Article Text

Statistics from Altmetric.com
A 50-year-old Caucasian man was presented to the emergency department with cough and progressive dyspnoea.
Plain chest x-ray showed multiple pseudo-nodular parenchymal opacities, partly confluent and calcified, prominent in the middle-basal lung fields (figure 1A).

(A) Plain chest x-ray showing multiple pseudo-nodular parenchymal opacities, partly confluent and calcified, prominent in the middle-lower lung fields. (B) Trans-axial HRCT slice with lung window setting showing diffuse bronchiectasis with thickened and calcified walls, associated with empty or filled bronchiolectasis (tree-in-bud sign). (C) Mediastinal window of an upper slice revealing the presence of circumferential thickening and calcification of tracheal wall with subsequent lumen distortion.
Volumetric high-resolution computed tomography (HRCT) confirmed multiple bilateral parenchymal nodules with lobulated margins and extensive calcifications due to diffuse bronchiectasis with thickened and calcified walls (figure 1B–C). Airways involvement was evident, characterised by submucosal deposits and lumen distortion mainly in the trachea, without sparing of the posterior membranous portion, and main and segmental bronchi (figure 2).
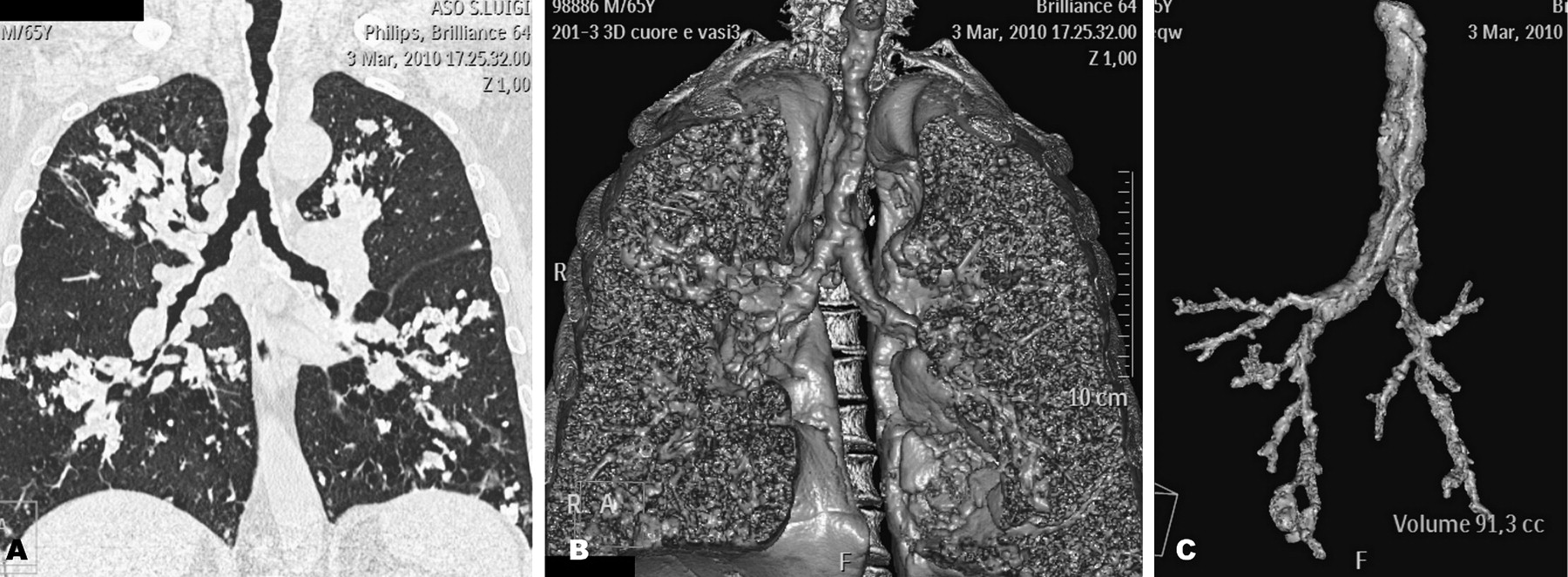
(A) Coronal reconstruction of volumetric HRCT with lung window setting and (B and C) 3D reconstructions demonstrating diffuse irregular narrowing of the trachea and main and segmental bronchi, with associated peripheral bronchiectasis and bronchiolectasis.
Biopsy specimen from bronchoscopy was striking for amyloid (figure 3), therefore the evidence pointed towards a diagnosis of primary tracheo-bronchial amyloidosis.

{kind=link}
{kind=link}
{kind=link}
Bronchial biopsy, magnification 100× (A) and 200× (B). Standard haematoxylin–eosin staining reveals abundant stromal deposits of amorphous eosinophilic substance, consistent with amyloid.
Learning points
There are four patterns of thoracic amyloid deposition, well demonstrated on CT: tracheo-bronchial, nodular parenchymal, diffuse alveolar/septal and lymphadenopathies.1
For the tracheo-bronchial form many radiological differential diagnoses should be considered, mainly Wegener's granulomatosis, tracheobronchopathia osteochondroplastica (that typically spares pars membranacea) and relapsing polychondritis.2
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Smokewaves