Article Text

Statistics from Altmetric.com
A 72-year-old woman was admitted in the Cardiology Department for respiratory insufficiency. ECG revealed atrial fibrillation, and echocardiography revealed heart failure with an estimated left ventricular ejection fraction of 25%. Chest roentgenogram revealed multiple nodules, and chest CT scan revealed multiple dense nodules surrounded by ground-glass attenuation (halo sign) with unilateral pleural effusion (figure 1). A bronchoalveolar lavage was performed to rule out any infection.
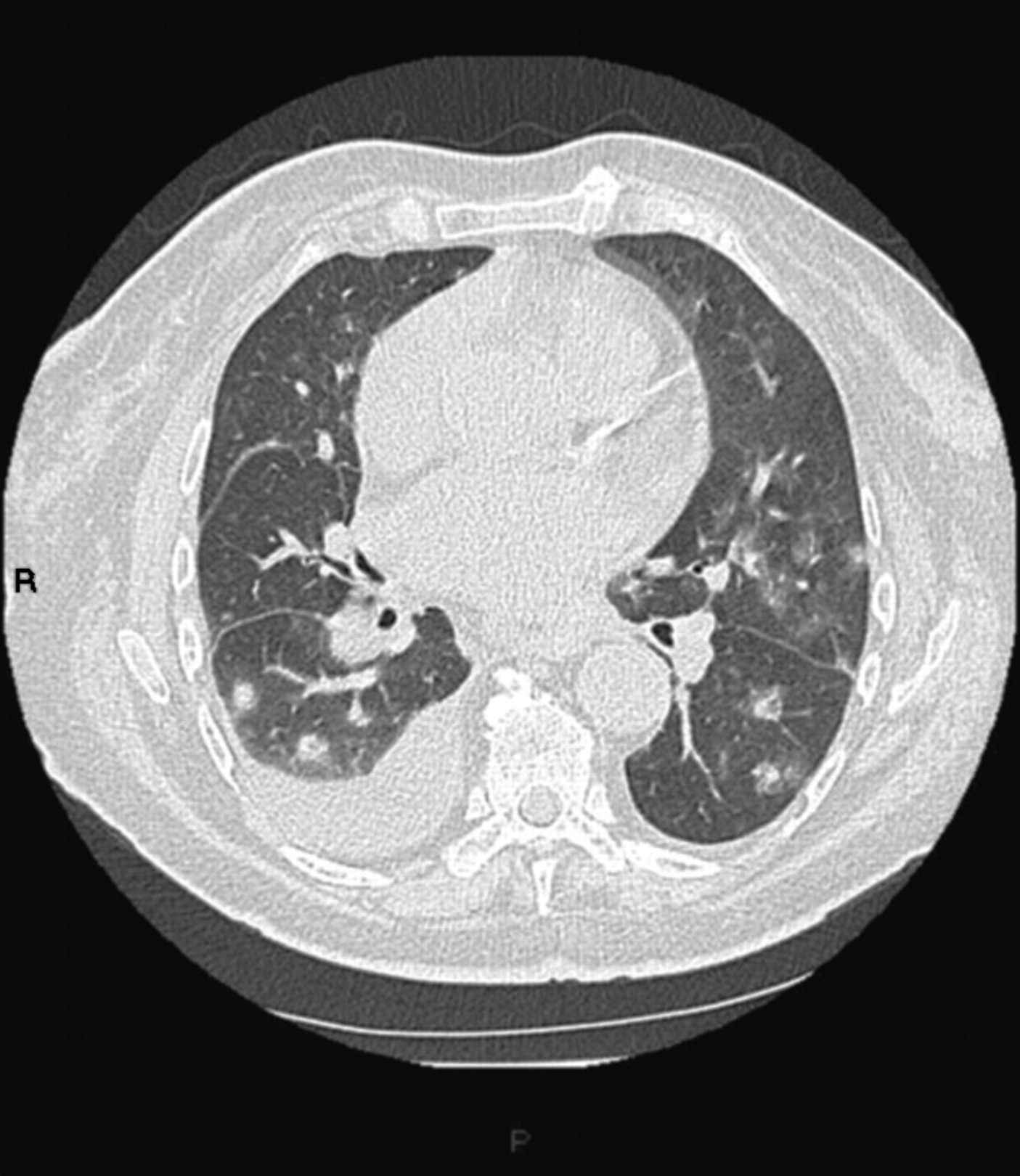
CT scan on arrival, revealing multiple nodules.
Anticoagulation was begun before a successful external cardioversion, followed by oral amiodarone treatment. Diuretics were increased without any other medication. One week later, a control chest CT scan revealed the disappearance of all nodules, as well as of the pleural effusion (figure 2).

{kind=link}
{kind=link}
CT scan after cardiac therapy.
Learning points
Multiple pulmonary nodules evoke metastatic cancer. and the rate of malignancy in nodules >20 mm is 81%.1 The halo sign, defined as ground-glass attenuation surrounding a solid nodule, is usually associated with haemorrhagic nodules.2 First described in immunocompromised patients with invasive aspergillosis, it has been reported in metastases from hypervascular tumours and vascularitis. The halo sign may also correspond to tumorous or inflammatory infiltration, as in bronchiolo-alveolar carcinoma, lymphoma or viral infection. Although the association of ground-glass opacities, interlobular septal and peribronchovascular interstitial thickening and predominantly right-sided pleural effusion is the most common presentation, cardiac insufficiency may occasionally take the form of multiple ill-defined centrilobular opacities that may have a nodular appearance.3 4
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.