Article Text

Statistics from Altmetric.com
S131 USE OF PROPORTION OF PATIENTS WITH COPD ADMITTED UNDER A RESPIRATORY SPECIALIST AS A MARKER OF COPD CARE
E. Thompson, P. P. Walker, G. Tack, H. Crone, G. Flatt, M. G. Pearson. Aintree Health Outcomes Partnership, University of Liverpool, Liverpool, UK
Patients with a chronic obstructive pulmonary disease (COPD) exacerbation are more likely to have blood gases recorded, receive corticosteroids and/or non-invasive ventilation (NIV), and access early discharge schemes if managed by specialists rather than generalists (Connolly, Thorax 2006). The 2008 National UK COPD Audit shows patients prefer to be cared for by a specialist. Hence, delivery of acute COPD care by a respiratory specialist presents a potentially important, measurable proxy of outcome.
Hospital Episode Statistics (HES) data detail every COPD hospital admission and record a variety of related outcomes. Separately we have created a database of GMC numbers of 821 respiratory specialists (missing only 5 from the BTS workforce book) and matched this to HES. From this we calculated the percentage of admissions under respiratory specialist care for 149 English Trusts during 2006–7 and 2007–8. We went on to examine the potential of this to represent an indicator of quality of care.
In 2006–7, 51 107 out of 128 184 (40%) COPD admissions were discharged from respiratory specialists. The total for 2007–8 was 49 114/126 695 (39%). Comparing Trusts, there existed a wide variation in the percentage of patients admitted under a respiratory specialist—2006–7 median 38.6% (interquartile range (IQR) 28.8–49%); 2007–8 median 37.2% (IQR 29.5–48.4%)—allowing considerable room for improvement. This percentage for each Trust varied little between years (r = 0.84; p<0.001)—shown in fig 1—probably reflecting the organisation of the acute “take”. However, there was no relationship between specialist care and either annual number of admissions per Trust, mean length of stay or 30-day mortality, these outcomes presumably being complex and influenced by multiple factors.
Most COPD admissions are not managed by specialists, but there is a wide inter-Trust variability, suggesting very different triage processes exist. If the audit data are accepted, then this may be a useful quality indicator of the hospital organisation and thus care offered for patients with COPD.

S132 COULD THE AVERAGE “TOTAL BED DAYS PER PATIENT” BE AN INDICATOR OF COMBINED HOSPITAL AND COMMUNITY CARE?
G. Tack, P. P. Walker, E. Thompson, H. Crone, G. Flatt, M. G. Pearson. Aintree Health Outcomes Partnership, University of Liverpool, Liverpool, UK
A principle aim of chronic obstructive pulmonary disease (COPD) care is to keep patients out of hospital—that is, reduce admissions and readmissions. This depends on both community and hospital practices. These factors are hard to interpret individually but can be combined in a single measure—the total number of bed days per individual in 1 year.
Hospital Episode Statistics (HES) provide data on the number and length of each admission and can be linked to an individual. We expressed COPD total bed days per 1000 Primary Care Trust (PCT) population, then controlled for age (by comparison with the national data in 5 year age cohorts) and for smoking (by using the standardised mortality ratio (SMR) for lung cancer derived from cancer registry data). The latter provided an indirect control for local smoking prevalence.
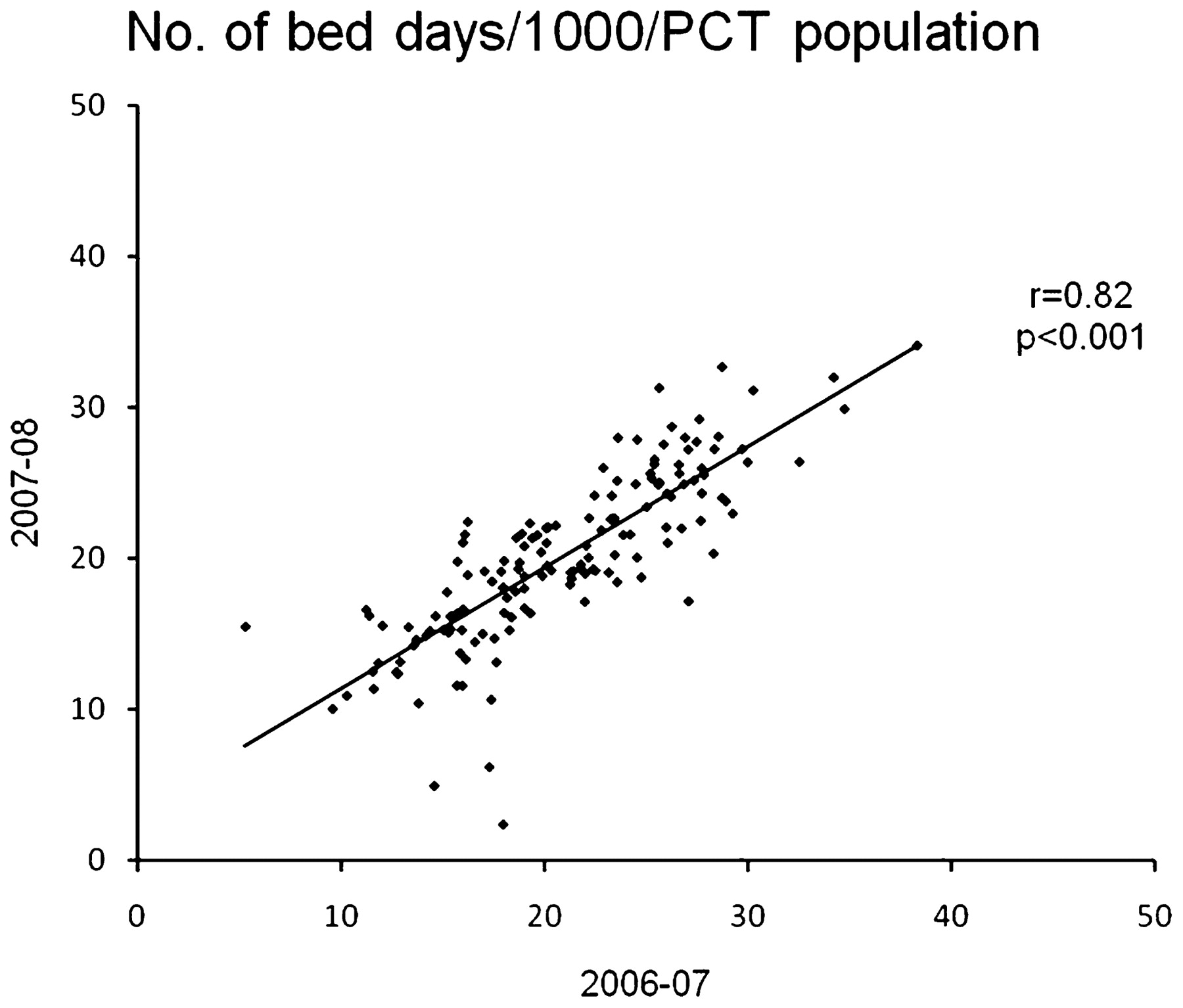
We identified 128 184 COPD admissions in 85 606 patients in 2006–07 and 126 695 admissions in 86 037 patients in 2007–08. Mean (SD) age was 72 (11) years and 49% were male. Mean bed days/1000 PCT population in 2006–07 was 22.8 (SD 9.7) days and in 2007–08 was 21.9 (SD 9.2) days. This wide range is significantly reduced by control for smoking prevalence, with the SD falling to 5.8 and 5.6, respectively. The values within PCTs were strongly correlated year on year (r = 0.82, p<0.001) and were independent of the size of the PCT; see fig 1. Even after control for age and smoking, a quarter of PCTs exceeded 24.5 and 24.2 days, respectively, and a quarter had <16.2 and 16.3 days, respectively, over the 2 years, suggesting there is potential for reducing the overall hospitalisation of patients with COPD. This fits with the National COPD Resources and Outcomes Project (NCROP) audit observation that only 142/239 (59%) Trusts operated early discharge policies.
Total bed days per patient may be a useful indicator of the combined hospital and community quality of care for patients with COPD.

PCT, Primary Care Trust.
S133 JOINED UP THINKING: CONCEPT OF A LUNG/RHEUMATOLOGY MDT IN A DGH SETTING
1P. Huey, 1C. Adams, 1Y. Ahmed, 2D. J. McKeon. 1Ysbyty Gwynedd, Bangor, UK, 2Faculty of Medical Sciences, Bangor University, Bangor, UK
Introduction and Objectives The benefits from delivering healthcare in a coordinated multidisciplinary team (MDT) have long been established in the treatment of cancer. These expert forums allow for the provision of the most up-to-date and relevant treatment options for individual patients. Connective tissue diseases (CTDs) are a group of complex multisystem disorders that often affect the lung. Both rheumatologists and pulmonologists can find treating these diseases in isolation difficult and challenging. We have taken a novel MDT approach involving expertise from a wide variety of disciplines including pulmonology, rheumatology, pharmacy, physiology, immunology and radiology to improve the treatment of these patients.
Method Regular 2 monthly MDTs were organised over a 12-month period and patients were discussed, with their radiology, physiology and immunology also presented. The cohort of patients included those suffering from CTDs with pulmonary complications as well as patients with primary pulmonary pathology with either clinical or immunological features suggesting an underlying CTD. There was also an overlap group of patients who were under investigation for the pulmonary complications of immunosuppressive medication.
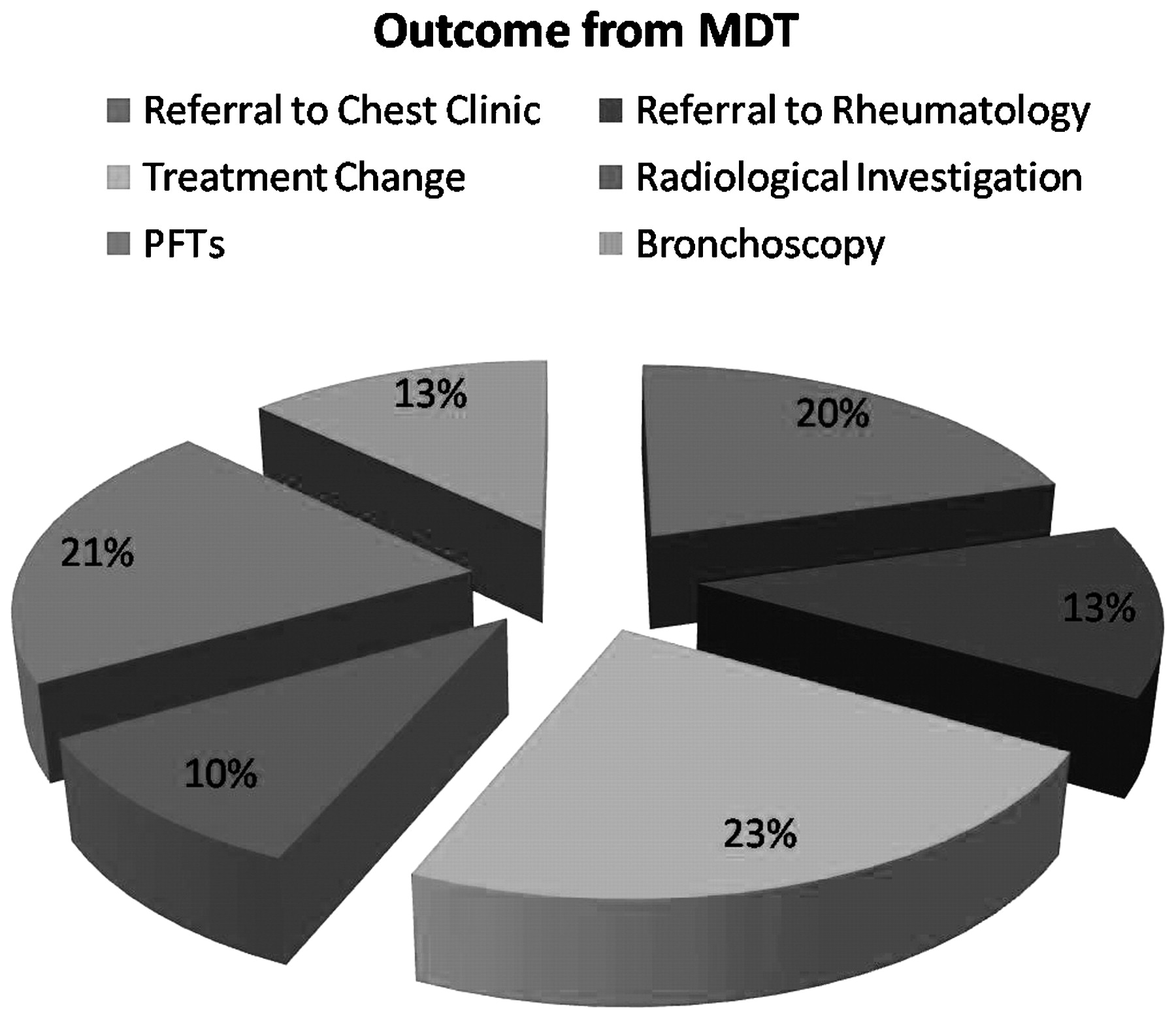
Results The demographic data demonstrate that 22 patients (17 female, 5 male) were discussed over an 12-month period. The most common reason for presentation was the pulmonary complications of rheumatoid arthritis (n = 9). Other diseases included pulmonary complications of scleroderma (n = 5), sarcoidosis (n = 3) and the other CTDs including Wegner granulomatosis (n = 5). The outcomes of the MDT (see fig 1) were direct cross-referral from Rheumatology to Chest clinic (n = 8) and vice versa (n = 5). Changes in treatment included escalation of immunosuppressant (n = 9). Other outcomes included further referral to diagnostics (radiology, n = 4), pulmonary function (n = 8) or for bronchoscopic procedures including transbronchial biopsy (n = 5).
Conclusion Traditionally patient care is centred on distinct specialties working in isolated silos. CTDs par excellence are a group of disorders that defy this model and by their nature demand a more universal approach. We have demonstrated that by coordinating healthcare provision through an MDT model and bringing distinct specialties together, patient care is improved. We propose this model should be adopted in both tertiary institutions and District General Hospitals.
{kind=link}
{kind=link}
{kind=link}
MDT, multidisciplinary team; PFT, pulmonary function tests.
S134 A STORY WITH NO BEGINNING AND AN ILL-DEFINED END: A SERIAL QUALITATIVE STUDY OF END-STAGE COPD
1H. J. Pinnock, 1M. Kendall, 1A. Worth, 1A. Sheikh, 1M. Porter, 1W. MacNee, 2P. Levack, 1S. Murray. 1University of Edinburgh, Edinburgh, UK, 2Tayside Primary Care Trust, Dundee, UK
Background Palliative care services are extending to meet the needs of people with non-malignant disease, often extrapolating models of care originally designed to meet the needs of patients dying with cancer.
Methods We undertook serial in-depth interviews with people with severe chronic obstructive pulmonary disease (COPD) and their nominated informal and professional carers to identify the end-of-life needs in the context of the story of their illness. Interviews were transcribed and analysed using thematic and narrative analysis.
Results 21 patients, 12 carers and 16 professionals provided a total of 82 interviews over 18 months. 11 patients died during the study. In contrast to cancer narratives, the “story” of people with COPD lacked a clear beginning, was impossible to distinguish from their life story and had an ill-defined unpredictable end. Severe symptoms causing major disruption to normal life were described, but often in terms implying acceptance of the situation as a “way of life” rather than an “illness”. Deprived social circumstances, which many patients seemed unable to influence, contributed substantially to suffering. The insidious progression of symptoms due to a lifetime of smoking made it impossible for patients to describe the beginning of their COPD, and contributed to clinicians’ difficulty defining end-stage disease and the point of transition to palliative care.
Conclusion Acceptance of COPD as “a way of life” by patients has important implications for clinical care. The policy focus on identifying a time point for inclusion on a palliative care register has little resonance for people with COPD or their clinicians, and is potentially counterproductive if it distracts from early provision of supportive care.
Funding: Chief Scientist’s Office, Scottish Government. HP is supported by a PCRCA from the Chief Scientist’s Office, Scottish Government