Article Text

Statistics from Altmetric.com
S129 LENGTH OF STAY AS AN INDICATOR OF THE EFFICIENCY OF HOSPITAL CARE FOR COPD
G. Tack, P. P. Walker, E. Thompson, H. Crone, G. Flatt, M. G. Pearson. Aintree Health Outcomes Partnership, University of Liverpool, Liverpool, UK
Chronic obstructive pulmonary disease (COPD) is the second most common reason for emergency medical admission. The National COPD Resources and Outcomes Project (NCROP) audit in 2003 and 2008 showed that length of stay (LOS) varies widely, and National Institute for Health and Clinical Excellence (NICE) guidelines suggest that early discharge schemes offer opportunities to reduce the burden.
We used the Hospital Episode Statistics (HES) to identify all patients admitted with a COPD exacerbation to 149 English acute Trusts in 2006–7 and 2007–8. We analysed whole admissions not episodes. LOS rises in a non-linear fashion with age, so we controlled for age by comparing each admission LOS with that expected for each 5-year age cohort and expressed it as relative LOS (observed minus expected) for each Trust. We then controlled for the overall deprivation index associated with the patients attending that Trust.
There were 128 184 patients with COPD in the 2006–7 and 126 695 in 2007–08. Mean (SD) age was 72 (11) years, 49% male. Median (interquartile range (IQR)) LOS in the 2006–7 data was 8.4 (7.6, 9.3) days and in 2007–8 median (IQR) LOS was 8.4 (7.5, 9.2) days. Even after age and deprivation control some Trusts were 50% longer in LOS than others and this was independent of hospital size. Correlation between hospitals over the 2 years was consistent (r = 0.84; p<0.001); see fig 1. There was also consistency in that hospitals with shorter LOS in under 65s tended to have shorter stays for over 75s, (r = 0.58; p<0.001) and hospitals with long LOS in respiratory disease had longer LOS in gastroenterology (r = 0.48; p<0.001).
Longer LOS cannot be blamed on age or deprivation, and we suggest that the processes leading to longer LOS may be the result of the systemic organisation within a Trust and thus be an indicator of the efficiency of care.

LOS, length of stay.
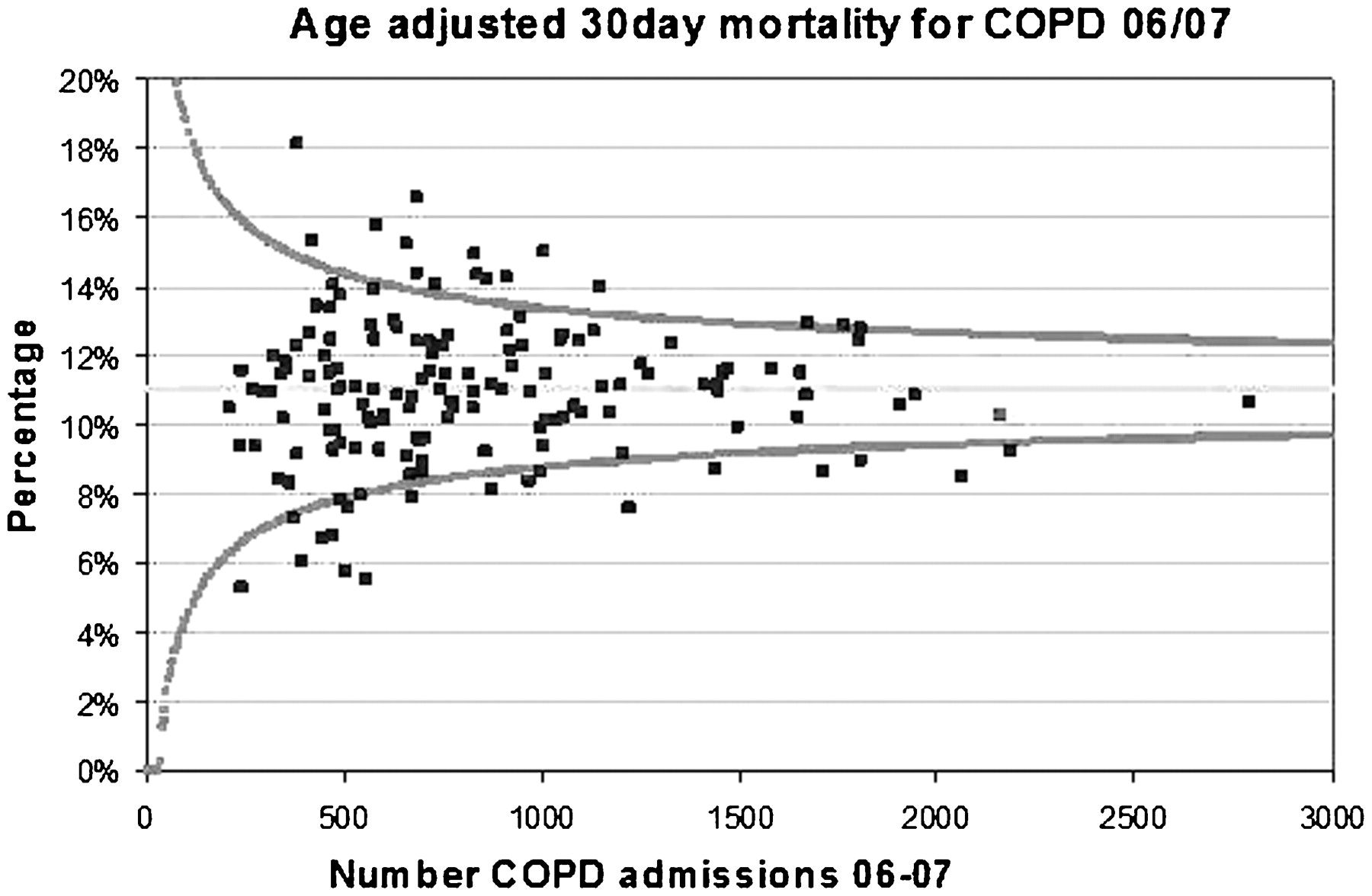
S130 USE OF 30-DAY MORTALITY AFTER INPATIENT ADMISSION AS A QUALITY MARKER OF COPD CARE
P. P. Walker, G. Tack, E. Thompson, H. Crone, G. Flatt, M. G. Pearson. Aintree Health Outcomes Partnership, University of Liverpool, Liverpool, UK
Death associated with a chronic obstructive pulmonary disease (COPD) exacerbation is common and is inarguably an important clinical outcome. The 2003 National COPD Resources and Outcomes Project audit showed that there was wide variability between Trusts and that lower mortality was associated with better organised care and more consultants. The 2008 audit confirmed that 90-day mortality after a COPD exacerbation remained high at 13.9%. Hospital Episode Statistics (HES) data, derived from inpatient coding, define every COPD admission and can be linked to Office for National Statistics (ONS) data to determine 30-day mortality after each admission over a full year. ONS mortality data avoid internal coding variability within trusts and differential discharge patterns. After age correction, 30-day “observed minus expected” mortality data were determined for each Trust during 2006–7 and 2007–8 and then expressed as a percentage of COPD admissions.
During 2006–7 median relative 30-day mortality rate across 149 Trusts was 11% (interquartile range (IQR) 9.7–12.6%). The figure for 2007–8 was 11.4% (IQR 9.5–12.9%). There was considerable variation between Trusts (illustrated in fig 1 as a funnel plot using 2006–7 data) in some cases with mortality varying more than twofold. There is a modest relationship between individual Trust mortality when the two years are compared (r = 0.52; p<0.001), suggesting that while disease severity is important, both organisation and delivery of care also impact upon mortality. Nineteen Trusts have a mortality level in the highest quartile during both years, while in 17 Trusts mortality is in the lowest quartile during both years. When data are split into quartiles there are clues that support the findings of the 2008 National Audit which suggested that larger trusts had better organisation and lower mortality.
Much COPD mortality is an inevitable consequence of the disease process, but the variability between Trusts suggests that 30-day mortality after a COPD admission may represents a potential quality indicator of hospital delivery of care.
{kind=link}
{kind=link}
COPD, chronic obstructive pulmonary disease.