Article Text

Statistics from Altmetric.com
ELITE trial in cystic fibrosis
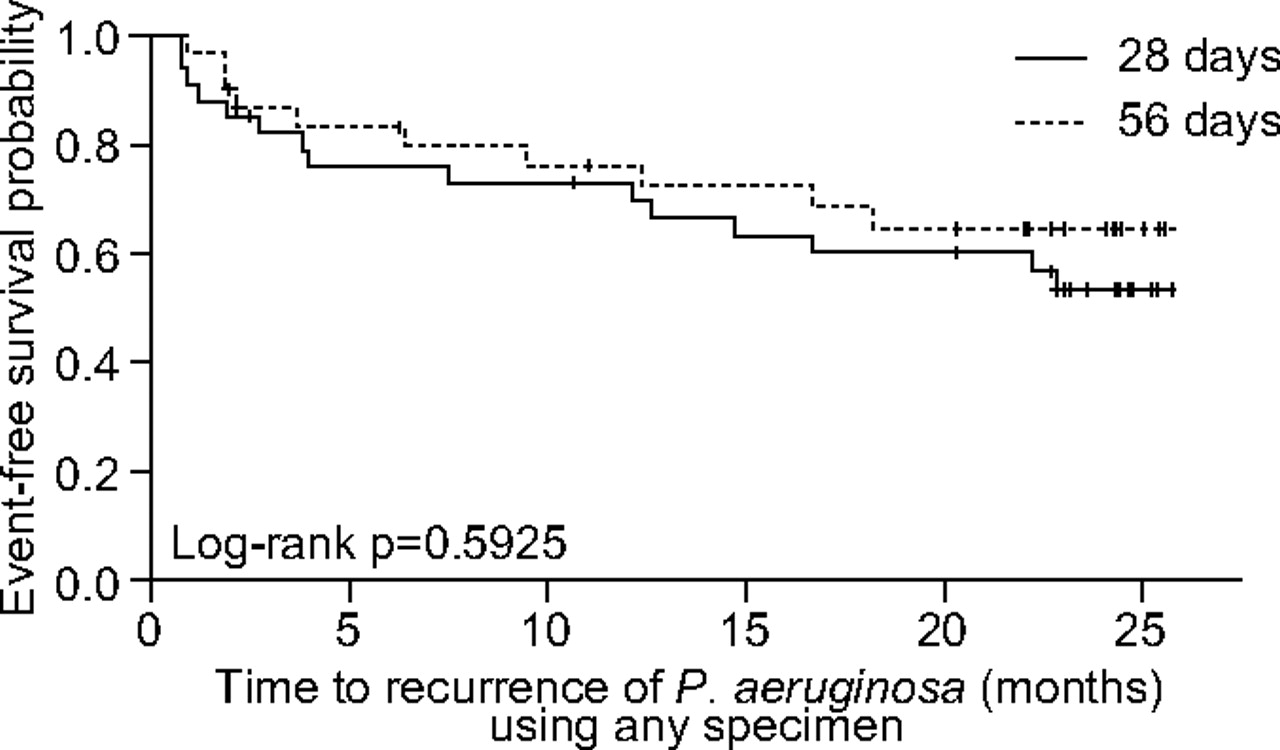
As Smyth informs in his editorial in this month's Thorax to the accompanying paper by Ratjen and colleagues, the most significant event in the life of a person with cystic fibrosis (CF) is the acquisition of chronic pulmonary infection with Pseudomonas aeruginosa. However it is possible to eradicate P aeruginosa in early stages of infection before formation of biofilms and this is now usual clinical practice, though there have been few studies comparing eradication regimes. Ratjen and colleagues report the results of the ELITE trial where inhaled tobramycin was used for 28 days for early eradication, followed by randomisation to either stop therapy or have another 28 days of tobramycin. There was no difference in the primary or secondary outcomes with the 28 day or 56 day regime and therapies were well tolerated. Smyth concludes that ELITE is the first step in determining the optimal eradication regime and now cystic fibrosis centres need to collaborate to perform more multicentre trials of these regimes.
NIV intensity in stable hypercapnic COPD
Although home non-invasive ventilation (NIV) is now increasingly used in patients with stable hypercapnic COPD, the evidence for benefit is not strong. One reason for the variability in studies may be differences in inspiratory pressures used during NIV though it is important that effective ventilation is administered to this patient group especially overnight. In this issue, Dreher and colleagues describe a randomised crossover trial comparing 6 weeks high-intensity with low-intensity NIV in patients with stable hypercapnic COPD. The results show that high-intensity NIV was better tolerated than low-intensity NIV and produced better control of nocturnal hypoventilation, dyspnoea and lung function. This study only involved 17 patients and future larger trials of home NIV in COPD may need to include higher inspiratory pressures with careful monitoring of any potential side effects such as pneumothorax.
See page 303
Social inequalities in lung cancer
Prognosis of lung cancer is related to early diagnosis and access to surgery. In this issue, Anders and colleagues describe a population-based cohort study using the Regional Lung Cancer Register in Central Sweden to examine associations between socioeconomic status and management and survival in patients diagnosed with non-small cell lung cancer (NSCLC). The results show a higher diagnostic intensity in patients with high compared with low education and social gradients were seen in time between referral and diagnosis in early stage disease. After adjustment for prognostic factors, mortality in early stage disease was lower in women with a high education. The authors suggest that the reasons for these results may be different access to care, co-morbidity and lifestyle factors though we need to understand further the association between social inequality and management of lung cancer.
See page 327
Pulmonary blood flow in fibrotic lung disease
The prevalence of pulmonary hypertension in patients with fibrotic lung disease has been reported from 31 to 85% and is associated with clinical deterioration and mortality. Cardiac output is an important prognostic marker in pulmonary hypertension and proportional to pulmonary blood flow. In this issue Corte and colleagues report the use of a non-invasive assessment of pulmonary blood flow with the inert gas breathing Innocor device in normal subjects and those with fibrotic lung disease. They show good repeatability and reproducibility and suggest this technique can be used in clinical practice especially for monitoring disease progression and response to therapy.
See page 341
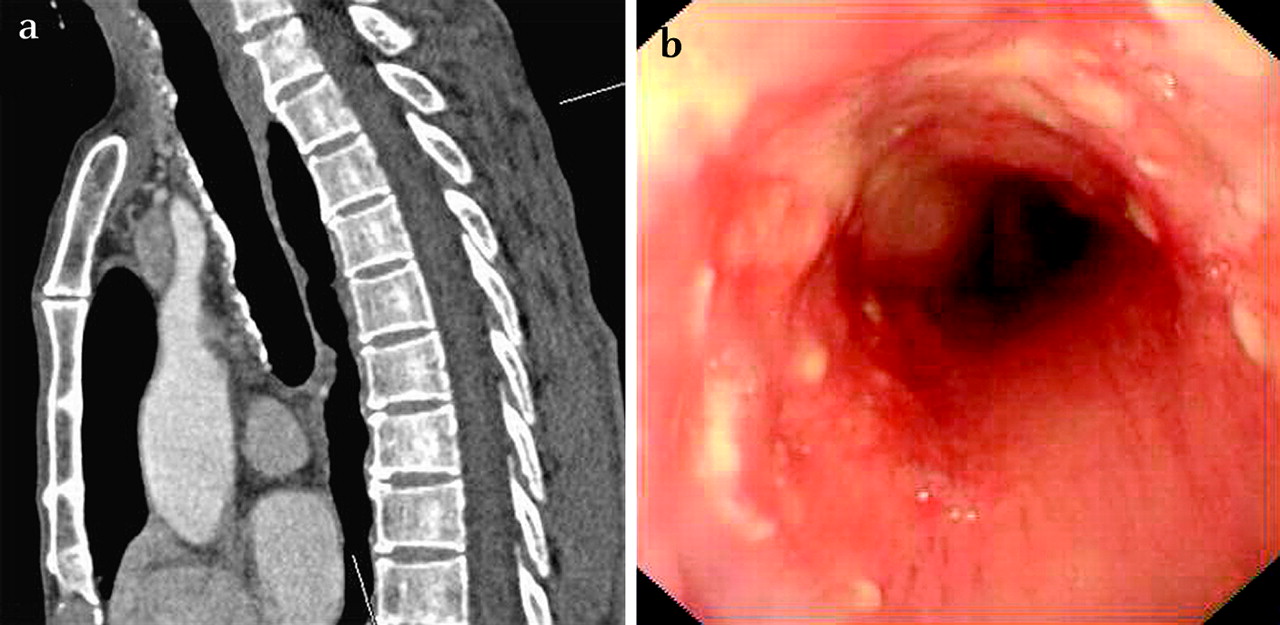
(a) Sagital section of CT thorax, (b) fibreoptic bronchoscopic view of trachea with sparing of nodularity posteriorly. See page 309.

Lung biopsy showing necrotising granulomatous inflammation and Histoplasma capsulatum. See Images in Thorax, page 372.

{kind=link}
{kind=link}
{kind=link}
Kaplane–Meier plot of time to recurrence of any strain of Pseudomonas aeruginosa in patients with cystic fibrosis treated with tobramycin inhalation solution twice daily (efficacy evaluable population). See page 288.
Linked Articles
- Editorial
- Lung cancer
- Images in Thorax
- Cystic fibrosis
- Pulmonary puzzle
- Interstitial lung disease
- Chronic obstructive pulmonary disease