Article Text

Abstract
Introduction The peroxisome proliferator-activated receptor-γ agonists rosiglitazone and pioglitazone activate glucocorticoid receptors and have an immunomodulatory effect. The authors aimed to systematically determine the risk of pneumonia or lower respiratory tract infections associated with thiazolidinediones.
Methods Systematic searches of MEDLINE, EMBASE, regulatory documents and trial registries were carried out for randomised controlled trials of thiazolidinediones with no date restrictions through March 2010. The authors selected long-term (≥1 year) randomised controlled trials of thiazolidinediones versus a placebo, metformin or sulfonylurea control for prevention or treatment of type 2 diabetes that reported on pneumonia or lower respiratory tract infection adverse events or serious adverse events (hospitalisation, disability or death). Relative risks (RRs) were estimated using a fixed-effects meta-analysis, and statistical heterogeneity was assessed using the I2 statistic.
Results Thirteen trials (n=17 627, including 8163 patients receiving thiazolidinediones and 9464 patients receiving control therapy) with a duration of follow-up of 1–5.5 years were included after a detailed screening of 58 studies. Thiazolidinediones were associated with a statistically significantly increased risk for any pneumonia or lower respiratory tract infection (n=130/8163 vs 100/9464; RR 1.40; 95% CI 1.08 to 1.82; p=0.01; I2=0%) and serious pneumonia or lower respiratory tract infection (n=111/7391 vs 87/8692; RR 1.39; 95% CI 1.05 to 1.83; p=0.02; I2=0%).
Interpretation Long-term thiazolidinedione use is associated with a modestly increased risk of any pneumonia or lower respiratory tract infection and serious pneumonia or lower respiratory tract infection in patients with type 2 diabetes.
- thiazolidinediones
- type 2 diabetes
- trials
- serious adverse events
- pneumonia
- clinical epidemiology
- drug-induced lung disease
- drug reactions
- systemic disease and lungs
Statistics from Altmetric.com
- thiazolidinediones
- type 2 diabetes
- trials
- serious adverse events
- pneumonia
- clinical epidemiology
- drug-induced lung disease
- drug reactions
- systemic disease and lungs
Introduction
Thiazolidinediones (rosiglitazone and pioglitazone) are peroxisome proliferator-activated receptor (PPAR)-γ agonists. Rosiglitazone is a PPARγ agonist whereas pioglitazone has both α and γ effects. PPAR activation has anti-inflammatory and immunomodulatory effects in the lung.1 Thiazolidinediones act as partial agonists at the glucocorticoid receptor.2 Rosiglitazone significantly improved lung function compared with inhaled beclometasone in a recent randomised controlled trial (RCT) in people who smoke and have asthma.3 Pioglitazone is as effective as dexamethasone in reducing airway hyper-responsiveness and pulmonary inflammatory mediators in animal studies.4 There is considerable optimism about the potential of the thiazolidinediones to favourably affect the course of asthma and chronic obstructive pulmonary disease.
The long-term effects of thiazolidinediones, however, are unpredictable, resulting in unusual toxicities. There have been concerns about an increased risk of myocardial infarction associated with rosiglitazone.5–7 Thiazolidinediones are associated with an increased risk of congestive heart failure,6–8 fractures (in women),9 and possibly macular oedema.
It is possible that these immunomodulatory and glucocorticoid-like properties of the thiazolidinediones could potentially induce susceptibility to lung infections, similar to glucocorticoids in chronic obstructive pulmonary disease.10 A signal for an increased risk of pneumonia in patients with type 2 diabetes was reported in a long-term trial of pioglitazone.11 Another long-term trial of rosiglitazone reported a non-significant increase in pneumonia adverse events.6 However, the exact risk of rare, serious adverse events such as pneumonia cannot always be conclusively determined from a single trial because of inadequate statistical power. The authors aimed to systematically determine the risk of pneumonia or lower respiratory tract infection adverse events associated with thiazolidinedione therapy in long-term clinical trials of patients with type 2 diabetes.
Methods
Selection of trials with pneumonia or lower respiratory tract infection adverse event data
Our specific inclusion criteria were as follows: a study design consisting of parallel group RCTs of any thiazolidinedione (rosiglitazone or pioglitazone) with a treatment duration of at least 12 months; study participants with type 2 diabetes mellitus; control treatment which could be placebo, metformin or sulfonylurea, with the only difference between the treatment groups being thiazolidinedione exposure among participants; studies that reported data on ‘pneumonia’ or ‘lower respiratory tract infection’ adverse events or serious adverse events (including 0 events).
Active oral hypoglycaemic agents (metformin or sulfonylurea) were used as active comparators because metformin and sulfonylurea are not known to increase the risk of pneumonia. The recently approved incretin mimetics have been linked to an increase in the risk of infections.12 The analysis was restricted to RCTs of at least 12 months' duration to evaluate the risk of pneumonia associated with long-term use of thiazolidinediones.
Search strategy
The authors evaluated all the RCTs identified from the database searches (MEDLINE, EMBASE, Cochrane Controlled Trials Register) in their previous systematic reviews.7–9 The authors (YKL and SS) conducted an updated search of MEDLINE and EMBASE (Ovid SP from June 2008 to March 2010) for RCTs of rosiglitazone and pioglitazone. Trial reports were evaluated of all phase 3 and 4 published or unpublished trials of the GlaxoSmithKline clinical trials register, the Takeda clinical trials register and the Clinical Study Results Database for additional RCTs. Existing systematic reviews and the bibliographies of the studies that were included were checked. The search was limited to English-language articles, and included pre-approval and unpublished studies from regulatory documents and trial registries. The updated search strategy is outlined in online appendix S1.
Study selection
Trials were identified and subjected to inclusion and exclusion criteria. Two reviewers (SS and YKL) independently and in duplicate scanned all titles and abstracts that indicated the study was an RCT evaluating the use of thiazolidinediones among patients with type 2 diabetes. After obtaining full reports of potentially relevant trials, the same reviewers independently assessed eligibility from full-text articles.
Study characteristics
A prespecified protocol was used to record the location and duration of the RCT (in years), the inclusion and exclusion criteria, the dose and frequency of thiazolidinedione and control interventions, mean age and sex of participants, and mean glycated haemoglobin levels at baseline.
Risk of bias assessment
The Cochrane Toolkit was used for the assessment of bias in evaluating each trial for the reporting of sequence generation, allocation concealment, the use of blinding of participants and personnel, and information on loss to follow-up or withdrawal rates.13 In accordance with the Cochrane handbook of systematic reviews, the authors assessed the strength of adverse events data by noting how the investigators monitored and recorded adverse events.13
Outcome measures
The primary prespecified outcomes measures were any pneumonia or lower respiratory tract infection adverse event (irrespective of severity), and pneumonia or lower respiratory tract infection reported as serious adverse events. Serious adverse events are life-threatening, require hospitalisation, or lead to significant disability or death.
Data abstraction
Two reviewers (SS and YKL), independently and as a team, assessed the eligibility and quality of studies for reporting of adverse events. They separately extracted data (including 0 events) on the proportion of patients with any pneumonia or lower respiratory tract infection among tabulated listings of adverse events for each study. Published reports were reconciled with trials in the clinical trials register when possible to avoid potential duplication. If there were multiple reports available for a particular study, data on pneumonia were extracted from the latest version.
Two reviewers (SS and YKL) were independently involved in all stages of study selection, data extraction and quality assessment. Any discrepancies were resolved through discussion. The reviewers achieved consensus on inclusion of studies and data extraction.
Data synthesis
Review Manager (RevMan), version 5.024 (Nordic Cochrane Center, Copenhagen, Denmark) was used to conduct a meta-analysis of the pooled relative risks (RRs), with 95% CI, using the fixed-effects model for dichotomous outcomes. The fixed-effects Mantel–Haenszel model is the appropriate method for meta-analysis of rare events because the random effects model lacks statistical power.14 A continuity correction of 0.5 was used when there were zero events in one intervention arm. All reported p values are two sided, with significance set at p<0.05. Statistical heterogeneity was assessed using the I2 statistic.15 A substantial level of heterogeneity is indicated by I2 values of 50% or more.15
Prespecified sensitivity analyses were conducted to determine the influence of statistical models (use of Peto odds ratio which has been recommended for analysis of rare events, or the random effect which has less power)14 on effect size. A subgroup analysis was also conducted to evaluate for intraclass differences in the risk of pneumonia between rosiglitazone and pioglitazone. Publication bias was assessed by visual inspection for funnel plot asymmetry,13 and evaluation of effect sizes in published studies versus data obtained from unpublished studies. The fail-safe number using the Rosenberg method was estimated to assess the potential impact of missing data in the meta-analysis (ie, the number of additional negative trials that would be required to reverse a significant finding in the meta-analysis).16
The number needed to harm (and 95% CI) was estimated by applying the pooled RR from the meta-analysis to the average control event rate in different populations. The number needed to harm is the number of patients with type 2 diabetes who need to be treated with a thiazolidinedione, rather than with placebo or comparators, for one additional patient to have pneumonia or a lower respiratory tract infection.
Results
The selection of trials is shown in figure 1 (online). The authors identified 280 potentially relevant citations, and after a detailed review of 58 studies, selected 10 datasets involving 13 trials of 17 627 patients that reported on pneumonia or lower respiratory tract infections.6 11 17–32
Trial characteristics are shown in table 1. In the trials 8163 participants received thiazolidinediones and 9464 received control therapy. Nine RCTs evaluated thiazolidinediones against active controls,6 17–21 27–32 while four RCTs evaluated them against placebo.11 22–26 The RCTs ranged in duration from 1 year to 5.5 years6 and the sample size ranged from as low as 5726 to 5238.11 Thiazolidinedione-exposed participants had similar glycated haemoglobin at baseline to the control patients. Eight RCTs evaluated rosiglitazone.6 17–27 Five RCTs evaluated pioglitazone, including one large RCT (the Prospective Pioglitazone Clinical Trial in Macrovascular Events, PROactive)11 and another dataset,28 which reported a pooled analysis among older patients with diabetes from four pioglitazone trials.29–32
Characteristics of long-term randomised controlled trials of thiazolidinedione use included in the analysis of pneumonia and lower respiratory tract infection adverse events
Trial quality was generally satisfactory (online table S1). All the RCTs were double blind except for the Rosiglitazone Evaluated for Cardiovascular Outcomes and Regulation of Glycaemia in Diabetes (RECORD) trial, which was open label.6 Four trials had inadequate reporting of allocation concealment, sequence generation or loss to follow-up.21 30–32 Eight RCTs were judged to be at low risk of bias (adequate sequence generation, allocation concealment and double blinding, and clear reporting of loss to follow-up or withdrawal rates), whereas the remaining five RCTs were at unclear risk of bias.6 21 30–32
Because pneumonia and lower respiratory tract infection have not previously been linked to thiazolidinedione therapy, detection in these trials occurred via routine monitoring of adverse events or serious adverse events because it is not possible to prespecify diagnostic criteria for unexpected adverse events. Accordingly, none of the included RCTs had objective pneumonia definitions, or reported the proportion of patients that had radiographic confirmation of pneumonia. Thus the methods for diagnosing pneumonia and lower respiratory tract infection possibly varied between trials (clinical vs radiographical). Seven trials reported pneumonia or lower respiratory tract infection to be a serious adverse event,6 11 17–23 whereas six trials reported lower respiratory tract infection as an adverse event.26–32 Approximately 86% of pneumonia and lower respiratory tract infection events in our meta-analysis were classified as serious adverse events leading to hospitalisation, disability or death. Although six trials did not report on cause-specific mortality,6 11 28–32 available information on fatal adverse events from seven rosiglitazone trials17 reported no deaths due to pneumonia or lower respiratory tract infection associated with rosiglitazone. Thus it is possible that most of these serious adverse events caused by pneumonia or lower respiratory tract infection stemmed from hospitalisation.
Risk of pneumonia or lower respiratory tract infection
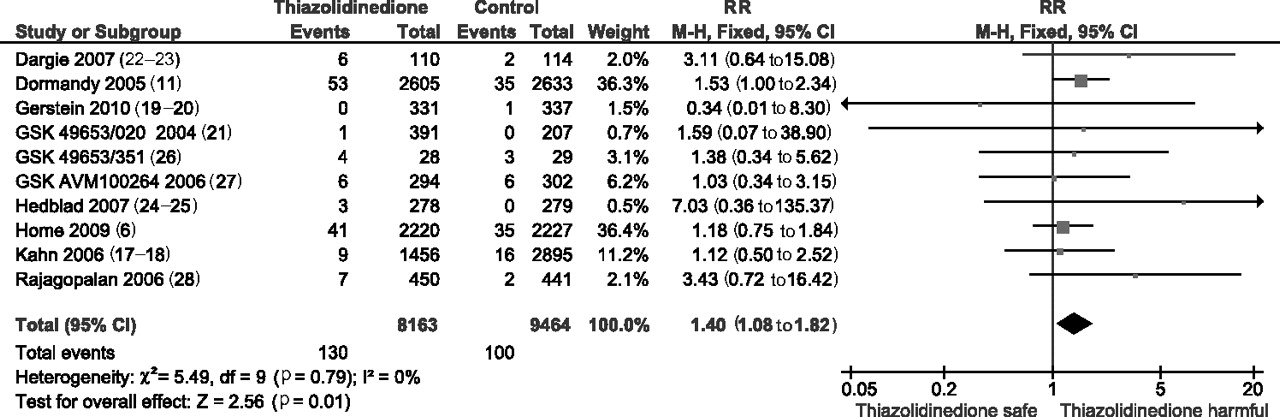
Thiazolidinediones were associated with a significantly increased risk of pneumonia or lower respiratory tract infection compared with controls in a meta-analysis of 13 RCTs involving 17 627 participants (n=130/8163 vs 100/9464; 1.59% vs 1.06%; RR 1.40; 95% CI 1.08 to 1.82; p=0.01); there was no statistical heterogeneity among the included trials (I2=0%) (figure 2).6 11 17–32

Fixed-effects meta-analysis of long-term randomised controlled trials of pneumonia or lower respiratory tract infection with thiazolidinediones versus controls.
Risk of pneumonia or lower respiratory tract infection as serious adverse events
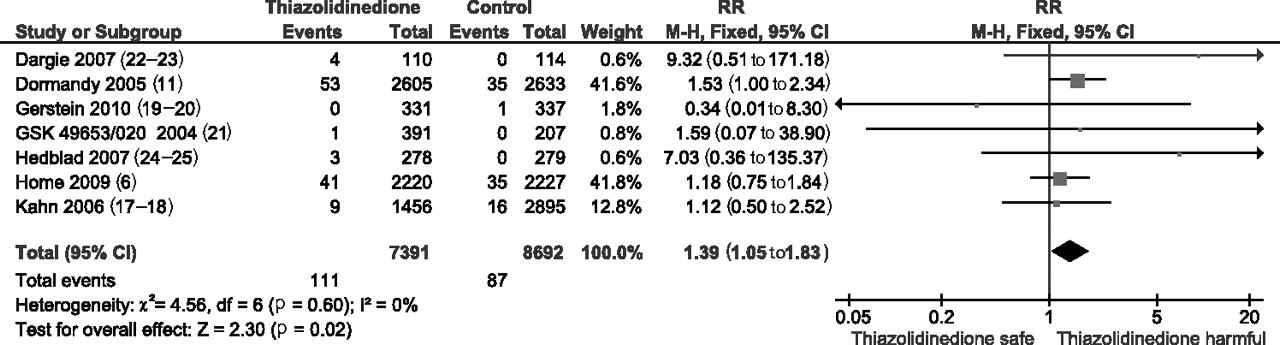
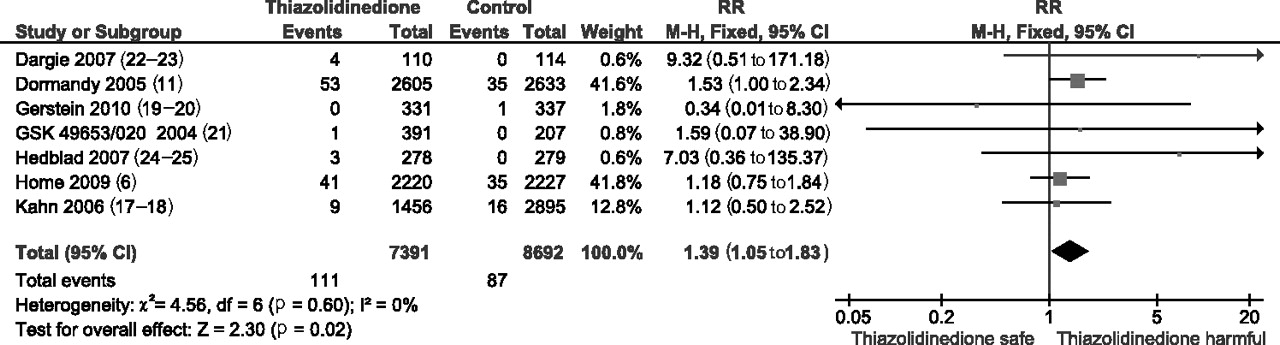
Thiazolidinediones were associated with a significantly increased risk of serious adverse events caused by pneumonia or lower respiratory tract infections compared with controls in a meta-analysis of seven trials involving 16,083 patients (RR 1.39; 95% CI 1.05 to 1.83; p=0.02); there was no statistical heterogeneity among the included trials (I2=0%) (figure 3).6 11 17–23
{kind=link}
{kind=link}
Fixed-effects meta-analysis of long-term randomised controlled trials of serious pneumonia or lower respiratory tract infection with thiazolidinediones versus controls.
Sensitivity analysis
The sensitivity analysis using the Peto odds ratio yielded estimates similar to those of the fixed-effects model for the risk of any pneumonia or lower respiratory tract infection associated with the thiazolidinediones (RR 1.42; 95% CI 1.09 to 1.84; p=0.009; I2=0%).6 11 17–32
The sensitivity analysis using a random-effects model yielded estimates similar to those of the fixed-effects model for the risk of any pneumonia or lower respiratory tract infection associated with the thiazolidinediones (RR 1.38; 95% CI 1.06 to 1.79; p=0.02; I2=0%).6 11 17–32
The direction of effect for both the thiazolidinediones showed a similar increased risk, with the RRs for pioglitazone achieving statistical significance (RR 1.63; 95% CI 1.09 to 2.46; p=0.02) in a meta-analysis of five trials involving 6129 patients.11 28–32 The RRs for rosiglitazone did not reach statistical significance (RR 1.26; 95% CI 0.90 to 1.76; p=0.23) in a meta-analysis of eight trials involving 11 498 patients, but a clinically significant excess risk could not be ruled out.6 17–27 The test for homogeneity of effects across the two thiazolidinediones pioglitazone and rosiglitazone did not demonstrate a statistically significant difference between the two agents (p=0.32). However, these subgroup analyses should be interpreted for the direction of effect, rather than the magnitude of statistical significance, because subgrouping or removal of specific studies can render the meta-analysis underpowered to detect differences.
Assessment of publication bias and missing data
Visual inspection of the funnel plot did not reveal any evidence of asymmetry (online figure S1). The RR for pneumonia from unpublished data was 1.38 (95% CI 0.82 to 2.30), which was similar to that of the published studies (RR 1.40; 95% CI 1.05 to 1.90). To reverse the significantly increased risk of pneumonia or lower respiratory tract infection shown in our meta-analysis, 11 negative studies with an average sample size of 1400 participants would be required.23
Estimated number needed to harm
Using estimates of the incidence of pneumonia of 4919/100 000 person-years from a population-based study (mean age 61 years, 51.7% male) in patients with type 2 diabetes in Ontario,33 the number needed to harm for pneumonia or lower respiratory tract infection associated with thiazolidinedione use was estimated to be 55 (95% CI 28 to 269). Treatment of 55 patients with thiazolidinediones for 3.7 years would result in one extra case of pneumonia or lower respiratory tract infection based on the event rate in population-based studies. Based on the average control event rate in the trials, the estimated number needed to harm for any pneumonia or lower respiratory tract infection associated with thiazolidinedione use is 239 (95% CI 117 to 1191).
Discussion
Our meta-analysis of 17 627 patients raises serious concern about a significant association between long-term thiazolidinedione use and pneumonia or lower respiratory tract infection leading to adverse events or serious adverse events among patients with type 2 diabetes (RRs≈40% increased risk). The absence of statistical heterogeneity, the consistency in the direction of effect, and the robustness of risk estimates for pneumonia or lower respiratory tract infection of varying severity suggest that this concern deserves detailed investigation. Any potential accentuation of risk with thiazolidinediones is of particular concern given that several recent epidemiological studies have reported an increased risk of pneumonia in patients with type 2 diabetes.33
The exact mechanisms by which thiazolidinediones increase the risk of pneumonia or lower respiratory tract infection are uncertain. Thiazolidinediones have glucocorticoid-like effects in the airways.3 4 These effects could induce susceptibility to pneumonia or lower respiratory tract infection, similar to the effect of glucocorticoids in chronic obstructive pulmonary disease.10 Thiazolidinediones have off-target effects on PPARδ at clinically relevant doses.34 Thiazolidinediones may exhibit proinflammatory activities in a PPARγ and PPARα independent manner by augmenting PPARδ signalling.34 Pioglitazone was also associated with an increased risk of hospitalisation for acute cholecystitis in a pooled analysis of 1526 patients (12 cases vs one for placebo).35 Further studies are required to elucidate the role of PPARs off-target and glucocorticoid effects in the development of serious infections such as pneumonia.
Limitations
The study has potential limitations, which mainly reflect the quality of reported data. The estimates are imprecise because of the low event rates in the trials. In the absence of patient-level data, we could not determine whether pneumonia or lower respiratory tract infection associated with thiazolidinedione use is immediate or there is a lag time to harm. Another possibility is that congestive heart failure events, a known harmful effect of thiazolidinedione use, were misclassified as pneumonia or lower respiratory tract infection. However, congestive heart failure was studied in several long-term trials.6 11 19 20 22 23 In the PROactive study, post-hoc adjudication of congestive heart failure and pneumonia outcomes reclassified only three pneumonia events—one in the pioglitazone arm (0.04%) and two in the placebo arm (1%).11 The effect of any potential misclassification on the meta-analysis is likely minimal because all trials (except RECORD) were double blind. Any misclassification of pneumonia or lower respiratory tract infection would be non-differential, and would bias our estimates towards the null. The absence of specific mortality data for pneumonia or lower respiratory tract infection from some of the included trials, and the low event rates prevent conclusions being drawn on the prognostic outcome of pneumonia or lower respiratory tract infection associated with thiazolidinediones.
Despite their limitations, the findings warrant further investigation. Individual patient data analysis could yield further information on the risk of pneumonia or lower respiratory tract infection with long-term use of thiazolidinediones. Stratified analysis ought to be conducted to determine any differences in the risk among people who smoke, people with chronic obstructive pulmonary disease, or those vaccinated with the influenza or pneumococcal vaccine. Clinical trials of thiazolidinediones among patients with type 2 diabetes, and ongoing trials in patients with obstructive lung disease, should monitor the risk of pneumonia using objective definitions with radiological and microbiological confirmation. The safety concern for long-term thiazolidinedione use needs to be replicated in carefully conducted epidemiological studies.
Conclusion
Long-term thiazolidinedione use is associated with a modestly increased risk of pneumonia or lower respiratory tract infection, and serious pneumonia or lower respiratory tract infection in patients with type 2 diabetes.
References
Supplementary materials
{kind=link}
{kind=link}
Footnotes
SS and YKL contributed equally.
Funding SS is supported by the Johns Hopkins Clinical Research Scholars Program. This publication was made possible by Grant Number 1KL2RR025006-03 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available on the website (http://www.ncrr.nih.gov/). Information on Re-engineering the Clinical Research Enterprise can be obtained from the website (http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp). The design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript was independent of any other sources of funding. Other Funders: NIH.
Competing interests Dr Furberg reports that he is a senior investigator and steering committee chair of the National Health, Lung, and Blood Institute–sponsored Cardiovascular Health Study (CHS), a cohort study to examine risk factors of coronary heart disease and stroke in the elderly. In 2004, the study received a grant for $280 000 from GlaxoSmithKline to determine the relationships between LpPLA-2 and various vascular diseases. The grant was primarily for the CHS central laboratory and the CHS coordinating center. Funding was channeled through Wake Forest University and Dr Furberg was the CHS principal investigator, but he received no salary support and the funding period ended 30 June 2006. Dr Furberg did not benefit personally from the grant and has no funding from any other manufacturers of antidiabetic medications. No other financial disclosures were reported. No specific financial interests and relationships and affiliations relevant to the subject of their manuscript were reported by Sonal Singh and Yoon Loke.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves