume analysis has been previously described.17 Additional details of imaging and analyses are given in the online supplement.
Statistical analysis
Statistical analyses were performed using statistical software package SPSS Version 17.0 for Windows (SPSS Inc). AHI, anthropometric and CT-measured variables (upper airway and fat) were compared between baseline and 24 weeks using paired t tests or Wilcoxon signed-rank tests, depending on data distribution. Correlation (Pearson r or Spearman ρ depending on the distribution of the data) was used to explore associations between continuous variables in all patients. Correlation analysis was used to assess relationships between (1) changes in OSA and upper airway and fat; (2) changes in anthropometric measures and fat volumes; (3) changes in facial and abdominal fat; and (4) changes in facial fat and upper airway dimensions. To account for multiple comparisons, an adjusted p value of <0.01 was considered statistically significant for the correlation analyses. Multivariate forward linear regression was used to investigate the relationship between improved sleep apnoea (%∆ AHI, dependent variable) and changes in fat and airway and anthropometric variables (independent variables). Variables selected for consideration in the model were those that in correlation analysis had p values <0.1. Change in supine sleep time was also considered as an independent variable to ensure that differences in body position between sleep studies did not contribute to changes in AHI. Multivariate linear regression was also used to assess whether baseline CT-measured variables could predict the amount of improvement in AHI. All independent variables in the regression analysis were examined for colinearity and analysed in separate models if necessary. The models were checked to ensure the assumptions of no multicolinearity, linearity and homoscedasticity were met. Statistical significance was accepted at p<0.05.
Results
Subject characteristics
The study subjects were Caucasian men aged 46.6±9.8 years who were moderately obese (34.1±2.6 kg/m2) with moderate-to-severe OSA (AHI range 16.9–109.9 events/h). The subjects had moderate weight loss (7.8±4.2 kg) and improvement in OSA (31% reduction in AHI), although with large individual variation (see figure S1 in online data supplement).
Anthropometric, fat and upper airway variables before and after weight loss
Paired CT data (baseline and 24 weeks) were analysed for 54 subjects. Comparative anthropometric, upper airway, regional fat and hyoid position data between the two time points are presented in table 1.
Paired comparisons of anthropometric and CT-measured variables at baseline and after a 24-week weight loss programme
Upper airway length and oropharyngeal or hypopharyngeal measurements did not change. Velopharyngeal volume increased significantly at 24 weeks (5.3±2.6 cm3 vs 6.3±2.4 cm3; figure 2) along with minimum CSA, mean CSA and the lateral diameter.

Upper airway volumes at baseline and after a 24-week weight loss programme. The velopharyngeal volume increased compared with baseline (5.3±2.6 cm3 vs 6.3±2.4 cm3). There was no change in oropharynx or hypopharynx volume (N=51). *p<0.01.
Facial (mid, lower face, fat pad) and abdominal (subcutaneous and visceral) fat volumes decreased following weight loss. Bone volume did not change between analysed scans in either face regions (data not shown), validating this methodology to measure changes in facial fat volume reliably. The parapharyngeal fat pad volume decreased significantly and fat pad distance increased slightly but without reaching statistical significance. Surface reconstructions from CT images of the face and upper airway before and after weight loss are shown for an individual patient (figure 3).

{kind=link}
{kind=link}
{kind=link}
Surface reconstructions from CT scans of a single patient before and after weight loss showing (A) head and neck region and (B) the upper airway. The patient showed a 5.1 cm3 increase in upper airway volume after 19 kg weight loss (approximately 18% of body weight) associated with an improvement in apnoea-hypopnoea index (AHI) from 55.9 events/h to 15.1 events/h.
Hyoid to PNS and hyoid to C3 distances decreased, suggesting there was posterior and superior movement of the hyoid bone with weight loss.
Relationships between changes in anthropometric and CT-measured variables (upper airway and facial and abdominal fat) and OSA improvement
Anthropometric changes showed some relationship with improvement in AHI (table 2), but these correlations did not reach statistical significance. Changes in facial and parapharyngeal fat did not correlate with AHI. Abdominal fat changes showed some relationship with changes in AHI, but only changes in visceral abdominal fat significantly correlated with improvement in AHI.
Correlation coefficients for percentage change (%∆) in AHI with %∆ in anthropometric and CT-measured variables
Upper airway structural changes did not show any relationship with AHI improvement. Although there was no mean change in upper airway length between baseline and 24 weeks, there was a positive correlation between percentage change in AHI and difference in upper airway length. Multiple linear regression analysis (table 3) showed that the percentage improvement in AHI was best predicted by a reduction in airway length and visceral abdominal fat. This model explained approximately 30% of the variance in AHI change. There was colinearity between anthropometric and abdominal fat measures. To account for this, these predictors were considered in separate models. Although weight, waist circumference and subcutaneous abdominal fat were also found to be predictive in combination with change in airway length, these models did not explain as much of the variance in AHI change as the model containing visceral abdominal fat (see table S2 in online data supplement).
Multiple regression analyses for percentage change (%∆) in AHI (N=48)
Relationships between changes in anthropometric and CT-measured facial and abdominal fat
Changes in anthropometric measures (weight, neck and waist circumference) were strongly related to changes in facial fat (mid and lower face) and abdominal fat (subcutaneous and visceral) volumes measured by CT (table 4). There was no relationship between changes in fat pad volume and anthropometric measures.
Correlation coefficients for percentage changes (%∆) in anthropometric and CT-measured fat variables
Relationships between facial and abdominal fat loss
Changes in abdominal fat volumes were strongly related to changes in facial fat volumes but not parapharyngeal fat pad volume (table 5). Generally, facial (mid and lower face) fat loss was more closely related to visceral than to subcutaneous abdominal fat loss. Visceral abdominal fat loss appeared to be more closely related to mid-face fat loss than lower face fat loss.
Correlation coefficients for percentage changes (%∆) in facial and abdominal fat volumes measured on CT scan
Relationships between fat loss and upper airway changes
Facial or parapharyngeal fat loss was not associated with changes in the upper airway. No anthropometric measures or abdominal fat volumes correlated with changes in upper airway variables.
Baseline measurements and improvement in OSA
Baseline CT variables were checked for relationships with improvement in AHI to assess any predictive value for weight loss outcome. No baseline measures correlated with or were predictive of the amount of improvement seen in AHI after weight loss.
Discussion
Weight loss decreases upper airway collapsibility during sleep, and this improved upper airway function can be attributed to reduced mechanical loads resulting from adiposity and/or subsequent improvements in neuromuscular control. However, the effect of weight loss on upper airway structure in OSA has received little attention in the literature. To our knowledge, this is the largest study to investigate the effects of weight loss on the upper airway and regional facial fat in obese men with OSA using volumetric analyses. Weight loss was associated with an increase in velopharyngeal airway size and reductions in facial and parapharyngeal fat volume.
Upper airway
Increased extraluminal tissue pressure and reduced airway space resulting from fat deposition around the pharynx can facilitate upper airway collapse.5 We have shown enlargement of the velopharyngeal airway space in obese men with apnoea after weight loss. The velopharyngeal walls are directly bordered by the lateral parapharyngeal fat pads. Reduced volume of these adipose tissue structures with fat loss could alter traction on surrounding soft tissues and influence velopharyngeal size, particularly in the lateral dimension (as found in this study). The only previous investigations of the effects of weight loss on upper airway structure in OSA have reported no changes in pharyngeal areas following weight loss.10 11 However, this may reflect the smaller sample sizes (n=12), analysis being limited to CSA and gender differences, with one sample predominantly female.10 Although we did not investigate other upper airway soft tissue structures, a previous weight loss imaging study in women without OSA reported no changes in tongue and soft palate volumes,19 which may account for the absence of changes in the lower pharyngeal regions.
Decreased airway length was associated with a greater improvement in the severity of OSA. Length change was found to be more influential than total weight or visceral abdominal fat loss in explaining AHI improvement. A longer upper airway has been associated with OSA20 and may be an important factor in the propensity to collapse. Indeed, a longer airway in men appears to be the primary characteristic—anatomical or functional—to explain the male predisposition to OSA.21 Furthermore, pharyngeal length increases in the supine position in men with OSA but not controls.22 Our finding may suggest that a decrease in supine upper airway length after weight loss contributes to reduced collapsibility. However, the mechanisms by which upper airway length is reduced are unclear. Increased lung volume decreases pharyngeal collapsibility23 and increases pharyngeal CSA,24 25 presumably via increased caudal traction on upper airway structures from mediastinal, rib cage and cervical strap muscle connections.26 Such increases in pharyngeal CSA could be associated with shortening of the total upper airway length, but the effects of lung volume changes on upper airway structure requires further investigation. Similarly, changes in adipose tissue around the pharynx could increase lateral traction, shortening the upper airway.
Hyoid position
Hyoid position shifted superiorly and posteriorly post-intervention. An inferiorly positioned hyoid bone is a cephalometric finding commonly associated with OSA.27 It is unclear whether an inferiorly positioned hyoid is a cause or effect of OSA, but the decreased vertical distance of the hyoid position observed in this study may result from a lessening of downward pressure due to a reduction in excess pharyngeal tissues.
Regional fat
Fat loss in both facial and abdominal regions correlated highly with anthropometric changes of obesity. In this study, change in visceral adipose tissue volume had the strongest relationship with improvement in OSA of all the obesity measures. Changes in facial fat correlated with abdominal fat loss, with this relationship being strongest between visceral adipose tissue and mid-face fat volume. Indeed, reduction in visceral adipose tissue was more closely associated with the amount of mid-face fat loss than changes in the anthropometric measure of waist circumference, and this supports the concept that facial fat may be an important risk factor for OSA. Interestingly, we found that at baseline (before weight loss) the only obesity measures to reflect the amount of visceral abdominal fat were waist circumference and mid-face fat volume, with both correlations being equally strong (see online supplement). This relationship with visceral fat was also preserved for the simplified measure of mid-face width. Our previous work using craniofacial photography identified this surface facial measure as highly predictive of OSA,16 and the current study suggests that this simple craniofacial metric may provide an insight into obesity-related risk factors for OSA in regions beyond the face.
Parapharyngeal fat pad size has previously been shown not to relate to the severity of OSA28 29 and was not related to improvement in AHI in the current study. However, our assessments of parapharyngeal and facial fat did not take craniofacial size into consideration. Upper airway collapsibility relates not only to the amount of surrounding tissue but also to the size of the craniofacial skeleton enclosing it, a concept termed ‘anatomical balance’.7 30 Therefore, changes in total upper airway volume in relation to overall anatomy and not just reduced adipose tissue size may be important. In this study, soft tissue within the craniofacial enclosure could not be assessed due to artefact in the oral region obscuring the tongue. However, a surrogate correction for craniofacial bony enclosure using the bony facial width did not relate our fat volumes more closely to OSA (results not shown). Craniofacial size may be important as a denominator in assessing regional fat loss effects on OSA but requires verification in future studies.
Obesity may also influence sleep apnoea through its inflammatory and metabolic consequences. Centrally-acting proinflammatory cytokines and adipokines such as leptin may alter respiratory control and modulate upper airway function.5 12 Indeed, leptin was reduced after the 6-month weight loss programme in patients in this sibutramine-assisted weight loss trial.17 Alterations in such factors by changes in adiposity may account for improvement in upper airway neuromuscular control beyond the anatomical changes associated with reductions in mechanical loads on the pharynx and torso. These effects may not directly correlate with measurable fat volumes and may help to account for interindividual variability in changes in AHI with weight loss.
Study limitations
Several aspects of this study may limit the generalisability of these findings. First, although subjects lost weight, the amount on average was relatively modest (about 7% of body weight). The corresponding improvement in OSA (about 30%) appears reasonable for this weight loss,31 but greater fat loss may be needed to detect and investigate effects on upper airway structure. Bariatric surgery could therefore be a better paradigm to study the effects of weight on upper airway structure due to the more substantial weight loss achieved.
Sibutramine has a greater effect on reducing central adiposity,32 which is more common in men and has a close association with OSA.5 Although this is of particular relevance to the population studied, extrapolating these findings to other weight loss methods and women may require caution. Indeed, the influence of regional obesity on the severity of OSA appears to differ between genders, with neck fat in women and abdominal fat in men being of more significance.33 This may have implications for weight loss effects on upper airway size, which may be more prominent in women.
Sibutramine, by its action through the central nervous system, may have had some effect on the severity of OSA independent of weight loss, which would affect our assessment of upper airway structure in relation to OSA improvement. However sibutramine, without weight loss, is reported not to affect sleep architecture or OSA severity acutely.34
The original experimental design did not include a control group. Comparing 6-month interval CT scans with weight loss may incur variability. Although imaging posture was standardised, fat loss may have led to variations in head or neck posture which may affect airway size and shape. Dental artefact in the oral region also precluded analysis of the entire fat pad structure in some patients. The fat content of specific upper airway soft tissues cannot be as well defined with CT scanning as with MRI.6 However, the primary aim of the original study was to investigate the effects of sibutramine-assisted weight loss on OSA, and CT scanning was considered most practical to address the secondary aims of investigating the effects on upper airway structure. Indeed, shorter CT scanning times may be preferable for investigation of the upper airway lumen as the image reflects a single breath hold and is not averaged over multiple breath cycles. Also, analysis of large fat volumes—according to the aims of this study—was able to be performed rapidly and CT scanning has been shown to have less inter- and intra-observer variability than MRI.35 Also, this study only looked at anatomical changes in the upper airway whereas techniques such as computational fluid dynamics could be used to assess changes in upper airway resistance, which may further explain the improvement in OSA with weight loss.36
Conclusions
This is the largest study to investigate the effects of weight loss on upper airway structure in OSA using volumetric analysis. Improved OSA in obese men after a 6-month weight loss programme was associated with a small increase in velopharyngeal airway volume mediated by an increase in lateral diameter. Although this volume increase may have contributed to the reduced upper airway collapsibility, decreased upper airway length was found to be most closely associated with AHI reduction. Regional facial fat volumes closely reflect anthropometric variables of body habitus. However, inter-individual variability in the effects of weight loss on OSA severity cannot be explained in terms of changes in upper airway structure and local fat deposition alone. Future phenotyping studies incorporating craniofacial structure, regional body fat distribution, upper airway structure and function, and lung volume are needed to ascertain the relationship between weight loss and improvement in OSA.
Acknowledgments
The authors thank Dr Dev Banerjee and Dr Mike Trennell for their contributions to the study.
References
Supplementary materials
Web Only Data thx.2010.151613
Files in this Data Supplement:
{kind=link}
Footnotes
Funding This study was investigator-driven but was partly funded by Abbott Laboratories, Sydney, Australia (financial support and provision of Sibutramine medication for the participants) and the National Health and Medical Research Council Grant Number 301936.
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics review committee (Royal Prince Alfred Hospital zone) of the Central Sydney Area Health Service, protocol no. X0203316.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves