Article Text

Abstract
Objective To determine the prevalence and risk factors of obstructive sleep apnoea syndrome (OSAS) in Chinese children using a two-phase community-based study design.
Methods Children from 13 primary schools were randomly recruited. A validated OSAS screening questionnaire was completed by their parents. Children at high risk of OSAS and a randomly chosen low-risk group were invited to undergo overnight polysomnographic study and clinical examination. The the sex-specific prevalence rate was measured using different cutoffs (obstructive apnoea hypopnoea index ≥1, ≥1.5, ≥3 and ≥5 and obstructive apnoea index ≥5) and risk factors associated with OSAS were evaluated with logistic regression.
Results 6447 completed questionnaires were returned (out of 9172 questionnaires; 70.3%). 586 children (9.1%; 405 boys and 181 girls) children belonged to the high-risk group. A total of 619 (410 and 209 from the high and low-risk group, respectively) subjects underwent overnight polysomnagraphy. Depending on the cutoffs, the prevalence rate of childhood OSAS varied from 4.8% to 40.3%. Using the International Criteria of Sleep Disorders version II, the OSAS prevalence for boys and girls was 5.8% and 3.8%, respectively. Male gender, body mass index z-score and increased adenoid and tonsil size were independently associated with OSAS.
Conclusions The prevalence rate of OSAS in children was contingent on the cutoff used. The inclusion of symptoms as a part of the diagnostic criteria greatly reduced the prevalence. A further prospective and outcome study is needed to define a clinically significant diagnostic cutoff for childhood OSAS.
- Epidemiology
- childhood OSAS
- community study
- sleep apnoea
Statistics from Altmetric.com
Childhood obstructive sleep apnoea syndrome (OSAS) is a sleep-related breathing disorder characterised by intermittent upper airway obstruction that disrupts normal ventilation and sleep patterns.1 Increasing evidence suggests that childhood OSAS is an important public health problem. Children with OSAS have higher respiratory disease-related morbidity and healthcare utilisation starting from the first year of life until the date of diagnosis.2 If left untreated, the condition is associated with cardiovascular and neurocognitive consequences with significant long-term clinical implications.3–8
The reported prevalence of childhood OSAS varied from 0.1% to 13%.9 The wide range of prevalence rate was mostly related to methodological issues, including lack of polysomnographic confirmation, different sampling strategies, small sample size and the different diagnostic threshold used for defining childhood OSAS. In addition, there is a suggestion of ethnic difference in the prevalence of OSAS, with African-American children having a higher prevalence compared with white children in the USA.10 11 In a recent review, the authors commented that additional work in childhood OSAS epidemiology is needed and standardisation of selection and diagnostic criteria across studies would be helpful in future cross-ethnic comparisons.9 The ascertainment of a reliable and accurate prevalence of childhood OSAS will allow for better healthcare planning, resource allocation and future comparison of data.
The objective of this study was to determine the prevalence of OSAS in Chinese children aged between 5 and 13 years in the general population, thus reducing the potential selection biases introduced by recruiting hospital attendants. The study had a two-phase design; the first phase involved completion of a validated screening questionnaire by parents of randomly selected subjects. Subjects at high risk of OSAS together with a control group then underwent detailed clinical examination, upper airway assessment and overnight sleep study for confirmation of their OSAS status.
Materials and methods
Study population
Based on our pilot study, the prevalence of OSAS in local healthy children was not greater than 4.5%,12 A sample size of 6600 would be needed to allow an estimate of OSAS prevalence with a precision of 0.5% and 95% confidence. We recruited subjects from two school districts; Shatin and Tai Po. The two districts had similar social class and income distribution to the rest of the territory, thus the results obtained from this study would be a true representation of Hong Kong (http://www.censtatd.gov.hk/hong_kong_statistics/statistical_tables). There were 76 primary schools in the two districts. Selection of a school was based on computer-generated random numbers, and if the selected school declined to participate, the next randomly selected school was invited. Thirteen primary schools in the two districts were randomly chosen to participate in this study. In each school, two randomly chosen classes from each grade were invited to participate. The number of subjects recruited from this sampling frame would guarantee that the required sample size was obtained. Approval by the ethics committee of the Chinese University of Hong Kong was obtained.
First phase
All parents of children in the randomly selected schools were invited to attend an education forum during which full explanation of the purpose and flow of the study was given. An envelope containing a validated parent proxy OSAS screening questionnaire13 and consent was then distributed to parents within a week after the forum. The parents were asked to return the completed questionnaire within a week. For those who failed to return the questionnaire, another copy was given with a self-addressed envelope enclosed for ease of return.
The 54-item questionnaire (HK-CSQ) sought information regarding sleep habits and problems including nocturnal OSAS symptoms (snoring, witnessed apnoea, laboured breathing and oral breathing), parasomniac symptoms (presence and frequency of nocturnal enuresis, night terrors, nightmares, somnambulism, sleep talking and bruxism) and daytime symptoms (morning headache, recurrent upper airway infections, daytime sleepiness in different situations and hyperactivity). In addition, the following information was also obtained: body height and weight, history of allergic rhinitis and asthma, exposure to cigarette smoke, home living environment, family income, number of household members and parental education.
Data from three survey questions, namely snoring, nocturnal mouth breathing and night sweating, answered by a five-point frequency scale (0=‘never’; 1=‘rarely’ for 0–1 nights per month; 2=‘sometimes’ for 1–2 nights per month, 3=‘often’ for 1–2 nights per week; 4=‘frequently’ for 3 nights or more per week) and a ‘do not know’ category were used to classify survey participants as having a high or low risk of OSAS. From our previous research, a composite symptom score (summation of the scores of these three questions) of 7 or more has 75.4% sensitivity and 80.5% specificity, compared with polysomnography, to detect OSAS among children aged 5–15 years who had attended our paediatric clinics.13 Children with a composite symptom score of less than 7 were assigned a computer-generated random number and were invited as a control group with a ratio of 1:2 in the second phase.
All children belonging to the high risk of OSAS group and the randomly selected subjects at low risk of OSAS were invited to undergo examination by an otorhinolaryngologist and overnight polysomnographic study. Children were excluded from the study if they had intercurrent illness within 4 weeks of the polysomnographic study, or if they were reported by their parents to have cardiac, renal or neuromuscular diseases or chromosomal abnormalities, or if they had previously undergone upper airway surgery.
Second phase: polysomnography
A single attended overnight polysomnography was performed in a dedicated sleep laboratory with a CNS 1000P polygraph (CNS, Inc, Chanhassen, Minnesota, USA) as described in our previous publication.4 5 15 All computerised sleep data were further manually edited by experienced polysomnography technologists and clinicians according to standardised criteria.15 An obstructive apnoea was defined as the absence of airflow with persistent respiratory effort lasting longer than two baseline breaths, irrespective of arterial oxygen saturation changes. A mixed apnoea was defined as the absence of airflow for a duration of at least two breath cycles without inspiratory effort in the initial portion of the event, followed by resumption of inspiratory effort in the second portion of the event. An obstructive hypopnoea was defined as a reduction of 50% or more in the amplitude of the airflow signal with persistent respiratory effort. It was only quantified if it was longer than two baseline breaths and was associated with oxygen desaturation of at least 4% and/or arousals. The obstructive apnoea index (OAI) was defined as the number of obstructive apnoeas and mixed apnoeas per hour of sleep. The obstructive apnoea hypopnoea index (OAHI) was defined as the total number of obstructive apnoeas, mixed apnoeas and obstructive hypopnoeas per hour of sleep. All computerised sleep data were manually edited by experienced polysomnography technologists and clinicians according to standardised criteria.16 A successful polysomnography study was defined as total sleep time of over 6 h and a sleep efficiency (total sleep time/time in bed ×100%) of over 70%.
Childhood OSAS was defined by using different diagnostic criteria: OAHI ≥1, ≥1.5, ≥3, ≥5, OAI ≥1 and International Criteria of Sleep Disorders version II (ICSD-II) criteria (OAHI ≥1 plus habitual snoring plus at least one more OSAS-related symptom).17 Habitual snoring was defined as parental report of snoring for at least 3 nights a week in the past 12 months. OSAS-related symptoms included night sweating, nocturnal enuresis, morning headaches, daytime tiredness and restless sleep. These cutoffs are widely used to describe childhood OSAS, but it is not well standardised in children18, and the clinical importance of any particular cutoff is still undetermined. Although in our experiences an apnoea hypopnoea index of 5 or greater correlated best with cardiovascular outcome in cross-sectional studies.4 5
Clinical examination
Standing height (in metres) without shoes was measured using a Harpenden stadiometer (Holtain, UK) to the nearest 0.1 cm. Body weight (in kg) was measured with the lightest clothing to the nearest 0.1 kg by an electronic weighing scale (Seca model 708; Vogel & Halke GmbH & Co, Hamburg, Germany). Body mass index was calculated as kg/m2 and converted to a z score according to local reference.19 Overweight and obese children were defined as a body mass index z score greater than 1.036 and 1.645, corresponding to the 85th and 95th percentile (relative to age and gender), respectively. Each child also underwent physical examination by an experienced paediatrician (AML) before polysomnographic study.
Upper airway examination
The size of tonsils and adenoids was measured by endoscopic examination by means of a flexible fibrescope (Olympus 3 mm; Olympus, Japan). The examination was performed by an otorhinolaryngologist who was blinded to the group allocation and polysomnographic result of the subjects. The examination was carried out in the morning after overnight polysomnographic study. Tonsil size was reported as a percentage of the oropharyngeal airway while adenoid size was assessed as a percentage of the nasopharyngeal airway.
Statistics
The distributions of all the continuous data for parametric analyses were confirmed to be normal by normal probability plot (Q–Q plot). Continuous data were expressed as means (SD) while categorical data were expressed as percentages. Student's t test and the χ2 test were used for comparisons of continuous data and categorical data, respectively. The weighted prevalence of OSAS based on different diagnostic criteria was calculated. Logistic regression analyses were performed to assess the association between potential risk factors and childhood OSAS as defined by OAHI of 5 or greater or ICSD-II criteria. The association was first assessed in a univariate model and then in a multivariate model constructed by forward selection (likelihood ratio) method. SPSS for Windows 14 was used in the analysis, and the level of significance was set at 5% for all comparisons.
Results
A total of 9172 students was invited to participate. Six thousand four hundred and forty-seven completed questionnaires were returned and scored (response rate 70.3%). The demographic, socioeconomic and sleep symptoms data of the questionnaire respondents according to gender are shown in table 1.
Demographic and socioeconomic characteristics of the respondents
Five hundred and ninety-one (9.2%; 410 boys) children had a composite score of 7 or greater, of whom 410 (70%; 288 boys) agreed to take part in the second phase of our study. A comparison of demographic and socioeconomic data between subjects with a composite score of 7 or greater who agreed to undergo overnight polysomnography and those who refused did not reveal any significant differences (table 2). Six hundred and eighteen subjects (out of 5856) from the low-risk group (composite score <7) were approached and finally 209 (108 boys) agreed to participate in the second phase. Their baseline characteristics did not have significant differences compared with those with a composite score of less than 7, but were not selected to participate in the second phase (table 2). A total of 619 children underwent overnight polysomnography to ascertain their OSAS status, and polysomnography was successful in all cases. None of the subjects had cardiopulmonary abnormalities detected on clinical examination. No significant gender differences were found in age, body size, total sleep time and sleep efficiency. Boys had a significantly greater proportion of sleep stage 1 (7.5±4.0 vs 6.8±3.3%, p=0.018) but less sleep stage 2 (47.8±5.6 vs 49.4±5.2, p=0.002). They also had significantly higher OAHI (0.9 (0.1 to 2.5) vs 0.4 (0 to 1.2), p<0.001), OAI (0.4 (0 to 1.3) vs 0.2 (0 to 0.6), p<0.001), arousal index (6.8 (5.1 to 8.8) vs 6.1 (4.8 to 8.0), p=0.017) and lower arterial oxygen saturation nadir (91.6±3.4 vs 92.4±2.9, p=0.008) compared with girls. Furthermore, boys had a greater prevalence of nocturnal sweating (46.7 vs 30.0%, p<0.0001) and snoring (60.4 vs 51.6%, p=0.035) compared with girls.
Characteristics of subjects with and without polysomnography
Two hundred and sixty-six (194 boys), 197 (150 boys), 102 (80 boys) and 67 children (52 boys) were found to have OAHI of 1 or greater, 1.5 or greater, 3 or greater and 5 or greater, respectively. One hundred and fifty-two children (115 boys) were found to have OAI of 1 or greater. Table 3 shows the prevalence of OSAS symptoms in children with OSAS according to different diagnostic cutoffs.
Distribution of symptoms in children with OSAS by different diagnostic cutoffs
Weighted prevalence of childhood OSAS based on different diagnostic criteria
The mean composite score of the three survey questions of subjects belonging to the low-risk group was 1.94 (SD 1.89). The mean composite score of the 209 subjects was 3.55 (SD 2.05). In order to allow for a more reliable and accurate calculation of a weighted prevalence, the 209 subjects were further subdivided into those with composite scores less than 4 (low-low risk) and those with a score between 4 or greater and less than 7 (low risk).
The weighted prevalence of OSAS based on different diagnostic criteria was calculated using the following equation:
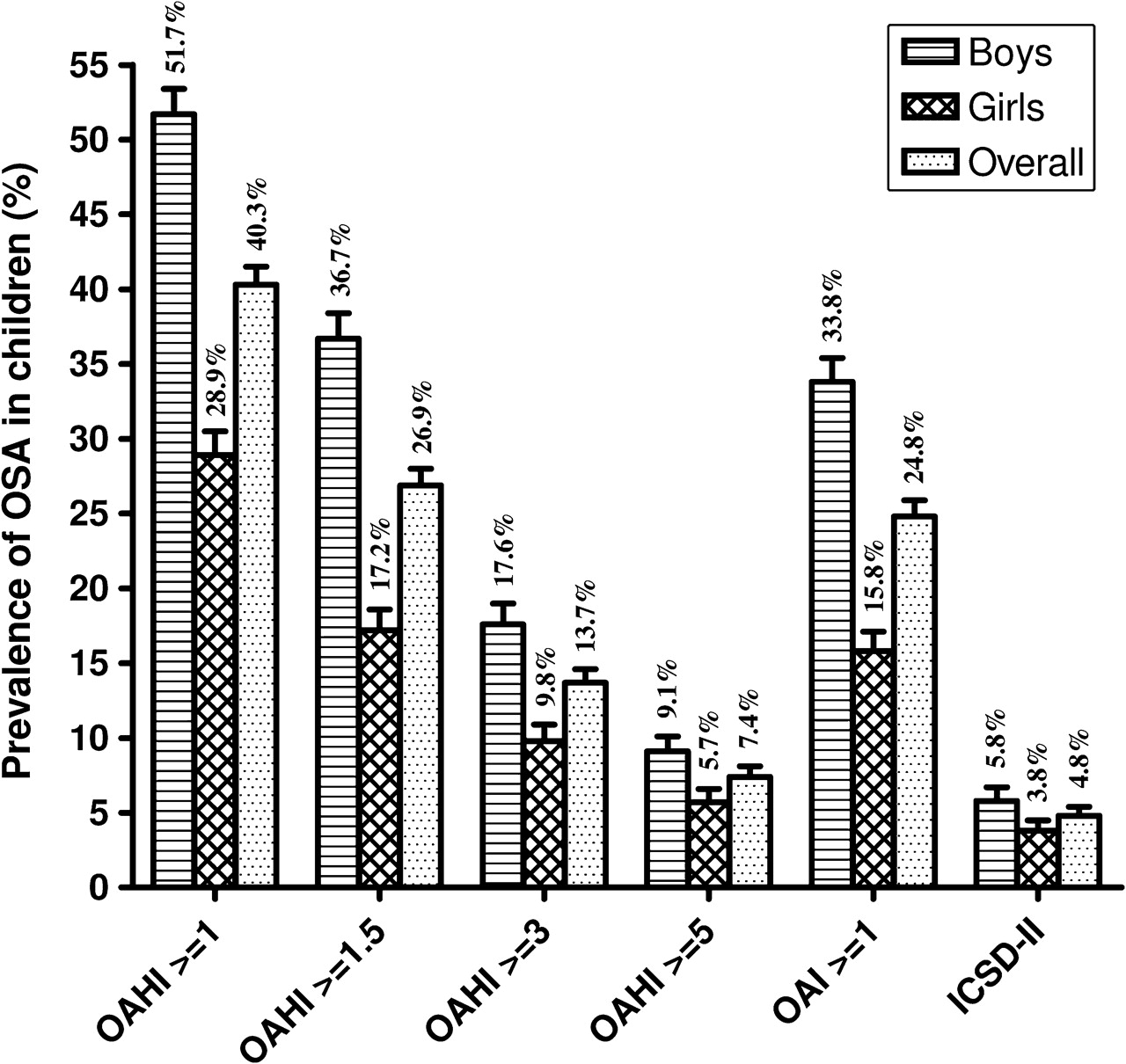
The gender-specific and overall weighted prevalence of OSAS according to various diagnostic cutoffs are presented in figure 1. Boys had a higher prevalence of OSAS than girls. The overall weighted prevalence varied from 4.8% to 40.3% depending on the cutoff chosen. Using ICSD-II recommendations, the OSAS prevalence (95% CI) for boys, girls and overall was 5.8% (5.1 to 6.7), 3.8% (3.2 to 4.5) and 4.8% (4.3 to 5.4), respectively.

{kind=link}
Weighted prevalence of obstructive sleep apnoea (OSA) in children by gender and different diagnostic cutoffs. The error bars depicted the upper limit of the 95% CI of the prevalence. ICSD-II, International Criteria of Sleep Disorders version II; OAHI, obstructive apnoea hypopnoea index.
Risk factors associated with OSAS
On multiple logistic regression analysis male gender, obesity and tonsil size were independently associated with OSAS using OAHI of 5 or greater as the cutoff. Whereas using ICSD-II criteria, obesity, the composite symptom score and tonsil size were significantly associated with a diagnosis of OSAS (table 4).
Factors associated with childhood OSAS defined as OAHI of 5 or greater or ICSD-II criteria*
Discussion
To the best of our knowledge, this is the first prevalence study that used a two-phase design with laboratory confirmation of OSAS in a large population-based sample of Chinese children. OSAS, as defined by the latest ISCD-II guidelines, is prevalent among both boys and girls aged between 5 and 13 years, the rates are 5.8% and 3.8%, respectively.
The criteria for diagnosing childhood OSAS have not been standardised, and the different cutoffs used could explain the wide range of prevalence rates reported in the literature.9 16 Although these cutoffs are statistically abnormal, their validity as predictors of long-term outcome has not been established.18 A few studies have chosen to use an apnoea hypopnoea index of 5 or greater as a clinically relevant cutoff.4 5 19 20 The need to include the presence of symptoms in diagnosing OSAS is another issue that needs to be clarified. The latest ICSD-II guidelines require the presence of habitual snoring plus one other OSAS symptom together with an OAHI of 1 or greater as diagnostic for childhood OSAS.17 In adults, OSAS is defined as OAHI of 5 or greater in conjunction with hypersomnolence or related problems in daytime function.21 The necessity of daytime complaints to be included in the definition of OSAS in adults has recently been challenged. The milestone OSAS epidemiological study from the Wisconsin Sleep cohort reported a minimal prevalence rate of 2% and 4% for men and women. The rate would inflate to 9% and 24%, respectively, when symptoms were excluded in the definition.21 The 18-year mortality follow-up from the same cohort showed that untreated subjects with a high apnoea hypopnoea index at baseline were at increased risk of cardiovascular mortality, irrespective of symptoms of sleepiness.22 A more recent article also provided similar evidence that non-sleepy OSAS adults were exposed to increased cardiovascular risk.23 In our study, when the necessity of symptoms was not included in the definition, the overall prevalence ranged from 7.4% to 40.3% depending on the OAHI/OAI cutoff one uses. Even adopting a rather conservative threshold of OAHI of 5 or greater, the prevalence of OSAS in boys and girls remains at 9.1% and 5.7%, respectively. Could this high rate of asymptomatic subjects with significant OAHI levels be due to sampling and design error? The relatively large proportion of subjects reported to have symptoms of allergic rhinitis might explain the high rate of OSAS in this group of children. However, the multivariate logistic regression results revealed that the presence of allergic rhinitis was not associated with the presence of OSAS as defined by OAHI of 5 or greater or ICSD-II criteria. In fact, the strength of our current study lay in the inclusion of subjects at low risk of OSAS, who were supposed to be free of any significant OSAS symptoms. In other words, most of the epidemiological studies that were based on reported symptoms,24–26 or polysomnographic confirmation in selected subjects11 27 28 would grossly underestimate the true OSAS prevalence by excluding asymptomatic subjects. Indeed, as demonstrated in our study, snoring that has been labelled as the cardinal symptom of OSAS1 was reported at most by approximately 80% of the subjects.
Our calculated prevalence for childhood OSAS was higher than the commonly reported figure of between 1% and 3%. The use of different diagnostic criteria in defining OSAS can explain this discrepancy and thus it is necessary to standardise the diagnostic cutoff to allow for more meaningful interracial comparison. One previous study examined the prevalence of OSAS among Chinese children with a mean age of 6.2 years.29 The study recruited hospital attendants, which greatly limited its application to the general population. In addition, it had a small sample size of 200 subjects and only 55% of suitable children, those reported to have habitual snoring, underwent overnight polysomnography. The study reported a prevalence rate of 0.1%, but this is likely to be an inaccurate estimation as a result of its unsatisfactory study design.
Previous studies reported that there were no gender differences in the prevalence of childhood OSAS.28 30 In contrast, our study consistently demonstrated that boys outnumbered girls in the prevalence of OSAS across all diagnostic criteria. Male gender was found to be an independent factor associated with OSAS in multiple regression analysis. A higher prevalence of atopy and especially allergic rhinitis among the boys may explain this gender difference. There is robust evidence to suggest allergic rhinitis increases the risk of OSAS in children, and treatment of allergic rhinitis could possibly prevent the onset of OSAS and reduce the severity of existing OSAS.31 Obesity is another important factor to account for the gender difference in OSAS prevalence. Boys are heavier than their female counterparts at all ages between 6 and 18 years.32
There are certain limitations in our study. First, we only achieved a 70% response rate to our questionnaire survey. This was compensated for by the large number of subjects (70% of high risk of OSAS subjects and a large sample of subjects at low risk of OSAS) undergoing overnight polysomnography to ascertain their OSAS status. Furthermore, this was a population-based study, therefore minimising any potential biases inherent in hospital-based subjects. Second, the ability of a single-night polysomnographic study to represent usual sleep has been questioned.33 34 The first night effect would influence sleep patterns and architecture and thus the reliability of a single night recording. Our previous research work, however, has demonstrated that a single night polysomnographic study could detect obstructive sleep apnoea in children in nearly 85% of cases.14 Third, our OSAS questionnaire had a sensitivity of approximately 80%, thus a proportion of genuine OSAS cases would have been missed in the initial screening phase. This deficit was partly overcome by including a reasonably large sample of subjects screened to be at low risk of OSAS to undergo polysomnography, thus allowing a weighted prevalence to be calculated. Despite our intensive effort and careful design, there is no doubt that a self-selected bias existed in the second phase. This could not have been completely prevented as parents were more likely to agree to take part in this study if they thought their child had a sleep problem, although the symptoms were mild and infrequent (thus had low scores). Nonetheless, we tried to rectify this bias by further weighting of the prevalence rates.
In conclusion, the present study estimated the prevalence of OSAS in Chinese children and the rates vary according to the diagnostic criteria used. Further research is needed to determine the level of apnoea hypopnoea index that is clinically significant as the prevalence of OSAS hinges on this important cutoff.
Acknowledgments
The authors would like to thank all the staff of the Sleep Assessment Unit of Shatin Hospital for logistic support, and the schools, children and their parents for their cooperation and participation.
References
Footnotes
Funding This study was funded by grant CUHK4161/02M from the Research Grants Council of the Hong Kong SAR, China.
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committee of the Chinese University of Hong Kong.
Provenance and peer review Not commissioned; externally peer reviewed.