Article Text

Abstract
Objective To assess associations between exposure to smoking depictions in films and adolescent tobacco use in a British population cohort.
Methods Data on exposure to smoking in films and smoking behaviour were collected from 5166 15-year-old adolescents in the UK. Main outcome measures were smoking initiation (ever tried a cigarette) and current smoking status. Social, family and behavioural factors were adjusted for, together with alcohol use and peer smoking as potential mediators. Data from all existing cross-sectional studies examining the effects of exposure to smoking in films were summarised in a meta-analysis.
Results Higher exposure to smoking in films was associated with a dose-response increase in the risk of smoking initiation even after adjusting for confounders. Adolescents in the highest exposure quartile were 1.73 (95% CI 1.55 to 1.93) times (RR) more likely to initiate smoking than those in the lowest quartile. They were more likely to report current smoking after adjusting for social and familial factors (RR 1.47 (95% CI 1.07 to 2.02)), but the association attenuated after including behavioural factors (RR 1.34 (95% CI 0.95 to 1.87)). The meta-analysis shows that, after aggregation of all relevant data, viewing smoking in films increases the risk of smoking onset by over 100% (combined RR 2.13 (95% CI 1.76 to 2.57)) and the risk of current or established smoking behaviour by 68% (combined RR 1.68 (95% CI 0.40 to 2.01)).
Conclusions This study provides evidence that adolescents in the UK and elsewhere who are exposed to smoking depictions in films are more likely to initiate smoking. Given the association between smoking and poor health outcomes, these data justify a review of film ratings.
- Cigarette smoking
- adolescent behaviour
- alspac
- psychology
- respiratory infection
- tobacco and the lung
- bronchoscopy
- rare lung diseases
- lung cancer
Statistics from Altmetric.com
- Cigarette smoking
- adolescent behaviour
- alspac
- psychology
- respiratory infection
- tobacco and the lung
- bronchoscopy
- rare lung diseases
- lung cancer
Key messages
What is the key question?
Is exposure to smoking depictions in films associated with smoking behaviour in adolescence?
What is the bottom line?
Adolescents who watch more films with smoking depictions are more likely to initiate smoking and more likely to be current smokers.
Why read on?
The strength of the association between smoking depictions in films and smoking behaviour in adolescence persists even after adjusting for social, family and behavioural confounders.
Introduction
One way in which children learn is by modelling the behaviour of others.1 While there is a convincing body of research examining the influence of family and friends on behaviour, there is also increasing evidence that exposure to risky behaviour in the media (eg, via television programmes and films) is associated with increased risky and delinquent behaviours such as tobacco and alcohol use in childhood and adolescence.2 3 Film ratings systems address violence by restricting films high in violence to older age groups. However, ratings systems do not address smoking, the commonest cause of preventable mortality in developed nations.
Research in the USA has shown that depictions of cigarette smoking in cinema films depict smoking as an attractive behaviour rather than associating it with adverse outcomes,4 making it similar to aspirational tobacco advertising imagery which is banned in the UK. Exposure to smoking in films is associated with adolescent attitudes towards smoking in the USA,5 and there is a dose-response between exposure and smoking behaviour.6–9 Adolescents in the USA with high exposure to films with smoking are 2–3 times more likely to start smoking than others, even after adjusting for factors associated with increased tobacco use.9 These findings have been replicated in New Zealand,10 Mexico11 and Germany.12 More than half of films shown in the UK that contain smoking are rated UK15 or below, so UK youth are clearly exposed, but it is unclear whether the association between exposure to smoking in films and actual smoking behaviour exists for contemporary UK youth. One cross-sectional study of Scottish young adults reported no association, raising questions about whether UK youth respond to films in the same way as youths from other developed nations. We examined this association at age 15 years in a large contemporary cohort, the Avon Longitudinal Study of Parents and Children (ALSPAC). Because the cohort contains rich information about the backgrounds of the children and their parents, we were able to control for characteristics of the child that might confound or mediate the relationship.
Methods
Participants
ALSPAC is a prospective study investigating social, environmental, biological and genetic influences on the health and development of children and has been described in detail elsewhere (http://www.alspac.bris.ac.uk). Briefly, 14 541 pregnant women living in a Bristol-based health district in the former County of Avon, UK, with an expected delivery date between 1 April 1991 and 31 December 1992 were enrolled in the study. Detailed information has been collected using self-administered questionnaires (completed by the mothers and, since the age of 7 years, also by the children), data extraction from medical notes, linkage to routine information systems and at research clinics for study children. Mothers consented to join the study at recruitment. Up to the age of 16 years, study children provided assent to take part and subsequently have provided their own consent. As with most large cohort studies, attrition is an issue. For the current study, data on 5509 adolescents were available from the 15-year clinic. Of these, 5367 had smoking data and 5169 had film data, allowing 5166 with both variables to be used for analysis. The proportion of the cohort that continues to take part in the study has been shown to have experienced fewer adverse circumstances than those who have dropped out.13
Measures
Exposure to smoking in films
In the 15-year clinic, a computer-assisted interview (CASI) was used to ask adolescents whether they had seen 50 randomly selected films. These were drawn from a list of 366 popular contemporary films comprising the top 70 US box office hits released between 2001 and 2005. The number of smoking occurrences in each film was counted by trained coders and the total exposure was the sum of the number of occurrences in each film.14 This method is described in detail elsewhere.9 15 The exposure variable was the number of smoking occurrences in films classified into quartiles (≤38, 39–68, 69–108, ≥109).
Smoking behaviour
As part of the 15-year CASI, cohort members were asked questions about smoking. Data were used to derive two outcome variables: (1) smoking initiation (‘Ever tried a cigarette, even just a puff?’) and (2) current smoking (‘Do you smoke every week?’).
Confounding variables
We selected factors associated with smoking in previous studies15 16 that were collected prospectively and available for the whole cohort. In addition, we controlled for variables not available in previous work including breast feeding (a proxy for social position), childhood disorders at age 7 and current alcohol use. Confounders were chosen on the basis that a complexity of social and environmental factors influence both behaviour and outcomes across the life course,17 and those that we believed would give additional insight into adolescent smoking behaviour were adjusted for in the analysis.
Antenatal data were collected as follows. At around 8 weeks of pregnancy the mother was asked to record whether her home was mortgaged, owned, council/Housing Association rented, privately rented or other; whether she was currently married, divorced/separated, widowed or never married; and her date of birth. At 18 weeks she was asked to list all her previous pregnancies, from which parity was derived. Responses to questions asked at 18 and 32 weeks were used to determine whether the mother had smoked during pregnancy. Partner smoking data were obtained at 18 weeks from the partner if available, otherwise from the mother. The 32-week antenatal questionnaire asked each mother to record her own and her partner's occupation and this was used to allocate social class groups (I, II, III manual, III non-manual, IV, V) using the 1991 Office of Population, Censuses and Surveys classification; the lowest class of mother and her partner was used in the analysis. At this time the mother was also asked five questions about financial difficulties which were combined to create a score ranging from 0 to 15 (higher values indicating more financial difficulties) and then divided into quartiles. She was also asked about her highest education level, categorised into none or CSE (national school examinations at age 16), vocational, O-level (national school examinations at age 16, higher than CSE), A-level (national school examinations at age 18) or university degree. Regarding data collected postnatally, infant gender was recorded in the delivery room or abstracted from obstetric records or birth notifications. Breast feeding information (exclusive, partial or never breast fed by 2 months of age) was obtained from a questionnaire sent to mothers when the child was approximately 6 months old.
The Development and Well-Being Assessment18 was used to assess childhood disorders when the child was aged 7 years. These are behavioural and emotional disorders defined by DSM-IV19 and, for the purposes of this paper, we included diagnoses for attention deficit/hyperactive disorder (ADHD), conduct disorder, anxiety and depression disorders.
At approximately 13 years of age further data about the child's behaviour were collected using CASI. Nine items from the intensity seeking scale of Arnett's Inventory of Sensation Seeking20 were used to measure sensation seeking (the original item ‘in general I work better under pressure’ was omitted from the CASI and so could not be included, and two items related to cinema films were removed (‘I stay away from movies that are said to be frightening or highly suspenseful’ and ‘I like a movie where there are a lot of explosions and car chases’)). All other intensity seeking items of Arnett's Inventory of Sensation Seeking were used. Study children were asked to rate whether each item described them (a) very well, (b) somewhat, (c) not very well or (d) not at all. The combined sensation seeking scale was derived by adding the scores and dividing into quartiles (with the top quartile representing the highest level of sensation seeking).
To quantify parental monitoring, nine questions based on parent's knowledge of their child's whereabouts, activities and associations were asked again using CASI at 15 years of age.21 22 These included items such as ‘How often do your carers/parents know what you do in your free time?’ and ‘How often do your carers/parents know what you spend your money on?’ Responses were recorded as (a) never, (b) hardly ever, (c) sometimes, (d) most of the time or (e) always, then combined to obtain an overall score which was divided into quartiles (the top quartile representing the highest level of parental monitoring).
Mediating variables
At age 15 years the CASI included a question on current alcohol use and responses were categorised as (a) no alcohol use, (b) alcohol use less than once per week or (c) alcohol use at least once per week. Participants were asked how many of their friends had smoked cigarettes during the last year and this was recorded as (a) none, (b) one/some or (c) most/all friends. Previous work23 24 has suggested that both alcohol use and having peers who smoke mediates the relationship between exposure to smoking in films and onset of smoking behaviour.
Statistical analysis
Means and SDs were calculated for continuous variables that were approximately normally distributed (number of films watched, age of child at clinic, maternal age), medians and IQRs for skewed variables (number of smoking depictions in films) and proportions for categorical variables (all other variables). A Spearman correlation coefficient was calculated to assess the linear association between number of smoking depictions in films and number of films watched. Associations between exposure (number of smoking depictions in films) and outcomes (smoking initiation, current smoking status) were assessed using Poisson regression with robust error variance to estimate risk ratios and CIs. This approach was used as ORs (obtained from logistic regression) are poor approximations of risk ratios (RRs) if the outcome prevalence is high.25 The interaction between gender and the exposure variable was formally tested when modelling associations between exposure and outcomes in order to determine whether separate models were required for males and females given that a sex difference in risky behaviour is often observed.
Associations between exposure and outcomes were examined after adjusting cumulatively for potential confounding factors also associated with exposure and outcomes (models 1–5): age at the 15-year clinic and gender (model 1); age, gender and social factors (social class, financial difficulties, housing) (model 2); age, gender and family influences (maternal age, maternal education, marital status, parity, breast feeding, maternal smoking, partner smoking, parental monitoring) (model 3); age, gender, social factors and family influences (model 4); behavioural variables were added into model 5 (age, gender, social factors, family influences and behavioural factors (ADHD, conduct disorder, anxiety, depression, sensation seeking)). In model 6 the data were adjusted for mediators (own alcohol use and peer smoking behaviours) thought to be part of the causal pathway from film exposure to adolescent smoking; including these as confounders in the other models may have over-specified the model and underestimated any associations between exposure and outcome. Model 1 was repeated restricting to those with complete sets of mediator information to ensure that any change in estimated RR observed in models 2–5 was attributable to confounding rather than missing data.
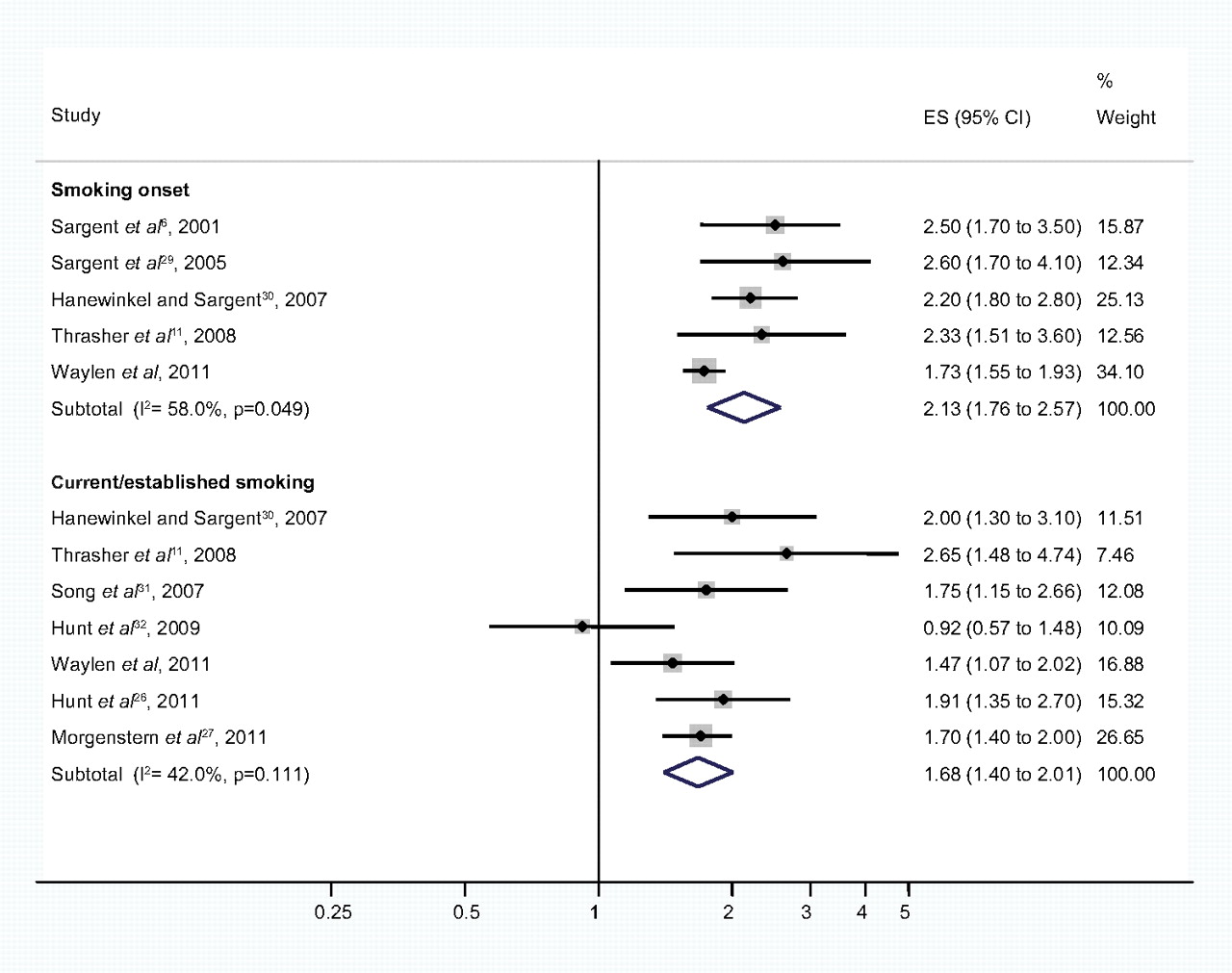
We summarised the published cross-sectional data by conducting a meta-analysis for all studies that assessed exposure to smoking in films in a similar fashion. The systematic PubMed search strategy “(movies[All Fields] OR (“motion pictures as topic”[MeSH Terms] OR (“motion”[All Fields] AND “pictures”[All Fields] AND “topic”[All Fields]) OR “motion pictures as topic”[All Fields] OR “films”[All Fields])) AND (“smoking”[MeSH Terms] OR “smoking”[All Fields])” was used to identify other studies. The strategy identified 145 publications, 10 of which involved cross-sectional assessments of smoking among adolescents and young adults. Of these, one cross-sectional trend study was excluded, two were excluded because exposure estimates involved assessing parental restrictions on R-rated films and two were excluded because the assessment involved only whether their favourite film star smoked. In order to compute the forest plot (figure 1), adjusted ORs from all published cross-sectional studies for both smoking onset and current/established smoking outcomes (quartile 4 vs quartile 1) were combined using meta-analysis. Note that the ORs from these published studies are likely to be overestimates of the association between smoking depictions in films and adolescent smoking as it is likely that the outcomes were non-rare. Figure 2 is the same forest plot but with the addition of data from the accompanying papers by Hunt et al26 and Morgenstern et al27 published in this issue of the journal and the findings of this study. Random effects models were fitted as there was some evidence of heterogeneity between studies as assessed by the Higgens I2 statistic.28 All analyses were performed in Stata V.10.1 (StataCorp).
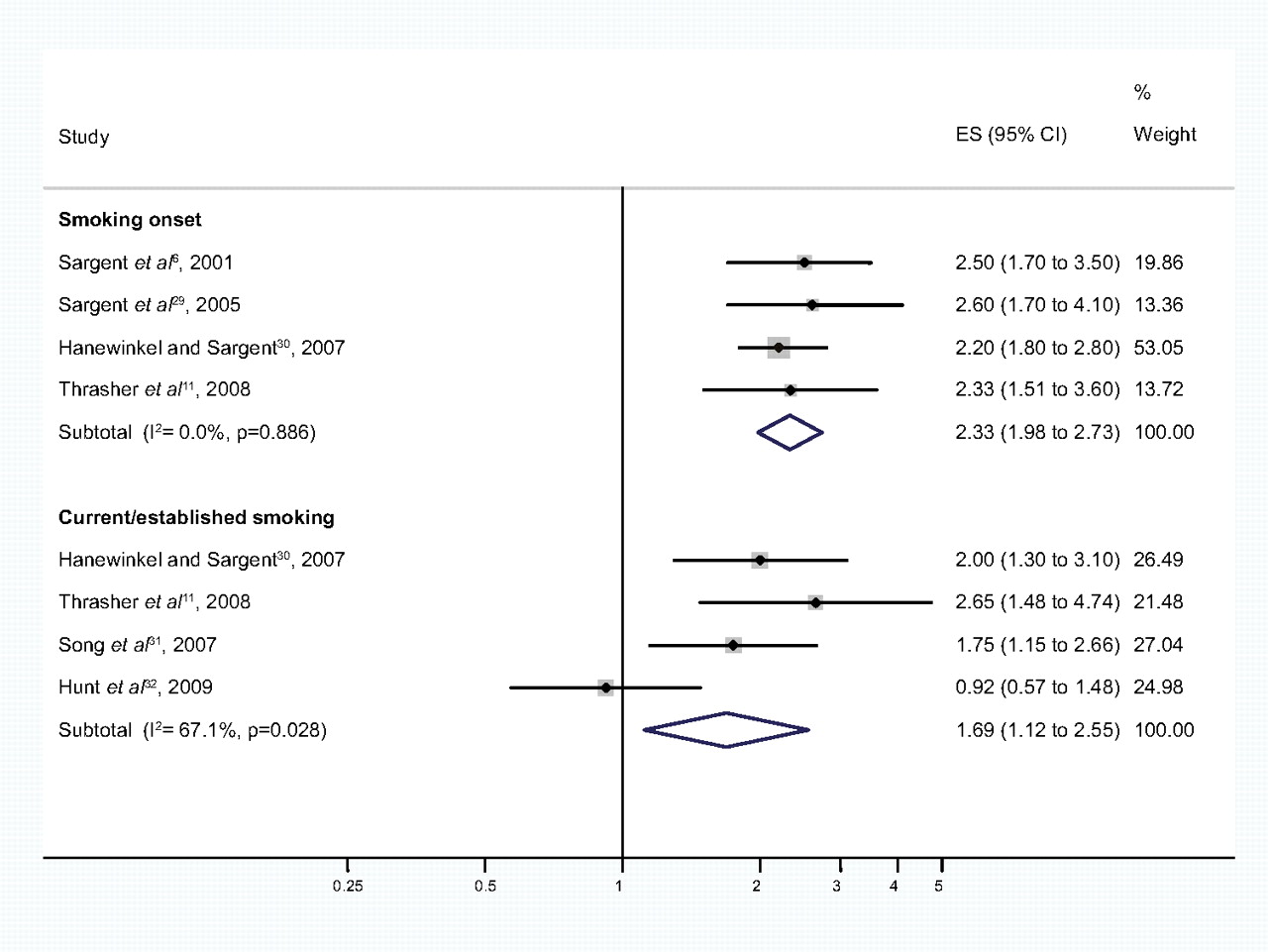
Meta-analysis of film exposures and smoking outcomes in cross-sectional studies published before 2011. Effect size (ES) = adjusted OR for smoking outcomes for quartile 4 versus quartile 1 of film exposures. I2 test is for heterogeneity. Weights are from random effects analyses.
{kind=link}
{kind=link}
Meta-analysis of film exposures and smoking outcomes in all cross-sectional studies published to date. Effect size (ES) = adjusted OR for smoking outcomes for quartile 4 versus quartile 1 of film exposures. I2 test is for heterogeneity. Weights are from random effects analyses.
Results
Data on 5166 adolescents with both film and smoking data were available for analysis from the 15-year clinic. The characteristics of the study sample are shown in table 1. Their mean age was 15.5 years and there were slightly more females then males (53.1%). The median (IQR) number of smoking occurrences in films was 68 (38–108) and the mean (SD) number of films seen was 17.7 (8.3). The Spearman correlation between the number of smoking depictions and the number of films seen was 0.79 (p<0.001). The percentage of study children who had ever tried smoking was 47.4% and 9.8% were current smokers, having smoked in the past 30 days. All covariates and potential mediators are summarised in table 1.
Summary of the characteristics of the 5166 cohort members with smoking and film data available at approximately age 15 years
There was no statistical evidence for interactions between gender and exposure variables when modelling associations with the outcome (p=0.1–0.7), so all analyses were carried out on the whole cohort.
Exposure to smoking depictions and smoking outcomes
Associations between smoking depictions in films and smoking outcomes are shown in table 2. There was an increasing trend across quartiles of movie smoking exposure (p for trend <0.001), with a 59% increase in the risk of smoking initiation for the highest quartile of film smoking exposure compared with the lowest after adjusting for all potential confounders in models 2–5. After adjusting for mediators (own alcohol use and peer-smoking, model 6), there was still a 32% increase in the risk of smoking initiation for those in the highest quartile of exposure. When current smoking behaviour rather than smoking initiation was the outcome, there was no evidence for an association with film smoking exposure after adjustment for mediators (p for trend=0.6).
Associations between film exposures and smoking outcomes
Meta-analysis of cross-sectional studies
Figure 1 shows the results of the meta-analysis excluding the data from the current study and also those in the accompanying papers published in this issue of the journal.26 27 Previously, the overall effect size for smoking onset after exposure to smoking in films was 2.33 (95% CI 1.98 to 2.73) and that for current or established smoking was 1.69 (95% CI 1.12 to 2.55).
Figure 2 shows the combined effect size for all cross-sectional studies (including those published in the accompanying papers) that examine the effect of exposure to smoking depictions on smoking onset. When the data from the three studies published in this issue of the journal are added to the existing cross-sectional data, there is a slight reduction in the effect size for smoking onset to 2.13 (95% CI 1.76 to 2.57). There is no real change in the effect size for current smoking status 1.63 (95% CI 1.40 to 2.01) but the CIs for this outcome are smaller, indicating that this estimate of effect size is more precise.
Discussion
Our results confirm an association between exposure to smoking in films and youth smoking in the UK. This association is consistent with the association reported in other populations. At age 15, adolescents in this Bristol-based birth cohort with high exposure to smoking in films were almost twice as likely to initiate smoking as those with low exposure. However, the influence of smoking depictions in films was attenuated when family factors including parental monitoring were included in the model and attenuated further when behavioural factors were included. A similar pattern is seen for current smoking status, but that effect is largely attenuated by the inclusion of family influences. The meta-analysis shows that results from cross-sectional studies conducted in the USA, Mexico, Germany and the UK give consistent results for the association with smoking onset and current or established smoking, despite different study characteristics.
One strength of this paper is that this birth cohort afforded a rich array of individual and family descriptors collected prospectively over time and not previously controlled for. Even after controlling for social, family and behavioural factors and mediating variables, increased exposure to smoking depictions in films increases the risk of smoking initiation in adolescence. This study is also consistent with findings from other studies in which alcohol use and having peers who smoke12 23 24 33 attenuate the effect of exposure to smoking in films on smoking initiation. Further research is required to examine mediating and moderating effects of these variables and to investigate the mechanisms by which smoking depictions inform and shape the attitudes and behaviours of adolescents.
The paper is subject to several limitations. We gave the study participants a list of films but only recorded those they had seen; we have no record of the number of times films were seen or of films not seen. Also, the data for peer behaviour and alcohol use—mediators which reduce the association between exposure to smoking depictions and smoking initiation—were collected concurrently so we cannot determine whether these relationships are causal or the likely direction of causality. Finally, as with most large cohort studies, attrition of those in more adverse circumstances could affect our ability to generalise results to groups who were more likely to drop out of the study. However, previous work using ALSPAC data13 has shown that drop-out from the ALSPAC cohort is selective and therefore regression models are likely to be only marginally affected.
Given the likelihood that the observed association may be causal (as noted by the US National Cancer Institute),34 it is important to consider public health implications as exposure to smoking depictions is universal in this instance, with virtually all adolescents reporting that they had seen at least one film from the list. In the subsample of the cohort who had seen 69 or more smoking depictions in films, the proportional attributable risk for the association between smoking depictions and smoking onset is large, in the order of 30%. It should further be noted that young people in the UK are exposed to 28% more smoking depictions in cinema films than youth in the USA because 79% of films rated as ‘adults only’ in the USA are rated as suitable for young people in the UK.35 Finally, randomised controlled trials to investigate the influence of smoking depiction on smoking behaviour would almost certainly be deemed unethical, so observational studies may be the most rigorous that we can achieve.
If the dose-response relationship between smoking depictions and smoking initiation is causal—as shown in other cross-sectional and longitudinal work36—then, in the first instance, preventing adolescents from being exposed to smoking depictions by raising the certification to ‘18’ in the UK is likely to lower smoking rates among youth. Given that smoking depictions in films are not consistent with the ban on smoking in public places in the UK and that the relationship may be causal, a precautionary principle should be pursued. Films ought to be rated by exposure to smoking in the same way that they are currently rated by level of violence: smoking and its adverse consequences are certainly a larger public health problem. Such a policy would also make the movie ratings system consistent with the ban on tobacco advertising in all other media.
The results of this study are consistent with others that have examined the association between exposure to smoking depictions in films and smoking initiation. In this population cohort, young people exposed to the greatest number of smoking depictions are 73% more likely to have tried smoking and almost 50% more likely to be current smokers than those exposed to very few smoking depictions. This association remains even after adjustment for confounding and mediating variables. Given the adverse effects of tobacco use on health, the findings of this study surely justify a review of the film rating categories in the UK and serious consideration given to incorporating smoking into the ratings system.
Acknowledgments
The authors are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses. The UK Medical Research Council, the Wellcome Trust and the University of Bristol provide core support for ALSPAC.
References
Footnotes
See Editorial, p 844
Funding JDS received funding for the content analysis of movie smoking from the National Institutes of Health (CA 77026) and the American Legacy Foundation.
Competing interests None.
Ethics approval Ethics approval was provided by Avon Longitudinal Study of Parents and Children (ALSPAC) Law and Ethics Committee and the local research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Smoking
- Smoking
- Smokewaves