Article Text

Statistics from Altmetric.com
Pandemic influenza A (H1N1) is a major global public health concern.1 We report an outbreak of H1N1 influenza involving clinical staff and patients in a teaching hospital in the North East of Scotland.
In October 2009, a teenage patient was admitted with an exacerbation of asthma. As there was no reason to suspect H1N1, the patient was not isolated. However, nose and throat swabs were in fact taken on the day of admission and were positive for H1N1 by PCR within 24 h. At this point, source isolation precautions were instituted. Seven otherwise healthy clinical staff in our department (6 doctors and 1 nurse; mean age 29, three males) subsequently developed typical symptoms within the next 9 days. Cases were confirmed by viral PCR from pooled nasal and throat samples. As H1N1 was common in the community at this time, it was not possible to determine whether the patient was the source of infection; however, five of the affected clinical staff had been in direct contact with the patient and the first symptoms reported by them were 48 h following his admission to the ward.
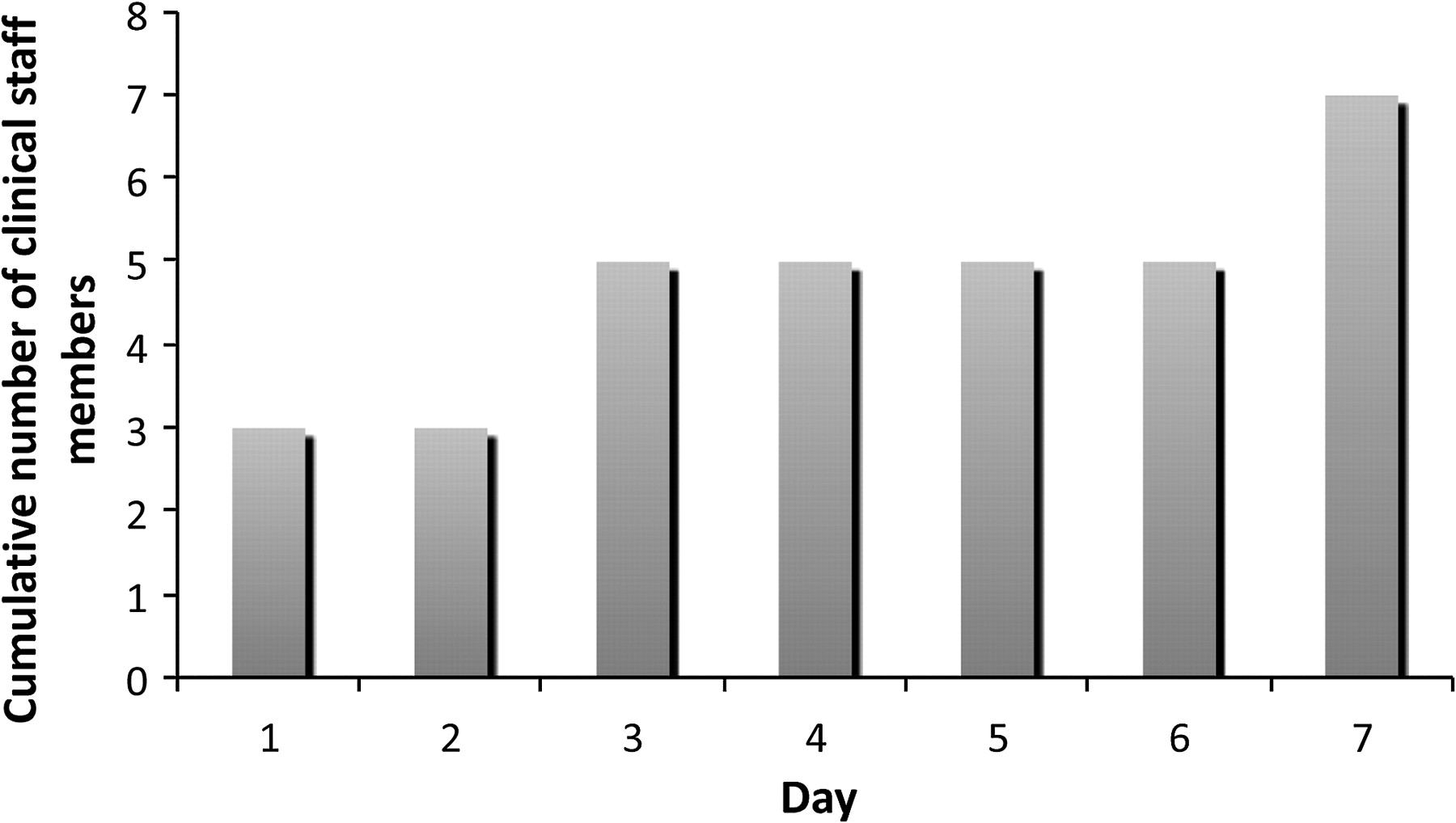
Affected staff were advised to remain off work for a week after the initial onset of their symptoms; 33 working days were subsequently lost due to illness. The cumulative number of staff members infected with H1N1 virus in our unit over a week from the time of first symptoms reported by a member of staff is shown (figure 1). During the same period, six patients on the ward also tested positive for H1N1 after developing flu-like symptoms. In two of these, H1N1 was likely to have been contracted while in hospital as they had been admitted several days earlier and were recovering from their presenting illnesses.
{kind=link}
Cumulative number of clinical staff in our unit with serological H1N1 influenza over a 7-day period.
Our experience has demonstrated that within the hospital environment, H1N1 is readily and rapidly transmissible between individuals. This outbreak highlights the importance of rapidly identifying infected patients and instituting source isolation procedures. Moreover, it is imperative that members of hospital staff use appropriate protection equipment and receive H1N1 immunisation (as recommended by the Department of Health) at the earliest opportunity. This should reduce the risk not only of healthcare workers contracting the virus from infected patients, but also of cross-infection between other patients and other healthcare workers. It is important that hospital trusts recognise the potential impact of H1N1 on frontline staffing and ensure appropriate contingency plans are made.
Reference
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; not externally peer reviewed.