Article Text

Statistics from Altmetric.com
A 76-year-old lady was referred to the respiratory clinic with a 6-month history of a discharging left chest wall sinus. She also had a 6-month history of dry cough, left chest wall pain and breathlessness. There was no history of fever, haemoptysis, weight loss or night sweats. She was a lifelong non-smoker and there was no history of asbestos exposure.
Investigations showed elevated white blood cell count of 14.5×109/l (neutrophil count 11×109/l) and C reactive protein 87 mg/L; renal and liver function tests were normal. Sputum cultures were negative.
She had a laparoscopic Nissen fundoplication 12 years earlier, complicated by perforation of the oesophagus. Subsequently, 6 years later, she developed dyspnoea; a chest x-ray at this time revealed a left-sided pleural-based abnormality. A thoracoscopic biopsy suggested benign pleural thickening/fibrosis. After thoracoscopy, she developed a discharging sinus around the access port site, which was excised.
The patient then relocated to the region and presented with a persistent discharge from the original chest wall sinus. Oral penicillin was commenced, although with only partial response and incomplete resolution of the discharge. Chest x-ray revealed a mass lesion in the left hemithorax, which was confirmed by a CT scan (figures 1 and 2).
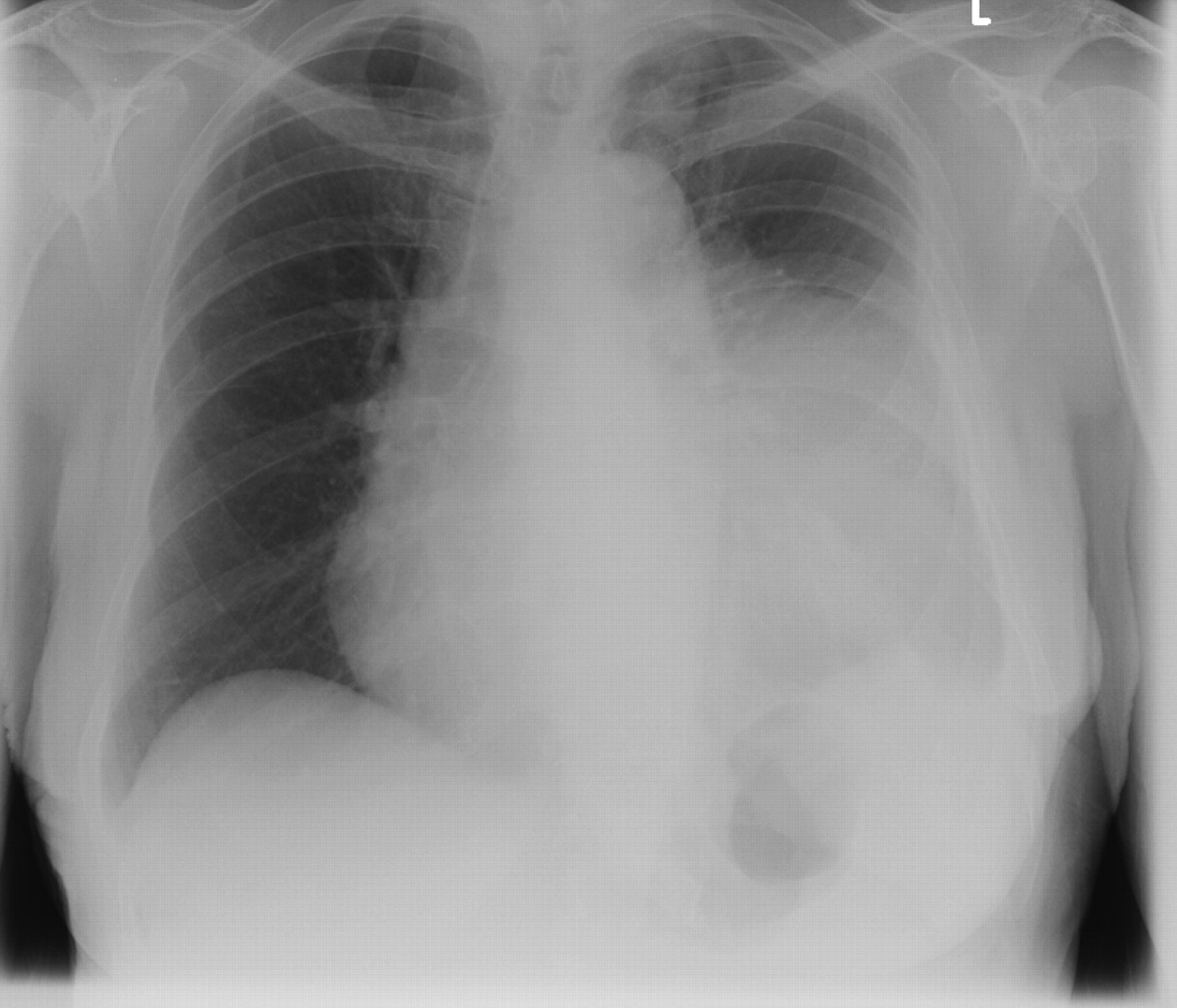
Chest x-ray, March 2010: extensive opacification within the left middle and lower zone.

CT scan of chest, March 2010: large mass within the left pleural space, which appears to invade the anterior chest wall.
Question
What is the diagnosis?
See page 738 for the answer
Answer
From the question on the page 733
Our patient underwent thoracotomy and excision of the mass (figures 3–5).
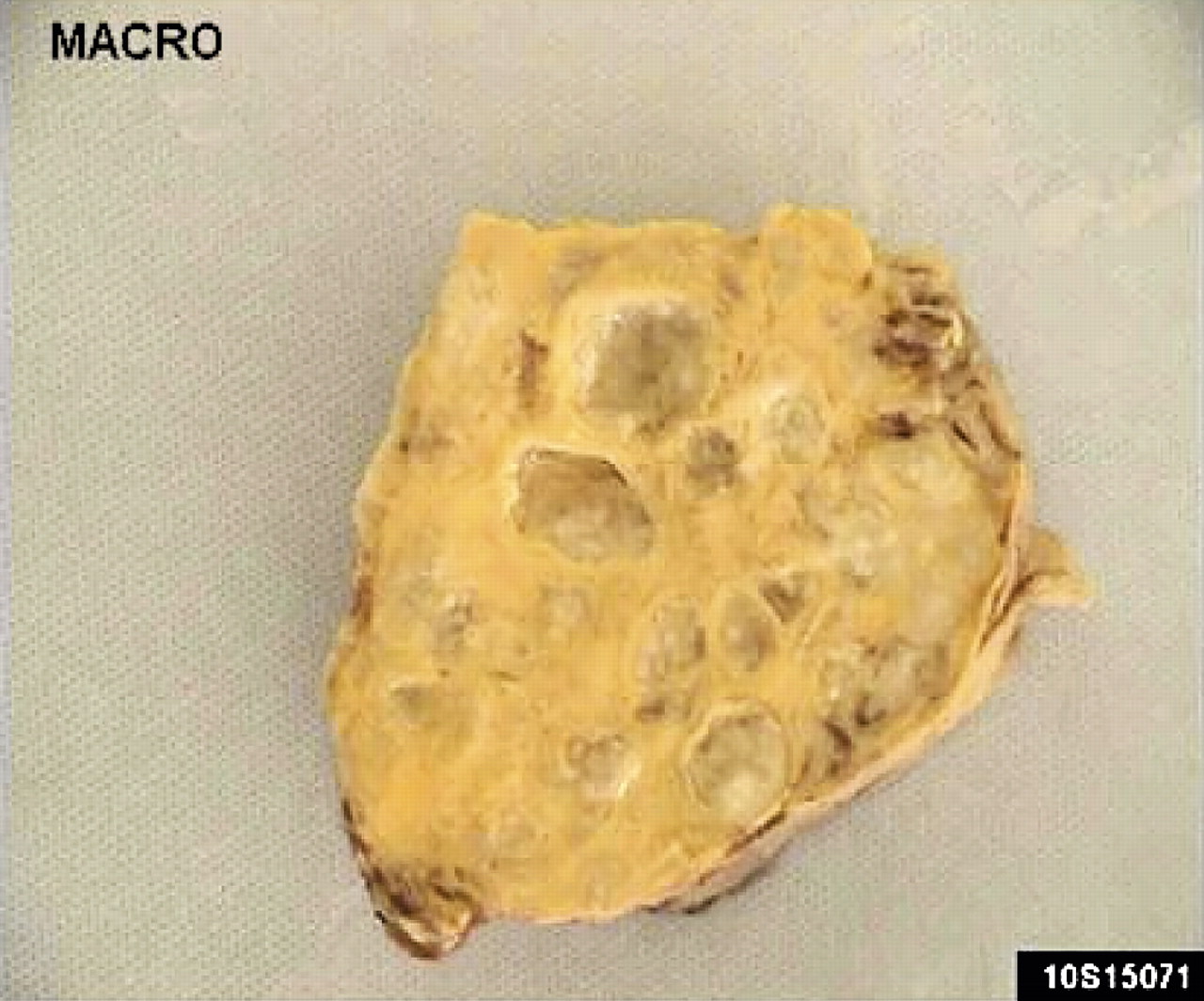
The pleural mass weighing 267 g was received in several fragments, the largest up to 8 cm in size. The cut surface was yellow with numerous locules of pus.

H&E stain showing a sulphur granule in a patient with actinomycosis. Many of the filamentous bacteria showed eosinophilic glassy deposits—a typical Splendore-Hoeppli phenomenon.

Actinomycosis colonies under Grocott's methenamine silver stain.
The cut surface was yellow with numerous locules of pus. Microscopy confirmed widespread abscess formation within a cellular fibrous stroma admixed with macrophages and cholesterol clefts. Within each abscess was a colony of actinomyces organisms surrounded by neutrophils. Many of the filamentous bacteria showed eosinophilic glassy deposits—a typical Splendore-Hoeppli phenomenon.
Although microscopy and culture of the wound sinus were negative, culture of the excised abscess grew actinomyces as well.
Postoperatively the patient was given high-dose amoxicillin, initially intravenously 2 g four times a day for 2 weeks followed by 6 months of an oral 1 gm dose four times a day (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
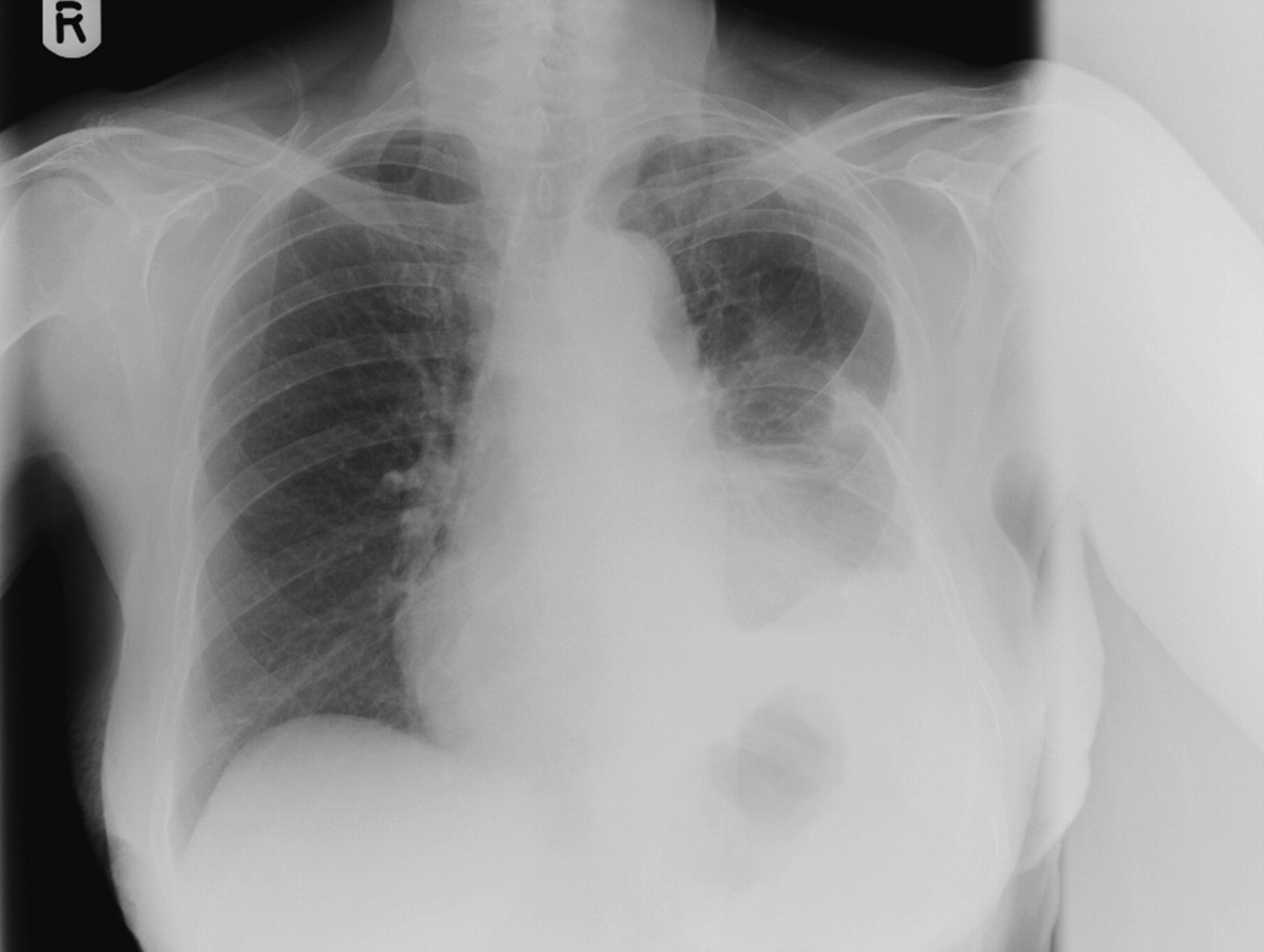
Follow-up chest x-ray, September 2010: loss of volume of the left lung and partial rib resection due to the previous thoracotomy. There is blunting of the left costophrenic angle, elevation of the left hemidiaphragm and increased density at the left base due to the previous thoracotomy. The right lung is clear.
Our patient had a good clinical response and the elevated inflammatory markers returned to normal.
Discussion
Common causes of large pleural-based masses include benign or malignant pleural tumours, as well as metastatic pleural deposits among other diagnostic possibilities. Thoracic actinomycosis, although less common, can occur but can easily elude diagnosis.
Actinomycosis is an infection caused by the actinomyces organism, a gram-positive anaerobic bacterium. The most common species is Actinomyces israelii. Pulmonary actinomycosis accounts for the 15% of the cases.1
Although sulphur granules are pathognomonic in the diagnosis of actinomycosis, similar findings are also noted in infections caused by Nocardia brasiliensis, Streptomyces madurae and Staphylococcus aureus causing botryomycosis. Sulphur granules consist of colonies of micro-organisms surrounded by polymorphonuclear neutrophils.1
There may be chronic pneumonia associated with pleuritis, abscess and fibrosis. Empyema allows extension to the chest wall and may lead to a fistula. Radiographic findings include peripheral non-segmental basilar infiltrates, mass-like consolidation, cavitation and pleural effusion or pleural thickening.2
Thoracic actinomycosis is usually the result of aspiration of infected material from the oropharynx. Normal gravitational and anatomical factors result in a predominance of lower-lobe pulmonary disease.3 Given the usual aetiology of thoracic actinomycosis, the likely factor in our patient's history was oesophageal perforation many years earlier.
Penicillin is the treatment of choice, in high dose and for a prolonged duration, most usually suggested for several months, but infections could also be polybacterial needing other antibiotics, especially if the recovery is slow. Complications include chronic and progressive sepsis, which may prove fatal. Surgery is reserved as a treatment option where diagnosis is uncertain (suspected neoplasm) or where there is no initial response to antibiotics.4
To conclude, there should be a high level of suspicion for the presence of actinomyces in cases with draining chest wall sinuses or with spontaneous discharge of an empyema. Recognition of these symptoms might avoid the need for surgery as actinomyces is an extremely penicillin-susceptible organism.
Footnotes
AK and MD contributed equally to this work.
Correction notice This article has been corrected since it was published Online First. The order of authors and their affiliations were changed.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves