Article Text

Abstract
A pathological diagnosis of pulmonary Langerhans cell histiocytosis (PLCH) usually requires a surgical lung biopsy. To date, diagnosis of PLCH by core needle biopsy has not been reported. Three cases are presented of PLCH diagnosed by CT-guided core biopsy in adult female smokers found to have multiple small bilateral lung nodules. The nodules biopsied were 5 mm, 7 mm and 1 cm in size, and showed interstitial expansion by Langerhans cells and eosinophils. CT-guided core biopsy should be considered as one of the less invasive techniques by which a pathological diagnosis of PLCH can be established.
- Histology/cytology
- imaging/CT MRI etc
- interstitial fibrosis
- tobacco and the lung
Statistics from Altmetric.com
Case 1
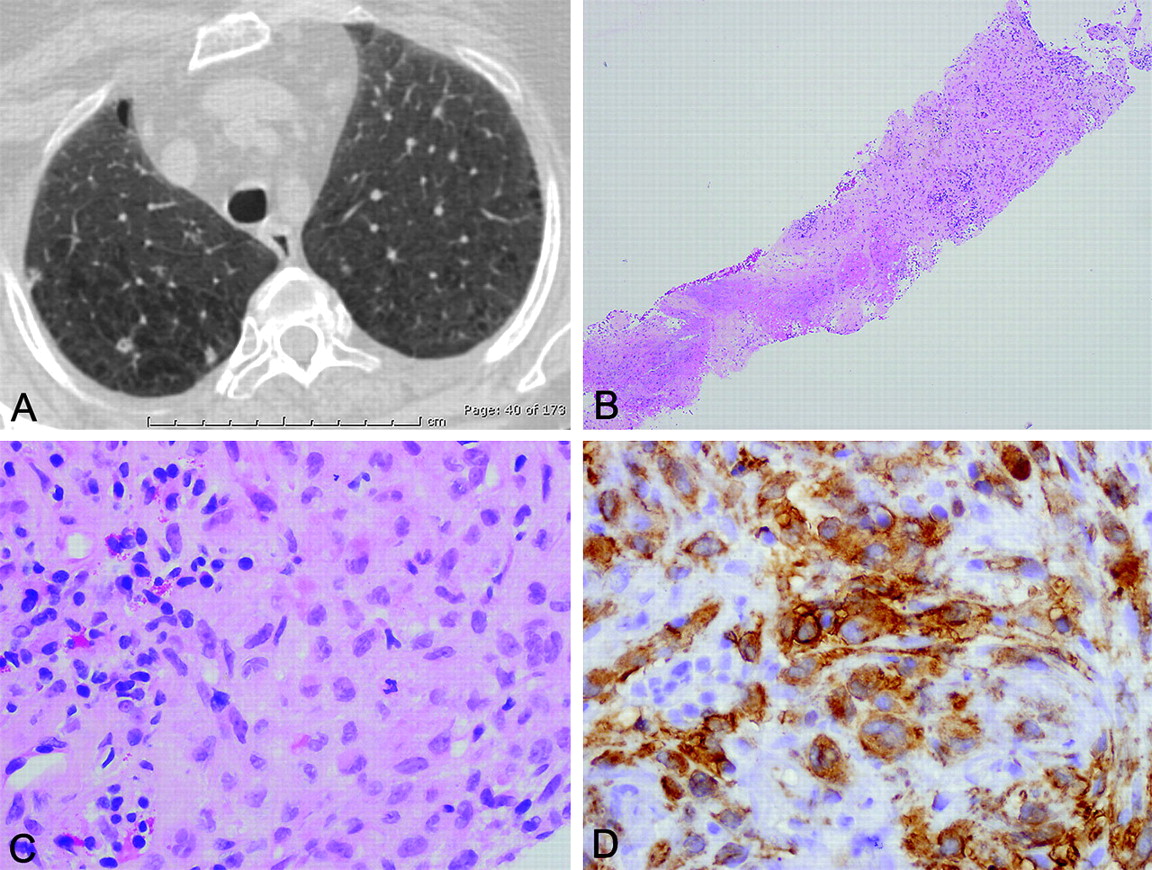
A 68-year-old female 30 pack-year active smoker was referred for evaluation of pulmonary nodules discovered incidentally on an abdominal CT scan performed for evaluation of abdominal pain. She was asymptomatic from a pulmonary standpoint. Chest CT showed multiple small bilateral lung nodules, most in the 3–5 mm range, some showing cavitation (figure 1). CT-guided biopsy of a 5 mm nodule in the right lower lobe was performed using a 19-gauge guiding needle and a 20-gauge biopsy gun. No material was sent for cultures.
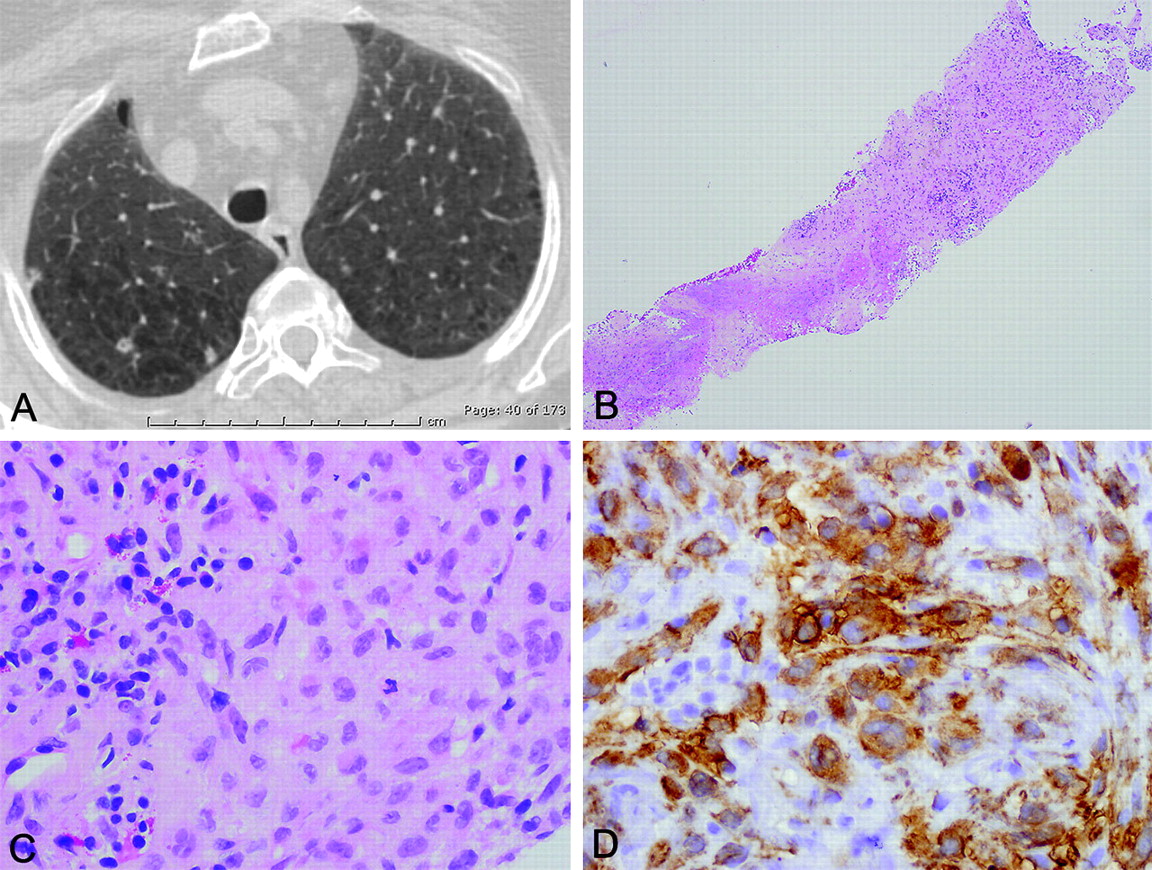
Case 1, radiological and pathological findings. (A) Chest CT showing three irregularly marginated nodules in the upper lobe of the right lung, one of which is cavitary, on a background of lung destruction that has the appearance of emphysema. (B) Low magnification view of one of the cores obtained by needle biopsy, showing cellular interstitial infiltrate (top right) and focal necrosis (bottom left) (H&E, original ×40). (C) High magnification of cellular interstitial infiltrate, showing numerous Langerhans cells (right) with characteristic irregular nuclear contours. A few eosinophils are present at top left (H&E, original ×400). (D) Langerhans cells are positive for CD1a (CD1a antibody, diaminobenzidine counterstain, original ×400).
Case 2
A 63-year-old 24 pack-year female active smoker with a history of systemic lupus erythematosus, stable on immunosuppressant treatment, was evaluated for pulmonary nodules discovered on a chest CT performed for dyspnoea. There were no other active pulmonary complaints. Chest CT showed multiple subcentimetre nodules in both lungs (figure 2). The differential diagnosis included metastatic tumour, infection and rheumatoid nodules. A 7 mm right lower lobe nodule was sampled by CT-guided core biopsy. Of the eight cores obtained, four were sent for cultures and four for pathological examination. Cultures were negative.

Case 2, radiological and pathological findings. (A) Chest CT showing a spiculated nodule in the right lung. (B) Low magnification of lung tissue obtained by core needle biopsy showing expansion of the interstitium by a cellular infiltrate (H&E, original ×40). (C) High magnification showing large numbers of Langerhans cells, numerous eosinophils and a few pigment-laden histiocytes (H&E, original ×400). (D) The Langerhans cells are positive for S-100 protein (S-100 antibody, alkaline phosphatase red counterstain, original ×400).
Case 3
A 55-year-old female active smoker with a 60 pack-year history of cigarette smoking was lifting heavy objects when she twisted a back muscle. A chest x-ray performed during her examination showed an incidental 1 cm nodule in the right upper lobe. A chest CT was subsequently performed, and showed multiple bilateral pulmonary nodules, the largest of which was the right upper lobe nodule previously noted (figure 3). Pulmonary function tests demonstrated moderate obstruction. The FEV1/FVC (forced expiratory volume in 1 s/forced vital capacity) ratio was 0.58 and the DLCO (diffusing capacity for carbon monoxide) was 49% of predicted. A metastatic malignancy was suspected. A bone scan performed to evaluate for metastases was negative. CT-guided biopsy of the 1 cm right upper lobe nodule was performed. Cultures were not obtained.

{kind=link}
{kind=link}
{kind=link}
Case 3, radiological and pathological findings. (A) This axial chest CT image at lung window settings shows multiple small nodules in the periphery of the upper part of the right upper lobe. The largest of the nodules was the target of the subsequent core needle biopsy. (B) Core needle biopsy at low magnification, showing interstitial expansion (H&E, original ×40). (C) High magnification, showing Langerhans cells and eosinophils (H&E, original ×40). (D) The Langerhans cells are positive for S-100 (S-100 antibody, alkaline phosphatase red counterstain, original ×400).
Pathological findings
Pathological findings were similar in all three cases, showing expansion of fibrotic pulmonary interstitium by Langerhans cells along with pigment-laden histiocytes and scattered eosinophils (figure 1–3). Focal necrosis was additionally present in case 1. Each case also showed respiratory (smokers') bronchiolitis, characterised by the presence of pigment-laden macrophages within the airspaces. The Langerhans cells were positive for S-100 and CD1a in all three cases.
Discussion
Pulmonary Langerhans cell histiocytosis (PLCH) is a form of interstitial lung disease characterised by bilateral pulmonary nodules, often accompanied by cysts. Surgical lung biopsy is by far the most common modality used for a definitive diagnosis of PLCH (table 1).1–5 Transbronchial biopsies may sample diagnostic areas, but the yield is lower (∼21%).5 Quantification of Langerhans cells in bronchioloalveolar lavage fluid (aided by CD1a immunostaining) has been advocated by some, but this method lacks specificity and is not widely used.
Diagnostic modality used for tissue diagnosis of PLCH in five large studies
To the best of our knowledge, this is the first report of PLCH diagnosed by CT-guided core biopsy of the lung. None of our cases represents an attempt to confirm a clinico-radiological suspicion of PLCH by means other than surgical biopsy. Instead, these cases were encountered, in most cases fortuitously, during investigation of pulmonary nodules of uncertain significance. A diagnosis of PLCH was not entertained in any case prior to biopsy. As in this report, the lung nodules of PLCH are often discovered incidentally during a radiological work-up for an unrelated condition. Although high-resolution CT scans may permit a definitive diagnosis in patients with the classic combination of bilateral lung nodules and cysts, this is often not the case in practice. The clinical and radiological considerations usually include metastatic malignancy and infection. Thus a definitive diagnosis typically requires tissue confirmation.
There are probably two explanations why CT-guided core biopsy has not been previously utilised to diagnose PLCH. First, core needle biopsy is not considered suitable for the diagnosis of diffuse interstitial lung disease, which typically requires larger tissue samples that are more likely to include diagnostic areas. However, it is important to recognise that although PLCH is a form of interstitial lung disease, it characteristically forms nodules, which frequently contain diagnostic clusters of Langerhans cells. It is not unreasonable, therefore, that a guided core biopsy of these nodules would sample diagnostic material. Secondly, radiologists may shy away from using core biopsy to diagnose PLCH given the small size of the nodules, which are often only a few millimetres. In all our cases, the nodules sampled were ≤1 cm in size, but this did not preclude retrieval of adequate material.
A clinical feature worthy of note in our cases is the relatively older age of our patients (55–68 years) compared with cases of PLCH reported in the literature, where the mean age ranges from 28 to 40 years.3–5 We believe that the slightly higher age of our patients may have made metastatic malignancy a particularly strong consideration in the differential diagnosis in these patients, this being a situation where CT-guided core biopsy is often used at our institution.
In the same time frame that these cases were diagnosed, we encountered two cases of clinico-radiologically suspected PLCH in which CT-guided core biopsies of subcentimetre nodules failed to sample lesional tissue. One of these patients was a 32-year-old male smoker with several bilateral solid and cystic lung nodules ranging from a few millimetres to 7 mm. A 6 mm nodule in the right upper lobe was sampled by CT-guided core biopsy, but yielded lung parenchyma unremarkable except for the presence of respiratory bronchiolitis. The other patient was a 51-year-old female smoker with multiple bilateral lung nodules, most of which were non-calcified. The nodules ranged from a few millimetres to 5 mm. The largest nodule was initially a cystic area adjacent to a calcification, but subsequently developed a soft tissue component. This 5 mm nodule was sampled by CT-guided core biopsy, and showed a necrotising granuloma without any organisms. In both cases, a subsequent surgical lung biopsy confirmed a diagnosis of Langerhans cell histiocytosis. We could not discern any differences between the lesion in the first ‘missed’ case and the ones that did lead to a diagnosis by CT-guided core biopsy. In the second ‘missed’ case, the core biopsy sampled an incidental granuloma which, in retrospect, was not representative of the pathology in the rest of the lung. This lesion was calcified, in contrast to the three adequately sampled lesions that form the basis of this report (‘hits’), which were not calcified. In view of the variable results described above, we view CT-guided core biopsies not as replacing surgical biopsy as the gold standard, but merely as providing an alternative method with potential for providing diagnostic material in a less invasive manner. We would like to emphasise that our study was not designed to determine the yield of CT-guided core biopsy, and that larger series will be required to address this issue.
In summary, CT-guided core biopsy should be added to the list of techniques by which a pathological diagnosis of PLCH can be established. Although the subcentimetre nodules of PLCH are usually considered too small to be approached with a core biopsy, our cases demonstrate that even lesions as small as 5 mm can be sampled by this technique, yielding diagnostic material.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.