Article Text

Statistics from Altmetric.com
P28 A MULTIDIMENSIONAL COMPOSITE SCORE USING NON-INVASIVE BASELINE VARIABLES TO PREDICT MORTALITY IN PATIENTS WITH PULMONARY ARTERIAL HYPERTENSION
W. N. Lee, S. Kerridge, A. J. Peacock, M. K. Johnson. Scottish Pulmonary Vascular Unit, Glasgow, UK
Introduction In order to facilitate decision making regarding treatment escalation and referral for lung transplantation in pulmonary arterial hypertension (PAH), an accurate way to predict prognosis is desirable.
Aim The aim of the study was to develop a composite score incorporating a number of prognostic non-invasive outcome variables measured at diagnosis to predict mortality in patients with PAH.
Methods Data from 331 patients diagnosed with inoperable chronic thromboembolic disease and PAH (excluding congenital heart disease) in the Scottish Pulmonary Vascular Unit from October 1996 to May 2009 were retrospectively reviewed. Univariate and multivariate logistic regression analysis was used to determine the association between age, gender, pulmonary function, pulmonary haemodynamics at right heart catheterisation, six-minute walk distance (6MWD), WHO functional class (FC), NTproBNP and CAMPHOR scores (on symptoms, activities and quality of life (QOL)) and mortality at 6 months, 1 year and 2 years. A composite score was derived including baseline values of 6MWD, WHO FC, NTproBNP and CAMPHOR QOL score. The weighting of each variable was adjusted using the coefficients of the logistic regression model. The predictive value of the composite score was assessed using ROC analysis.
Results The composite score is outlined in table 1. Patients with a composite score of ⩾7 had a higher mortality with a median survival of 468 days versus 1477 days in patients with a composite score of <7 (log rank, p<0.005). The area under the curve of the composite score was 0.88 (p<0.005) for 6-month mortality, 0.75 (p<0.05) for 1-year mortality and 0.73 (p<0.01) for 2-year mortality.
Definition of the composite score
Conclusions Using non-invasive baseline variables, we have derived a multidimensional composite score which appeared to predict mortality in our cohort of patients. Its usefulness needs to be validated prospectively before firm conclusions can be drawn.
P29 RELATIONSHIP BETWEEN MEAN AND SYSTOLIC PULMONARY ARTERY PRESSURE IN IDIOPATHIC PULMONARY HYPERTENSION, CONNECTIVE TISSUE DISEASE-ASSOCIATED PULMONARY HYPERTENSION AND CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION
S. F. Crawley, M. K. Johnson, A. J. Peacock. Scottish Pulmonary Vascular Unit (SPVU), Glasgow, UK
Introduction There is evidence from our laboratory and elsewhere to suggest that the relationship between systolic pulmonary artery pressure (sPAP) and mean pressure (mPAP) is tight enough to allow formulae for predicting the mPAP from sPAP. sPAP can be derived non-invasively by echocardiography whereas mPAP requires right heart catheterisation. Recently there has been concern whether the same formula can be used in all categories of pulmonary hypertension.
Aim The aim of the study was to examine the relationship between sPAP and mPAP in different categories of pulmonary hypertension.
Methods Right heart catheter data from 234 patients diagnosed with idiopathic pulmonary arterial hypertension (IPAH), connective tissue disease-associated pulmonary hypertension (CTDPH) and chronic thromboembolic pulmonary hypertension (CTEPH) in the Scottish Pulmonary Vascular Unit from January 2000 to May 2009 were retrospectively reviewed. The CTEPH group was further divided into proximal and distal CTEPH. Proximal CTEPH was defined as disease considered amenable to pulmonary thromboendarterectomy (PEA) by the National PEA centre at Papworth, UK. Distal CTEPH was disease considered unsuitable for PEA. Linear regression was used to generate equations predicting mPAP from sPAP.
Results All groups demonstrated a linear correlation between sPAP and mPAP: IPAH (n = 106) r2 = 0.89, p<0.0001; CTDPH (n = 63) r2 = 0.83, p<0.0001; CTEPH (n = 65) r2 = 0.76, p<0.0001. The relationship was similar in IPAH and CTDPH, but different in CTEPH: IPAH mPAP = 0.62 sPAP –0.6 mm Hg; CTDPH mPAP = 0.63s PAP –2.6 mm Hg whereas CTEPH mPAP = 0.49 sPAP + 5.8 mm Hg. Differences also existed between the proximal and distal CTEPH groups: proximal CTEPH (n = 42) mPAP = 0.45 sPAP + 7.8 mm Hg; distal CTEPH (n = 23) mPAP = 0.51 sPAP + 5.1 mm Hg.
Conclusions The relationship between sPAP and mPAP is similar in IPAH and CTDPH but is different in CTEPH. Existing equations to derive mPAP from sPAP in IPAH can be used confidently in CTDPH, but do not predict accurately mPAP in CTEPH. The different relationships observed in proximal and distal CTEPH support current opinion on the heterogeneity of these two groups, and further prospective evaluation is required to establish if they would be useful in identifying patients with disease amenable to PEA.
P30 PREDICTORS OF EARLY AND LATE MORTALITY IN ACUTE PULMONARY EMBOLISM
1A. Singanayagam, 1J. D. Chalmers, 2C. Scally, 2M. Z. Al-Khairalla, 2L. Leitch, 1A. T. Hill. 1Royal Infirmary of Edinburgh, Edinburgh, UK, 2Ninewells Hospital, Dundee, UK
Introduction Studies suggest that early mortality in pulmonary embolism (PE) is due to acute right ventricular dysfunction (RVD) and cardiogenic shock, while late mortality is largely related to co-morbid illnesses. We therefore hypothesised that biomarkers such as troponin (Tn) and a new scoring system described by the European Society of Cardiology (ESC) that incorporates Tn, RVD and haemodynamic instability may be more useful to identify patients at risk of early deterioration. The Pulmonary Embolism Severity Index (PESI) is an established severity score which is strongly influenced by age and co-morbidities and may be more useful to identify patients at risk of long-term mortality. The aim of this study was to investigate the predictive value of biomarkers and severity scores for early and late mortality in acute PE.
Methods A retrospective analysis of patients admitted with acute PE confirmed by CTPA to three teaching hospitals over a 2-year period. All patients had measurement of Tn and D-dimer and calculation of PESI score and ESC criteria on admission. The outcomes of interest were 7-day, 30-day and 90-day mortality. The area under the receiver operator characteristic curve (AUC) was used to assess performance of predictive tests.
Results 457 patients were included (median age 65, IQR 52–77). Co-morbidities were: 18.8% malignancy, 14.9% cardiac failure and 15.5% chronic lung disease. 3.9% of patients died within 7 days, 7.4% within 30 days and 10.3% within 90 days. The ESC criteria and Tn had good predictive value for early mortality but were less useful at predicting later mortality. PESI had moderate predictive value for all outcomes but appeared most useful for predicting late mortality. The predictive value (AUC) of biomarkers and severity scores for 7-day, 30-day and 90-day mortality are shown in table 1.
Predictive value (AUC) of admission variables for 7-day, 30-day and 90-day mortality
Conclusion Severity scores and biomarkers perform differently for prediction of mortality at early and later time points after admission with acute PE. This has important implications for use of these tools to guide early treatment strategies such as site of care and thrombolysis.
P31 COMPARISON OF OUTCOME FOLLOWING HEART/LUNG TRANSPLANTATION FOR CHRONIC THROMBOEMBOLIC PULMONARY HYPERTENSION AND IDIOPATHIC PULMONARY ARTERIAL HYPERTENSION
R. Venkateswaran, D. Jenkins, J. Dunning, S. Tsui, J. Wallwork, J. Parmar. Papworth Hospital, Cambridge, UK
Introduction Comparison of outcome following heart/lung transplantation (H/L Tx) performed for idiopathic pulmonary arterial hypertension (IPAH) and chronic thromboembolic pulmonary hypertension (CTEPH) is unknown. The objective of this study is to compare the outcome of H/L Tx performed for CTEPH and IPAH in a single institute.
Methods Between July 1984 and June 2009 a total of 330 H/L Tx were performed in our institute. The prospectively collected data on all patients undergoing H/L Tx for CTEPH and IPAH were analysed retrospectively. The recipient demographics, co-morbidities, donor data, CMV mismatch, operative details, duration of ventilation and intensive care unit stay, postoperative complications, freedom from bronchiolitis obliterans syndrome (BOS) and long-term survival were compared between the groups.
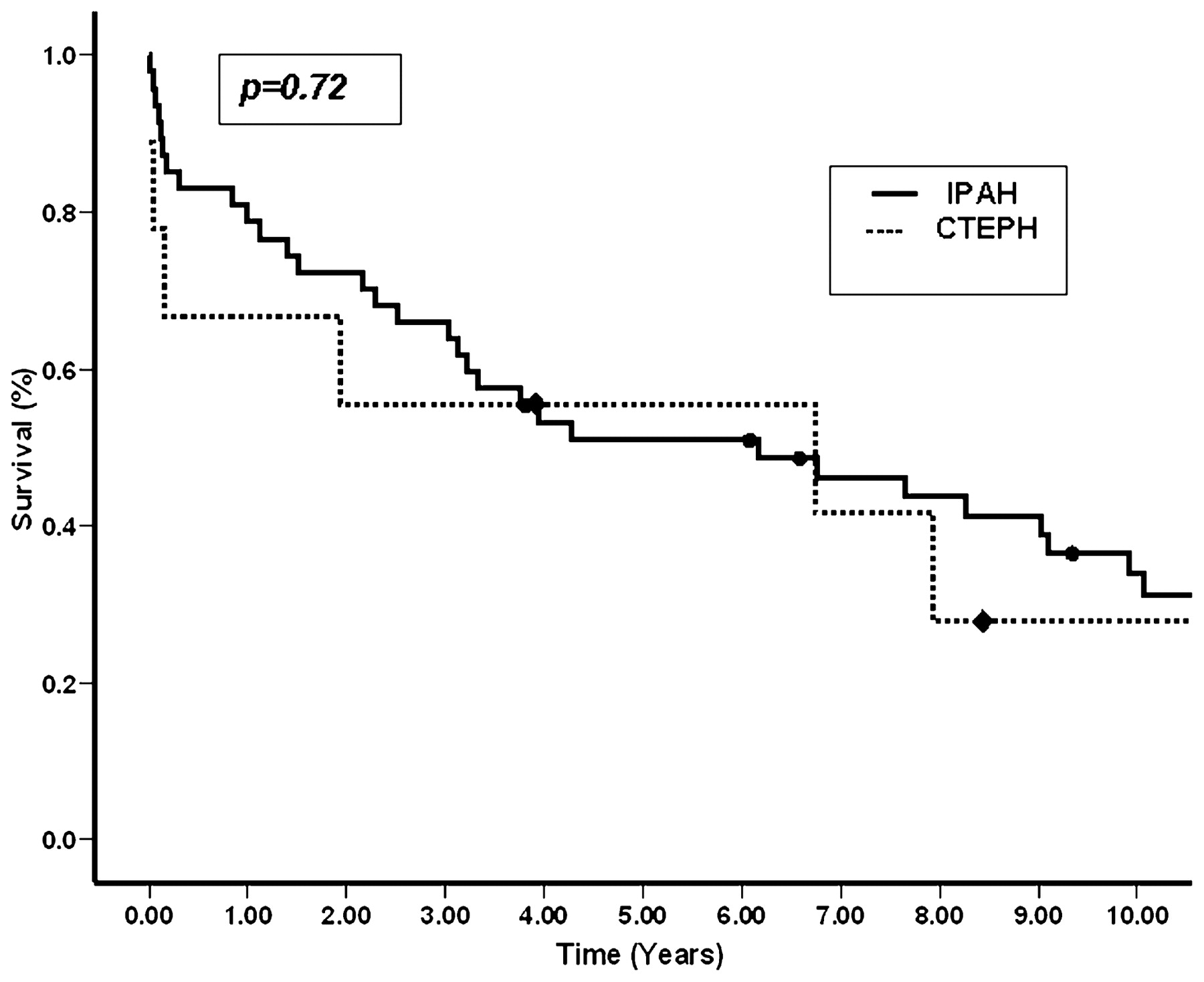
Results A total of 56/330 (17%) patients underwent H/L Tx for pulmonary vascular disease. Nine of the 56 patients (16%) had CTEPH and the remaining 47 (84%) had IPAH. The median duration of follow-up for the entire cohort was 1104 days (25th, 75th centiles 90, 2844). The baseline demographic factors were comparable between the groups except a significant female predominance in the IPAH group (p = 0.02). The 1-year and 5-year survival for the two groups were similar (fig). Postoperative episodes of acute rejection (p = 0.09), CMV mismatch (p = 0.72), fungal infection (p = 0.99) and freedom from BOS at 1 year (p = 0.28) were similar between the groups.

Conclusion Immediate and long-term outcome of H/L Tx performed for pulmonary vascular hypertension was similar irrespective of the aetiology. It remains a viable treatment option for end-stage irreversible pulmonary hypertension.
P32 INCIDENCE OF NON-DIAGNOSTIC CT PULMONARY ANGIOGRAPHY IMAGES IN THE PREGNANT POPULATION: A 4-YEAR EXPERIENCE
E. C. Potton, S. Marsh, C. Hasford. University College Hospital London, London, UK
Introduction and Objectives Venous thromboembolic (VTE) disease is the leading cause of maternal mortality during pregnancy and the puerperium.1 As VTE disease is highly treatable and has implications for future pregnancies, it is important to make a definitive diagnosis. A diagnostic pathway for pulmonary embolic disease in pregnancy has been a topic for debate and varies from hospital to hospital. There is relatively little evidence to guide physicians in the investigation of pulmonary emboli in pregnancy. CT pulmonary angiography (CTPA) has a non-diagnostic rate of 5–10% in the non-pregnant population due to breathing and motion artefact.2 There is some anecdotal evidence that pregnant patients may have a higher rate of non-diagnostic CTPA studies due to the hyperdynamic circulation.3 The rate of non-diagnostic scans is not well documented as there are no large series. This retrospective study documents the rate of non-diagnostic CTPA as a result of the hyperdynamic circulation in one centre over a 4-year period.
Methods Patients who underwent a CTPA during the period from June 2005 to June 2009 were identified from a radiology database. Data were collected retrospectively from patient files, electronic records and PACS radiology reporting system.
Results Of the 2292 patients who underwent a CTPA between June 2005 and June 2009, 34 patients were pregnant or within a 2-week postpartum period. Of these 34 CTPA examinations, 7 were reported by the radiologists as non-diagnostic due to the hyperdynamic circulation of pregnancy. All 7 patients underwent CTPA examinations in the third trimester and postpartum period. Four of the 7 patients underwent a further investigation; 2 were treated on clinical suspicion and 1 was reassessed and another cause for their symptoms was found.
Conclusions In this 4-year retrospective study in one centre there was a 20% rate of non-diagnostic CTPA examinations as a result of the hyperdynamic circulation. This highlights the urgent need for further multicentre studies and evidence-based protocols, as the disease is common and the consequences of correct or incorrect diagnosis considerable.
P33 CHANGING OUTCOMES IN DIFFERENT TYPES OF PULMONARY ARTERIAL HYPERTENSION
E. Soon, C. M. Treacy, M. R. Toshner, R. Mackenzie Ross, N. J. Doughty, K. K. Sheares, N. W. Morrell, J. Pepke-Zaba. Papworth Hospital NHS Foundation Trust, Cambridge, UK
Introduction Pulmonary arterial hypertension (PAH) has been associated with a poor prognosis. We sought to compare the survival of two cohorts diagnosed in 2001–3 and 2004–8 for three major aetiologies: distal chronic thromboembolic pulmonary hypertension (CTEPH), idiopathic pulmonary hypertension (IPAH) and PAH associated with congenital heart disease (CHD).
Methods All patients with incident PAH in 2001–8 belonging to one of the three aetiologies described were extracted from the database. Distal CTEPH cases were defined as de novo cases and did not include patients with proximal CTEPH rendered inoperable due to other reasons (eg, co-morbidities) or persistent PAH post-endarterectomy. Patients were divided into two cohorts based on the time period in which they were diagnosed. Their survival characteristics, demographics and treatments were compared for the two time periods described.
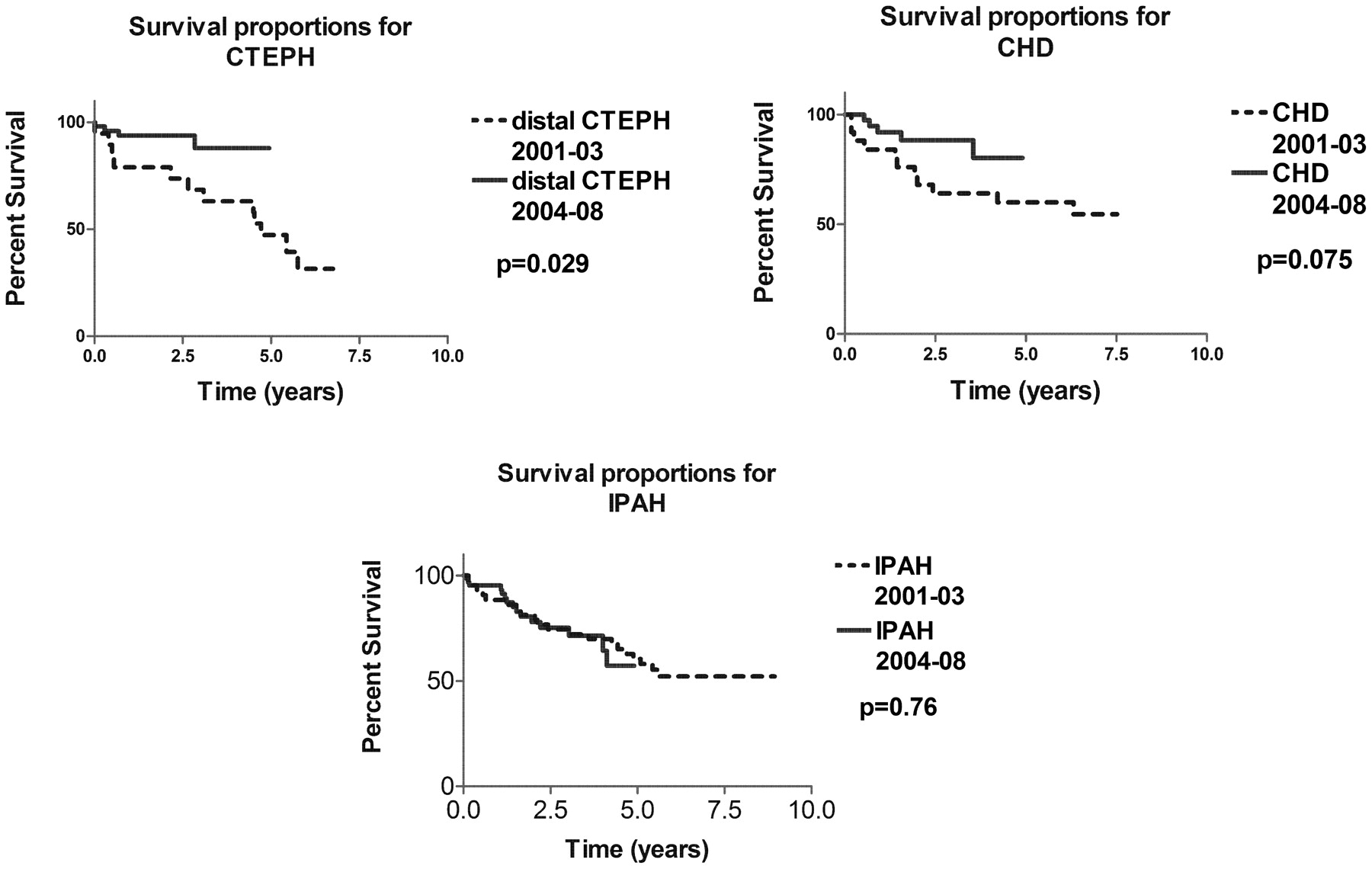
Results Survival was improved in the 2004–8 cohort of distal CTEPH compared with 2001–3, while there was a trend towards significance for patients with CHD. There has been no appreciable change in outcome for patients with IPAH (results summarised in fig 1). There were no significant differences in either the mean pulmonary artery pressures (mPAP) or pulmonary vascular resistances (PVR) at diagnosis when the CTEPH, IPAH and CHD cohorts diagnosed in 2001–3 were compared with the corresponding cohorts diagnosed in 2004–8. There were no significant changes in the gender distribution in the two time periods examined for any of the three types of PAH. A greater proportion of patients were using targeted therapies in the 2004–8 distal CTEPH cohort than in the 2001–3 group, but this did not reach significance, possibly because of the small numbers of patients (n = 50 and n = 19, respectively).

Comparison of survival curves for the 2001–3 and 2004–8 cohorts for different types of pulmonary arterial hypertension (PAH). CHD, congenital heart disease; CTEPH, chronic thromboembolic pulmonary hypertension; IPAH, idiopathic pulmonary hypertension.
Conclusions The survival of patients with distal CTEPH has improved significantly, while there is a trend towards improvement in CHD-associated PAH and outcome remains unchanged in IPAH. This may be due to increased use of targeted therapies.
P34 RELATIONSHIP BETWEEN MEAN AND SYSTOLIC PULMONARY ARTERY PRESSURES IN PULMONARY ARTERIAL HYPERTENSION
R. V. MacKenzie Ross, M. Toshner, E. Soon, J. Pepke-Zaba. Papworth Hospital NHS Foundation Trust, Cambridge, UK
Introduction The concept of using systolic pulmonary artery pressure (sPAP) to calculate the mean pulmonary artery pressure (mPAP) based on a fixed relationship is compelling.1 2 3 This makes non-invasive sPAP measurement a more useful tool. The pulmonary vascular waveform and pulse pressure in chronic thromboembolic pulmonary hypertension (CTEPH) has been shown to be different compared with other groups with pulmonary hypertension. We wondered whether the presence of large proximal thrombus would have the biggest effect on the sPAP to mPAP relationship and sought to test this with our patient population.
Method Pulmonary haemodynamics were taken from our database for patients from 1999 to 2008. To define proximal CTEPH we used only patients who achieved a reduction in mPAP to ⩽25 mm Hg following pulmonary endarterectomy (PTE). The data available allowed two proximal CTEPH groups to be studied. For the largest group we had data from measurements taken under anaesthetic at the time of PTE (PTE CTEPH). For a second smaller CTEPH group we had data from the time of diagnosis (Diagnosis CTEPH). Patients with idiopathic pulmonary hypertension (IPAH) and connective tissue disease-associated pulmonary hypertension (CTD) were used as a comparative group.
Results All groups demonstrated a linear correlation: IPAH (n = 42) r2 = 0.90; Diagnosis CTEPH (n = 42) r2 = 0.81; PTE CTEPH (n = 173), r2 = 0.80; CTD (n = 31), r2 = 0.82. The relationships differed: IPAH mPAP = 0.56 × sPAP + 3.3; Diagnosis CTEPH mPAP = 0.48*sPAP +5.2; PTE CTEPH mPAP = 0.47*sPAP +8.9; CTD mPAP = 0.54 × sPAP +5.0. There was a significant difference in the slopes between IPAH and PTE CTEPH (p<0.038, fig 1).

{kind=link}
{kind=link}
{kind=link}
Relationship between systolic pulmonary artery pressure (sPAP) and mean pulmonary artery pressure (mPAP). IPAH, idiopathic pulmonary hypertension; PTE, pulmonary endarterectomy.
Conclusions For IPAH and CTD our data are very similar to that published.1 2 For both proximal CTEPH groups (Diagnosis CTEPH and PTE CTEPH) we found the relationship between mPAP and sPAP was altered but remained linear. Unfortunately, this does not support the idea of a single fixed relationship between sPAP and mPAP in all forms of pulmonary hypertension.
Research supported by NIHR Cambridge Biomedical Research Centre.