Article Text

Abstract
Background A majority of patients with idiopathic pulmonary arterial hypertension (IPAH) display persistent exercise intolerance despite new specific therapies. Whether patients with IPAH exhibit peripheral muscle dysfunction that may contribute to this limitation remains unknown. The hypothesis that the muscles of patients with IPAH are weaker and display morphological changes compared with those of control subjects and that those changes partly correlate with their exercise capacity was tested.
Objective To characterise quadriceps function, morphology and the enzymatic profile of patients with IPAH.
Methods Exercise capacity, limb muscle cross-sectional area by CT scan, quadriceps strength by maximal voluntary contraction and non-volitional magnetic stimulation of the femoral nerve (quadriceps twitch; TWq), and muscle morphology and enzymatic profile by quadriceps biopsy of 10 patients with IPAH were compared with those of 10 matched controls subjects.
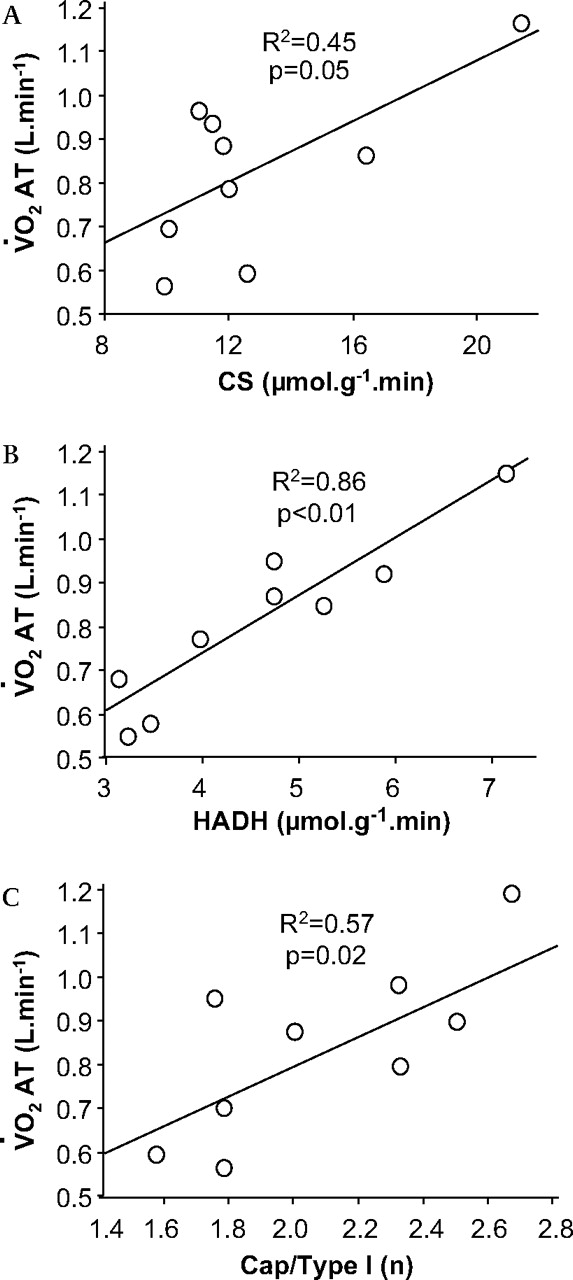
Results Patients with IPAH displayed a lower proportion of type I muscle fibres (p=0.05), a lower maximal voluntary contraction (p=0.05) and TWq (p=0.01), and an increased muscular phosphofructokinase/3-hydroxyacyl-CoA-dehydrogenase ratio (p=0.05). They also tended to have lower thigh muscle cross-sectional area (p=0.15). Maximal oxygen uptake correlated with quadriceps strength (R2=0.42, p=0.04), and oxygen uptake at anaerobic threshold correlated with muscle oxidative capacity assessed by oxidative enzyme level for citrate synthase (R2=0.45, p=0.05) and 3-hydroxyacyl-CoA-dehydrogenase (R2=0.86, p<0.01), and type I fibre capillarity (R2=0.57, p=0.02).
Conclusion Patients with IPAH present significant peripheral muscle changes that partly correlated with their exercise capacity.
- Hypertension pulmonary
- muscles skeletal
- exercise
- primary pulmonary hypertension
Statistics from Altmetric.com
Introduction
Idiopathic pulmonary arterial hypertension (IPAH) is characterised by the progressive increase in pulmonary vascular resistance ultimately leading to right heart failure and death. Until recently, the median survival in IPAH was <3 years.1 New specific therapies have considerably improved long-term prognosis of patients with IPAH, with recent studies describing a 3-year survival >80%.2 However, a majority of patients display persistent dyspnoea and significant exercise intolerance despite current treatments. Indeed, many patients remain in WHO functional class III, representative of marked exercise limitations and poor quality of life.3
This persisting exercise intolerance has been traditionally attributed to residual cardiac and respiratory impairment known to be involved in the exercise pathophysiology of IPAH.4 However, as for other respiratory and cardiac diseases,5 6 skeletal muscles abnormalities in IPAH may be implicated in the exercise limitation, leading to further worsening in functional status. This hypothesis has been reinforced by the recent description of respiratory7 and forearm8 muscle weakness in IPAH. Improvements in exercise capacity were also documented in patients with pulmonary hypertension undergoing pulmonary rehabilitation.9 The main objective of this study was to characterise the peripheral muscle function, morphology and enzymatic profile of patients with IPAH.
Methods
Study subjects
Ten WHO functional class II–III subjects with IPAH were recruited at our institution from February 2007 to March 2008. The IPAH diagnosis was made according to recent guidelines.10 All patients exhibited significant IPAH defined as a mean pulmonary artery pressure >25 mm Hg (range 29–69 mm Hg) at rest with a pulmonary capillary wedge pressure <15 mm Hg.11 Recent right heart catheterisation (<6 months) performed as part of their routine follow-up was used to described haemodynamic severity. Also, only patients with no change in their IPAH treatment and in stable clinical condition over the last 6 months were eligible. None of them had participated in a rehabilitation programme. Exclusion criteria were as follows: (1) recent syncope and WHO functional class IV; (2) left ventricular ejection fraction <40%; (3) significant restrictive (more than minimal lung fibrosis on CT scan or total lung capacity <70% of predicted) or obstructive (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) <70%) lung disease; (4) intrinsic musculoskeletal abnormality precluding exercise testing; and (5) patients with a pacemaker. Ten sedentary healthy subjects individually matched for age (within 5 years), gender, height (within 10 cm) and weight (within 5 kg) were recruited by advertisement in the community and tested concomitantly. The research protocol was approved by the institutional ethics committee, and both patients and control subjects gave written consent.
Study design
Measurements were performed by technicians blinded for the patients' condition and were completed during one visit to the laboratory.
Exercise capacity assessment
A 6 minute walk test and an incremental exercise test were performed according to the recent American Thoracic Society recommendations.12 13 Subjects were seated on an electrically braked ergocycle (Quinton Corival 400; A-H Robins, Seattle, Washington, USA) and were connected to the respiratory circuit through a mouthpiece (Quinton Qplex; A-H Robins, Bothel, Washington, USA). After 3 min of rest and 1 min of unloaded pedalling at a minimum rate of 60 rpm, a progressive ramp protocol was performed until exhaustion. Increments were adjusted subjectively from 5 to 20 W/min for a target exercise duration of 8–12 min. Five-breath averages of minute ventilation, O2 uptake and CO2 excretion were measured throughout the exercise.
Peripheral muscle morphology and enzymatic activity
Thigh muscle surface cross-sectional area
A CT of the dominant thigh halfway between the pubic symphysis and the inferior condyle of the femur was performed using a fourth-generation Toshiba Scanner 900S (Toshiba Inc., Tokyo, Japan).14 Each image was 5 mm thick and was taken at 120 kV and 200 mA with a scanning time of 1 s while the subject was lying in the supine position. The thigh muscle cross-sectional area was obtained by measuring the surface area of the tissue with a density of 35–100 Hounsfield units, corresponding to the density of muscle tissue.
Quadriceps biopsy
Percutaneous biopsy specimens of the vastus lateralis muscle of the non-dominant leg were taken at midthigh as described by Bergström.15 For the eight patients that were anticoagulated, oral anticoagulants were stopped 4 days before, and the international normalised ratio (INR) was measured prior to muscle biopsy, according to recent guidelines.21 After local anaesthesia, a 5–8 mm skin incision was made and muscle samples were obtained using one or two passes with the Bergström needle. The sample was immediately frozen in liquid nitrogen, embedded in optimum cutting temperature (OCT) compound (Tissue-Tek, Miles Inc, Elkhart, Indiana, USA), frozen in cooled isopentane and stored at −80°C. Transverse sections of 10 μm were cut using a cryostat Leica Jung CM 3000 (Wetzlar, Germany). Each section was verified by light microscopy to ensure proper fibre orientation.
Fibre typing
Muscle sections were stained to see myofibrillar adenosine triphosphatase activity according to the single-step modified ethanol technique.16 For each subject, the proportion of types I (non-stained), IIa (lightly stained) and IIx (darkly stained) fibres was assessed and was calculated as the number of fibres of each type divided by the total number of muscle fibres.
Fibre surface area and capillarity
The surface of 40 randomly selected fibres of each type was measured and averaged for each fibre type.17 Muscle sections were stained with the α-amylase–periodic acid–Schiff method to visualise capillaries.18 Muscle capillarity was expressed by dividing the number of capillaries in direct contact with the outer fibre membrane by the number of fibres.
Enzymatic activity
Quadriceps muscle activity of citrate synthase (CS; EC 4.1.3.7), 3-hydroxyacyl-CoA-dehydrogenase (HADH; EC 1.1.1.3) and phosphofructokinase (PFK; EC 2.7.1.11) was assessed using the spectrophotometric technique.19 Discriminating enzyme ratios representing glycolysis to the citric acid cycle (PFK/CS) and the β-oxidation of fatty acids (PFK/HADH) were assessed.20
Quadriceps muscle strength
Both non-volitional and volitional strength of the quadriceps was evaluated by a modified technique developed by Polkey et al,22 adapted in our laboratory by Saey et al.23 In the recumbent position (N-K 330 Exercise Table, N-K Products, Elsinore California, USA), the dominant leg was stabilised with the knee flexed at 90°. The ankle was attached to a strain gauge (Hewlett-Packard, Palo Alto, California, USA) through a non-elastic strap to measure isometric knee extension tension. Care was taken to ensure that the ankle strap and transducer were perpendicular to the leg and the chair frame, and that the standard position was kept identical throughout the protocol. During maximal voluntary contraction (MVC), patients maintained the highest isometric strength possible for 3 s. Verbal encouragement was provided throughout these manoeuvres. The signal obtained was amplified (8811A amplificator, Hewlett-Packard), then transformed by an analogue transducer (Biopac system, Santa Barbara, California, USA) connected to a computer for further data analysis (Acknowledge software, Biopac). Non-volitional strength of the quadriceps was measured using two commercial magnetic stimulators both related by a BiStim (Magstim, Whitland, Dyfed, UK). A 70 mm figure-of-eight coil was positioned over the femoral nerve at the position leading to the strongest muscle contraction. Because potentiated twitches (quadriceps twitch (TWq)) are more accurate,24 TWq were obtained at 100% stimulator output 3 s after MVC manoeuvres. Three sets of MVC and TWq measurements were performed, separated by a 1 min resting period. In the case of a variability of >5%, additional measurements were performed until the reproducibility criterion was met. Reported values for the MVC and TWq were the mean of the three strongest contractions.
Statistical methods
Values are reported as median (IQR) unless otherwise specified. Comparisons between groups were performed using Mann–Whitney U test. The categorical variable was analysed using the Fisher exact test. Based on normal TWq described in healthy subjects 25 and patients with other chronic respiratory diseases,6 we estimated that TWq would average 6.0 (2.0) kg in IPAH compared with 8.5 (2.0) kg for controls (primary outcome). Thus, we determined a priori that 10 patients with IPAH and 10 controls would be necessary to detect a statistically significant difference in TWq with a type I error of 5% and a type II error of 20%. Pearson correlation coefficients were used to evaluate relationships between exercise capacity and quadriceps strength. Because the anaerobic threshold is representative of the oxidative capacity, correlations between the oxygen uptake at anaerobic threshold and markers of muscle aerobic characteristics (type I fibre proportion, capillarity, oxidative enzyme profile) were also assessed. A p value <0.05 was considered statistically significant. Data were analysed using Statview V.5.0.
Results
Subjects' characteristics
The characteristics of the study population are shown in table 1.
Characteristics of the study population
Patients with IPAH and controls were well matched for age, gender and body mass index. Pulmonary function tests were also comparable except for the diffusing capacity of carbon monoxide (DLCO; 67 (25) % vs 89 (10) % of predicted, p=0.03). All patients with IPAH displayed significant resting pulmonary hypertension and marked exercise intolerance. At the time of the study, mean symptom duration was 55 (29) months and all patients were in WHO functional III at the time of diagnosis. They had been treated for 35 (22) months with bosentan (n=6), sildenafil (n=1), calcium channel blockers (n=1) or epoprostenol (n=2). Seven patients were now classified as WHO functional class II, whereas three patients were in WHO functional class III.
Quadriceps muscle morphology and enzymatic activity (table 2)
Compared with controls, patients with IPAH displayed a lower proportion of type I fibres and a higher overall proportion of type II fibres (p=0.05). Analysis of the type II fibres showed that the IIx fibres were responsible for the increase in the percentage of the type II fibres, although this did not reach statistical significance. Discriminating enzyme ratios revealed a higher PFK/HADH ratio, compatible with a relatively higher potential for anaerobic than for aerobic energy metabolism.
Peripheral muscle characteristics of the study population
Quadriceps muscle function
MVC (36 (10) kg vs 44 (7) kg, p=0.05) and TWq (6.8 (2.1) kg vs 9.4 (2.2) kg, p=0.01) were significantly lower in patients with IPAH (figure 1A). No difference was found when the quadriceps strength was normalised for thigh muscle cross-sectional area (0.49 (0.11) kg/cm2 vs 0.50 (0.06) kg/cm2, p=0.85). MVC moderately correlated with thigh muscle cross-sectional area (R2=0.26; p=0.02).

(A) Non-volitional and voluntary strength of the dominant quadriceps in patients with idiopathic pulmonary arterial hypertension (white bars) and matched sedentary controls (black bars). (B) Correlation between non-volitional strength of the quadriceps and maximal exercise capacity in idiopathic pulmonary arterial hypertension. Twq, strength assessed by magnetic stimulation of the femoral nerve; MVC, maximal voluntary contraction; V̇O2max, maximal oxygen uptake.
Correlates of peripheral muscle function in IPAH
Among patients with IPAH, exercise capacity positively correlated with quadriceps strength (figure 1B). Oxygen uptake at the anaerobic threshold also positively correlated with the quadriceps oxidative characteristics assessed by two oxidative enzymes (CS and HADH) as well as with the capillaries/type I fibre ratio (figure 2). Exploratory analyses suggested a negative correlation between disease duration and the proportion of type I fibre (R2=0.45; p=0.03). Conversely, there was no correlation between maximal exercise capacity, the proportion of fibre types, muscle surface area, activity of oxidative and glycolytic enzymes, muscle strength and any pulmonary haemodynamic parameters at rest.

{kind=link}
{kind=link}
Correlation between oxygen uptake at anaerobic threshold and muscular morphology in patients with idiopathic pulmonary arterial hypertension and (A) citrate synthase (CS) level, (B) 3-hydroxyacyl-CoA-dehydrogenase (HADH) level and (C) capillaries/type I fibre ratio (Cap/Type 1). The anaerobic threshold could not be determined in one patient. V̇O2 AT, oxygen uptake at the anaerobic threshold.
Discussion
The present study documented significant morphological and functional quadriceps changes in IPAH including a lower proportion of type I fibres, a higher PFK/HADH ratio compatible with a relatively higher potential for anaerobic than for aerobic energy metabolism, as well as lower quadriceps strength. Non-volitional quadriceps strength correlated with maximal oxygen uptake, whereas quadriceps aerobic characteristics correlated with the anaerobic threshold. Importantly, muscle characteristics were unrelated to the haemodynamic severity of IPAH. These observations suggest that peripheral muscle abnormalities may be implicated in the exercise pathophysiology of IPAH.
In IPAH, exercise pathophysiology is characterised by a disproportionate increase in pulmonary artery pressure, low stroke volume and chronotropic response, and ventilation–perfusion mismatch.26 These abnormalities presumably translate into low maximal oxygen uptake and oxygen pulse, early anaerobic threshold, excessive ventilation and exercise-induced hypoxaemia.4 Because baseline exercise capacity4 26 or changes in exercise tolerance over time26 27 only partly correlate with resting pulmonary haemodynamics in IPAH, others factors may contribute to exercise limitation in IPAH. More recently, respiratory and forearm muscle weakness were described in IPAH.7 8 Interestingly, muscle weakness was independent of haemodynamic severity. Forearm strength also correlated with respiratory muscle strength and exercise capacity.8 However, only volitional strength was assessed in these studies, and thus the validity of these observations was questioned.28 The present study confirmed that lower limb muscles are functionally abnormal in IPAH, as evaluated by both volitional and non-volitional measurements. Moreover, muscle strength and quadriceps oxidative properties correlated with exercise capacity and anaerobic threshold, respectively, whereas muscle characteristics did not correlate with the haemodynamic severity of IPAH. This could be explained by the influence of muscle function on the perception of leg effort during exercise, which is the main limiting symptom in a significant proportion of patients with IPAH.4 Whether the functional improvement previously observed following pulmonary rehabilitation was related to changes in peripheral muscle function remains to be explored.9
These observations are consistent with the peripheral muscle abnormalities previously described in patients with congestive left heart failure and chronic obstructive pulmonary disease (COPD) that include quadriceps muscle atrophy and weakness, relative increase in easily fatiguable type IIx fibres, relative decrease in oxidative type I fibres, decreased oxidative enzymes and mitochondria, abnormal intracellular calcium profiles, slower restoration of muscle phosphocreatine stores after exercise and an increased lactate accumulation during exercise.5 6 These muscle abnormalities also correlate with maximal exercise capacity, but are discrepant with the traditional marker of disease severity.5 6 Nevertheless, patients with IPAH differ markedly from patients with congestive left heart failure and COPD: they are much younger and the disease duration is much shorter. Interestingly, the proportion of type I fibres negatively correlated with disease duration. Thus, one could not extrapolate data from other chronic cardiac and respiratory diseases to IPAH. Importantly, the observation that muscle abnormalities are a common final scenario of several chronic conditions suggests some similarities in the underlying mechanisms. The investigation of various disease models may thus help in determining unifying mechanistic mechanisms involved in this dysfunction. Those may include the presence of systemic and/or local inflammation,29 low cardiac output and hypoxaemia leading to impaired peripheral oxygen delivery,1 sympathetic hyperactivity30 and deconditioning. Whether other factors such as endothelial dysfunction or interaction with molecules targeting the endothelin-1 and nitric oxide signalling pathways potentially influence vascular responsiveness of skeletal muscle arterioles in IPAH remains unknown.31 32
The limitations of our study should be discussed. First, the proposed protocol was physically demanding and potentially led to some selection bias towards patients less severely impaired. Thus, our results may not be representative of peripheral abnormalities that would have been observed in the most severe patients and may have decreased the magnitude of differences in peripheral muscle characteristics between patients with IPAH and healthy subjects. Furthermore, close correlations between muscle characteristics and exercise capacity do not imply causal relationships. Similarly, differences in muscle performance between groups were modest in comparison with the substantial differences in aerobic capacity. This suggests that muscle dysfunction, while potentially contributing to exercise intolerance, is unlikely to be the main limiting factor. Importantly, our limited sample size may have led to type I and type II errors, especially for secondary endpoints. However, the alterations in muscle characteristics observed in our study were of similar magnitude to those in COPD in which peripheral myopathy is clearly implicated in patients' functional impairment. Further studies are also needed in the more heterogeneous population of patients with non-IPAH, in whom the primary disease could independently influence muscle characteristics. Finally, our study design precluded the analysis of whether PAH-specific treatment influenced skeletal muscle function, morphology, enzyme activities and vascularisation.
Conclusion
The present study documented significant morphological and functional changes in the quadriceps of patients with IPAH. Some of these abnormalities correlated with patients' functional status. Whether improving peripheral muscle integrity will enhance functional status and quality of life in IPAH remains to be confirmed.
Acknowledgments
The authors would like to thank Annie Michaud, Louis Laviolette and Éric Nadreau for their technical assistance, Serge Simard for his statistical assistance, and the “Banque de tissue du Réseau en Santé Respiratoire du FRSQ, site de l'Institut Universitaire de Cardiologie et de Pneumologie de Quebec”.
References
Footnotes
See Editorial, p97
Linked articles 120824.
SP is a clinical scientist of the Fonds de Recherche en Santé du Québec and FM is a research scholar of the Fonds de la Recherche en Santé du Québec.
Funding Réseau en Santé Respiratoire du Fonds de Recherche en Santé du Québec and the Groupe de recherche en santé respiratoire de l'Université Laval (GESER).
Competing interests None.
Ethics approval The research protocol was approved by the institutional ethics committee.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.