Article Text

Statistics from Altmetric.com
S94 CYSTIC FIBROSIS NEWBORN SCREENING: THE CASE FOR INVASIVE SURVEILLANCE AFTER DIAGNOSIS
P. Stafler, J. C. Davies, I. M. Balfour-Lynn, M. Rosenthal, A. Bush. Royal Brompton Hospital, London, UK
Introduction and Objectives Cystic fibrosis (CF) newborn screening (NBS) raised the issue of how to manage asymptomatic infants. There is evidence of early functional, structural and pathological changes, and even bronchiectasis in babies with CF diagnosed by NBS. We have previously shown a high prevalence of unsuspected lower airway infection in newly diagnosed, unscreened children with CF. The aim of this study was to determine the yield of bronchoalveolar lavage (BAL) microbiology/cytology and 24-hour pH monitoring in a group of NBS-diagnosed infants.
Methods Infants with CF diagnosed by NBS between July 2007 and July 2009 underwent surveillance fibre-optic bronchoscopy (FOB), BAL and 24-hour dual-probe pH monitoring. All the invasive procedures were performed under the same general anaesthetic.
Results Full data sets were available for 19 infants, median age 3 months (47–193 days) at the time of FOB. In 6 out of 19 (32%) at least one bacterial organism was identified on BAL. None of the patients was symptomatic at the time of FOB. Cough swabs taken at various time points (8–77 days) prior to FOB were all negative. Organisms identified were Haemophilus influenzae (n = 3), Staphylococcus aureus (n = 2), methicillin-resistant S aureus (MRSA) (n = 1), Pseudomonas aeruginosa (n = 1) and Moraxella catarrhalis (n = 1). All led to a change in antibiotics. Five of 16 (31%) had neutrophilia (median 11.4%, range 0.3–73%). Nine of 17 (53%) had an abnormal pH study with a pH index ⩾12. Only 2 of those 9 patients (22%) had a clinical diagnosis of gastro-oesophageal reflux prior to pH study.
Conclusions The high yield of microbiology, cytology and pH probe investigations in infants subjected to NBS justifies invasive surveillance FOB. Longitudinal studies to determine if early aggressive treatment results in improved outcome are awaited.
S95 EFFECT OF EXERCISE ON LARGE ARTERY HAEMODYNAMICS IN CYSTIC FIBROSIS
1J. H. Hull, 2L. Ansley, 3C. E. Bolton, 4J. E. Sharman, 5R. K. Knight, 3J. R. Cockcroft, 3D. J. Shale, 1R. Garrod. 1St Georges, London, UK, 2University of Northumbria, Newcastle, UK, 3Cardiff University, Cardiff, UK, 4University of Tasmania, Hobart, Australia, 5Frimley Park Hospital, Frimley, UK
Introduction and Objectives Improved longevity in cystic fibrosis (CF) has prompted increased focus on extrapulmonary manifestations. Adults with CF have evidence of abnormal large artery haemodynamics at rest; however, improved insight into the function of the cardiovascular system can be obtained by evaluating response in exercise. We hypothesised that adult patients with CF would have a maladaptive haemodynamic response to exercise, as evidenced by increased indices of myocardial loading, in comparison with controls.
Methods We studied 36 patients with stable CF (n = 11 with CF-related diabetes (CFRD)), mean (SD) age 28.9 (9.0) years, body mass index (BMI) 23.0 (3.1) kg/m2, forced expiratory volume in 1 s (FEV1) % predicted 65.8% (21.3%) and 25 age/gender/BMI-matched healthy controls. Large artery haemodynamics, including blood pressure (BP), augmentation index (AIx) and augmented pressure (AP), were determined by applanation tonometry (SphygmoCor) at rest, during (at 8 min) and following a 10 min period of cycle ergometry at 60% age-predicted maximal heart rate (HR). The extra myocardial oxygen requirement to overcome central pressure augmentation was calculated as wasted left ventricular pressure energy (ΔEW). Cardiac output (bioreactance) and peripheral vascular resistance (PVR) were determined at rest and postexercise. Lung function, log10 interleukin-6 (IL-6) and habitual physical activity levels were determined.
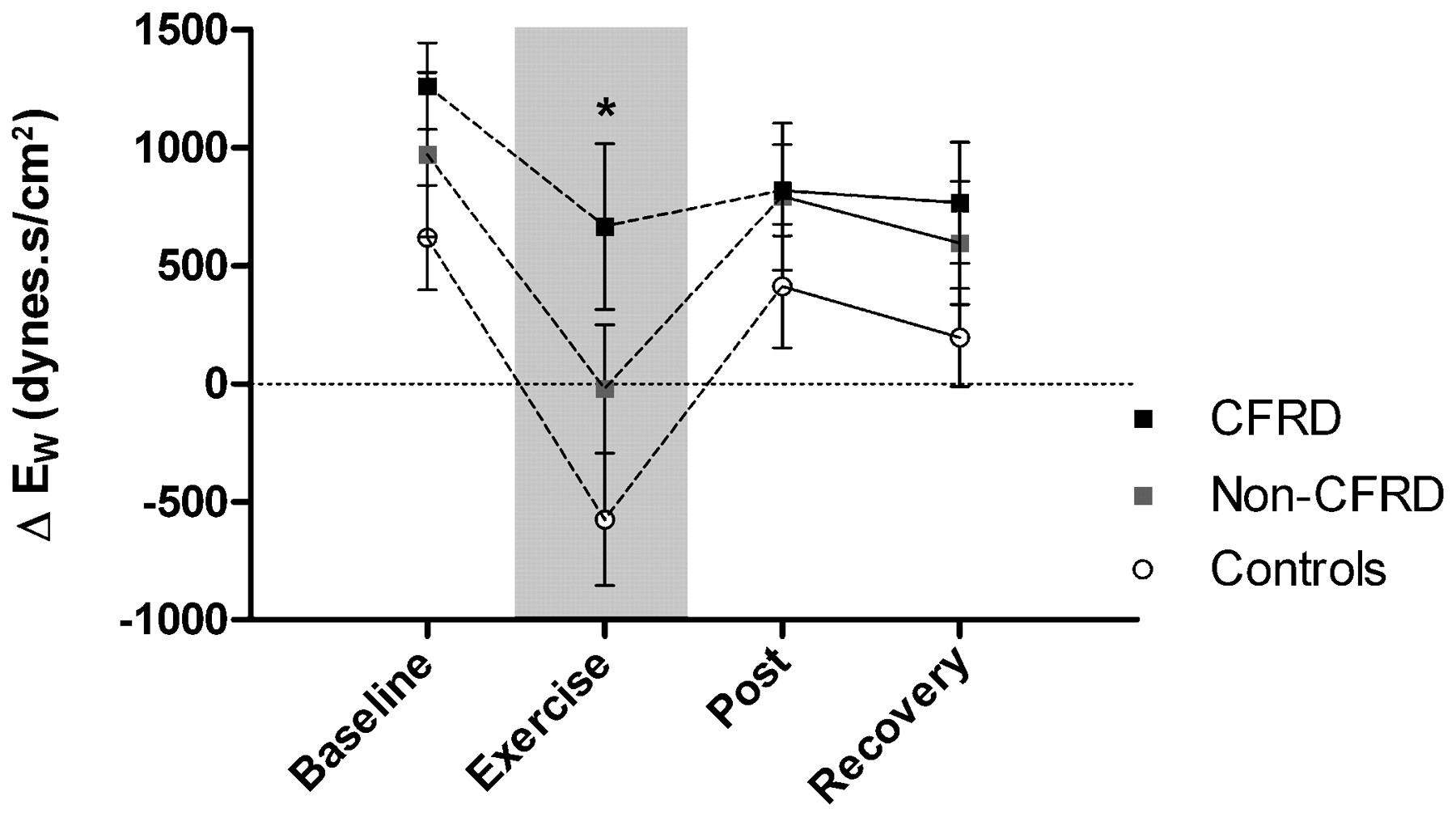
Results At rest, AIx was greater in both patients with and without CFRD than in controls. During exercise, despite a similar absolute HR and peripheral BP, patients with CFRD had greater mean arterial pressure, AP and ΔEW (fig 1) (p<0.05 for all) and a trend for greater AIx (p = 0.07). None of these indices was different from those of the controls in patients without CFRD (p>0.05 for all). Habitual physical activity was similar between groups, whilst log10IL-6 was increased in patients (p<0.001); both log10IL-6 and exercise ΔEW were greatest in patients with CFRD (both p<0.05). In all subjects, PVR was reduced postexercise from rest but was comparatively greater at all times in patients with CFRD than in controls (p<0.01).
Conclusions Haemodynamic response to exercise is similar between patients without CFRD and healthy controls. In contrast, patients with CFRD have increased central systolic stress during exercise, which has implications for myocardial work and oxygen demand. Further studies to explore long-term consequences for cardiovascular health and exercise capacity are required.
{kind=link}
Exercise-related changes in wasted left ventricular pressure energy (ΔEW). Symbols represent the mean with error bars±1 SEM. CFRD, cystic fibrosis-related diabetes. *p<0.05; CFRD difference from controls.
S96 GASTRO-OESOPHAGEAL REFLUX AND COUGH IN PATIENTS WITH CYSTIC FIBROSIS
1J. E. McCreanor, 1I. D. Molyneux, 2S. Faruqi, 1W. Jackson, 1J. O’Donnell, 1P. Sedman, 2A. H. Morice. 1Hull and East Yorkshire Hospitals NHS Trust, Hull, UK, 2University of Hull, Hull, UK
Introduction and Objectives Gastro-oesophageal reflux (GOR) is one of the most common aetiologies of chronic cough. There is a high incidence of symptomatic GOR in patients with cystic fibrosis (CF). We hypothesised that patients with CF might have abnormal oesophageal physiology.
Methods 24-hour ambulatory oesophageal pH monitoring and oesophageal manometry was undertaken in patients with CF with a clinical diagnosis of reflux-associated cough. We used a control group of DeMeester score-matched patients with reflux-associated cough without CF. The findings of the pH and manometry studies were analysed and comparisons were made between the groups.
Results 17 patients with CF (11 males, median age 28 years) and 17 patients with non-CF reflux-associated cough (10 males, median age 47 years) were included. Resting lower oesophageal sphincter (LOS) pressure was subnormal (<15 mm Hg) in 16 of 17 patients with CF (mean 10.4 mm Hg, SD 4.2). 13 had raised DeMeester scores (mean 33.0, SD 19.3). This was associated with a high number of transient lower oesophageal sphincter relaxation (TLOSR) episodes (mean 123.8, SD 40.3). Increasing frequency of TLOSRs correlated with increasing DeMeester score (coefficient 0.44). Patients with a LOS pressure ⩽8 mm Hg had a significantly greater DeMeester score (median 38.7, range 25–78) than those with >8 mm Hg (median 24.1, range 12–46) p<0.015. There was no statistically significant difference in resting LOS pressure (mean 10.35 vs 11.35; p = 0.21), percentage of peristaltic swallows (84.7% vs 72.4%; p = 0.13) or TLOSR episodes (123.8 vs 145.6; p = 0.17) between the CF group and controls. Time spent with oesophageal pH <4.0 was significantly greater in the CF group overall despite DeMeester matching (p<0.04).
Conclusion These results confirm the presence of acid reflux as a typical finding in patients with CF with a history of reflux cough. Furthermore, there may be a characteristic physiological abnormality in patients with CF with high frequency of TLOSR and increased oesophageal acidification.
S97 ASSESSMENT OF DIAPHRAGM FATIGUE FOLLOWING HIGH INTENSITY EXERCISE IN PATIENTS WITH CYSTIC FIBROSIS
1C. Reilly, 1K. Ward, 1L. Frank, 1C. Jolley, 1A. Lunt, 1J. Steier, 2C. Elston, 1G. F. Rafferty, 1J. Moxham. 1King’s College London, London, UK, 2King’s College Hospital, London, UK
Introduction There is an increased load placed on the respiratory muscles in cystic fibrosis (CF). Whether this predisposes the diaphragm to fatigue following exercise is unknown. The aim of this study was to examine whether patients with CF develop low frequency fatigue of the diaphragm after cycle exercise to exhaustion.
Methods Six male patients (median (range) age 22 (20–33) years) with CF (forced expiratory volume in 1 s (FEV1) % predicted 50% (31–80%)) were studied. The study was conducted on two occasions, 1 week apart. The first visit, to determine each subjects’ maximum work load (Wmax) and peak oxygen consumption (VO2peak), involved an incremental exercise test to exhaustion on a cycle ergometer. On the second visit patients performed an endurance exercise test above 80% of their predetermined Wmax at a constant pedal rate (50–60 rpm) to exhaustion. Twitch transdiaphragmatic pressure (TwPdi), elicited by bilateral anterolateral magnetic phrenic nerve stimulation (BAMPS), to assess the presence of low frequency fatigue, was measured before and at 20, 40 and 60 min postexercise.
Results Endurance exercise duration was 10.5 min (6–20) achieving 110% (100–121) of VO2peak. There were no significant differences in TwPdi at any time point postexercise compared with baseline (median (range) TwPdi 25.0 cm H2O (16.0–46.0) at baseline, 26.5 cm H2O (17.5–44.0) at 20 min, 26 cm H2O (17.5–44.0) at 40 min and 26.0 cm H2O (16.0–43.0) at 60 min postexercise (p<0.005)).
Conclusion Patients with CF do not develop low frequency fatigue of the diaphragm after high intensity, exhaustive constant load cycle exercise.
S98 THE USE AND PERCEIVED BENEFITS OF NON-INVASIVE VENTILATION FOR HYPERCAPNIC ADULTS WITH CYSTIC FIBROSIS IN A REGIONAL CENTRE
J. Barrett, P. Agostini, S. Cameron, E. Nash, J. Whitehouse, D. Honeybourne. West midlands regional adult Cystic fibrosis centre. Birmingham Heartlands Hospital, Birmingham, UK
Introduction Non-invasive ventilation (NIV) improves gaseous exchange and aids secretion clearance in patients with cystic fibrosis (CF). A recent study demonstrated that NIV improved chest symptoms and exercise tolerance, and reduced maximal nocturnal CO2 levels in this patient group. The objectives of this study were to examine the reasons for NIV initiation, and the perceived benefit in adults with CF with hypercapnia.
Method We conducted a retrospective observational study of adult patients treated with NIV during admission to a regional CF centre over an 18-month period. We recorded indication for treatment, perceived benefit in terms of work of breathing, symptoms of hypercapnia (early morning headache) and sputum clearance. Patient tolerance of NIV was also noted.
Results 19 patients, 5 of which were on the active lung transplantation list, were treated with NIV over 34 episodes during the 18-month period. Mean percentage predicted forced expiratory volume in 1 s (FEV1) on admission was 22% (range 10–53%) and 10 patients were female. Seven (20%) NIV episodes were initiated for treatment of decompensated respiratory acidosis, 24 (71%) episodes were in patients with compensated hypercapnic respiratory failure and in 3 (9%) episodes NIV was used exclusively as an adjunct to airway clearance. In patients with decompensated respiratory acidosis, NIV use resulted in a reduction in PaCO2, from 11.4±6.1 kPa to 6.25 ±2.2 kPa (mean±SD, p = 0.2) and an increase in pH, from 7.26±0.14 to 7.49±0.12 (p<0.04). In 68% of episodes the patient was discharged from hospital (n = 23), 16 with domiciliary NIV and 7 without NIV. 89% (n = 17) of patients reported subjective benefits from the NIV, including decreased work of breathing (n = 8), decreased hypercapnic symptoms (n = 5) and improved sputum clearance (n = 4).
Conclusion NIV was used successfully to treat and control symptoms of hypercapnic respiratory failure and was generally well tolerated, with a number of subjective benefits reported by patients.